
Abstract
Keywords
Introduction
The incidence of periprosthetic femoral fractures (PFFs) has been reported to be between 1% and 11% over a primary and up to 18% over a revised hip femoral stem.1-5 The ever-expanding indications for total hip arthroplasty (THA) are leading to more implants being placed in younger as well as in older patients with high functional demand. Prolonged life expectancy, combined with this increase in number of performed arthroplasties, is contributing to an overall increment of PFFs. The Vancouver classification was proposed in 1995 by Duncan and Masri 6 and since then it has been the most used for guiding the surgeon choice.7-10 It has been recently expanded and integrated into the Unified Classification System for Periprosthetic Fractures (UCS-PF).11,12 Specific patterns of fracture has also been described for PFFs, with different prevalence over uncemented or cemented stem and apparently over stem design.13-18 Also, atypical patterns have been described and periprosthetic atypical femoral fractures (PAFFs) are now accepted to exist.19-21 Historically, the treatment of PFFs has been associated with a high rate of complications, poor outcomes and the need for further surgery. 22 These fractures can cause frequent and severe comorbidities in elderly patients: multiple studies showed people older than 85 years had poor functional outcomes, greater loss in the ability to perform activities of daily living, and increases of the risk mortality after a PFF.23,24
PFFs occurring over a THA can be divided into intra-operative and post-operative PFFs. Intra-operative fractures are estimated to occur in less than 1% of cemented and in 5.4% of uncemented primary THA, while in revision surgery the incidence of PFFs is higher, up to 3.6% during cemented and 20.9% during uncemented procedures. 25
Post-operative PFFs may be associated with stem loosening, with or without concomitant osteolysis, 26 and usually they occur with low energy trauma.1,27 Their incidence has been estimated to be less than 1% after primary THA and up to 4% following revision THA.25,28 Lindahl et al found that the annual incidence of post-operative PFFs varied between .045% and .13% for all THAs recorded in the Swedish National Hip Register between 1979 and 2000, 1 while the cumulative risk of PFFs ranges from .4 to 2.53%. 29 These fractures can vary from minor injuries with a minimal effect on patient functionality to catastrophic injuries requiring major reconstruction. 30
The treatment of PFFs depends on 5 important factors: level of fracture, stability of the implant and of the fracture, quality and quantity of bone stock, patient’s factors (as age, comorbidities and functional demands), and surgeon experience.2,10,22,31-33 The aim of this review is to describe state-of-the-art treatment in the management of PFFs, and to propose a summary to guide treatment choice.
Materials and Methods
A systematic literature review of studies reporting on the management of PFFs around hip stems was performed according to Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines. 34 Two researchers independently searched the MEDLINE and Scholar databases to retrieve articles published from inception to April 2021. The language was restricted to English. The terms used were as follows: (periprosthetic femoral fractures) AND (management OR treatment). Reference lists of related papers were also manually searched for potential eligible studies that were included when meeting the inclusion criteria.
Studies that contained relevant information about the management of PFFs after THA or hemiarthroplasty were included. Exclusion criteria were infections, periprosthetic fractures around TKA, and acetabular fractures. Two authors independently screened the titles and abstracts and eliminated duplicates. Both authors reviewed the full texts of the potentially eligible studies and discrepancies were settled by discussion between the 2 authors and the senior authors. Details of the search are highlighted in Figure 1. Our initial search provided 2156 articles and, after applying inclusion and exclusion criteria we identified a total of 49 studies.8-10,33,35-79 Flow chart representing the search strategy for the articles included in the review according to PRISMA guidelines.
INTRA-OPERATIVE Fractures
Classification
Vancouver classification of intra-operative PFFs.

* actually, not included into the Vancouver classification
Graphical illustration of the Vancouver classification of intra-operative PFFs.
Management of Intra-operative PFFs
Treatment of intra-operative PFFs according to Vancouver type and subtypes.

Vancouver subtype A1 PFFs (proximal metaphyseal cortical perforation)
These fractures are frequent especially during revision surgery, and are due to reduced bone stock from previous surgeries or osteolysis.9,35,60 They rarely compromise implant stability and therefore can be treated with locally harvested autograft or can be ignored and observed. No weight-bearing restriction are required.9,10,39,60
Vancouver subtype A2 PFFs (undisplaced linear crack)
They occur during femoral broaching or stem insertion, and they usually involve the medial femoral neck and the calcar. 83 Cerclage fixation is performed prior to definitive preparation and stem insertion. When an undisplaced linear crack happens at stem insertion, stability of the implant should be assessed intra-operatively: if the stem is stable, cerclage fixation (even a single cable can be enough) may prevent further fracture propagation.10,39,60 If the stem is unstable, the fracture is, and must be treated as, a subtype A3 PFF. 9
Vancouver subtype A3 PFFs (displaced or unstable fractures of the proximal femur or the greater trochanter)
They are the most frequent intra-operative fractures that need to be addressed, and they can happen both during primary uncemented THA and in revision settings. If these fractures involve the calcar, they usually compromise the tightness of the metaphyseal area, and stem instability or subsidence can happen. Multiple cerclages plus longneck head in case of minor subsidence and adequate stem stability can be enough to offer immediate post-operative weight-bearing. Otherwise, stem fixation must be obtained more distal than the fracture using a longer stem.9,10,39,60,63 If a short metaphyseal stem has been prepared for, conversion to a conventional length implant can be sufficient together with cerclages in case of a short fracture line.
Isolated greater trochanteric fragments can be treated by a variety of fixation devices: the use of wires, cables and claw plates have all been advocated (Figure 3(A)).
60
When an extended trochanteric osteotomy (ETO)61,62 is performed to remove a previous implant, a fracture may occur in either the ETO fragment or in the remaining medial part of the femur (Figure 3(B)). As ETO is not usually longer that 13-15 cm, the proximal femur can be wrapped with cerclages around an uncemented diaphyseal-fitting stem. Also, if an ETO fragment is at risk of splitting at the greater trochanter base, a structural graft may be employed to prevent fracture. Intra-operative Vancouver subtype A3 PFF. Vancouver subtype A3 intra-operative PFFs can frequently occur during revision surgery and can be stabilized around an uncemented stem with cerclages. 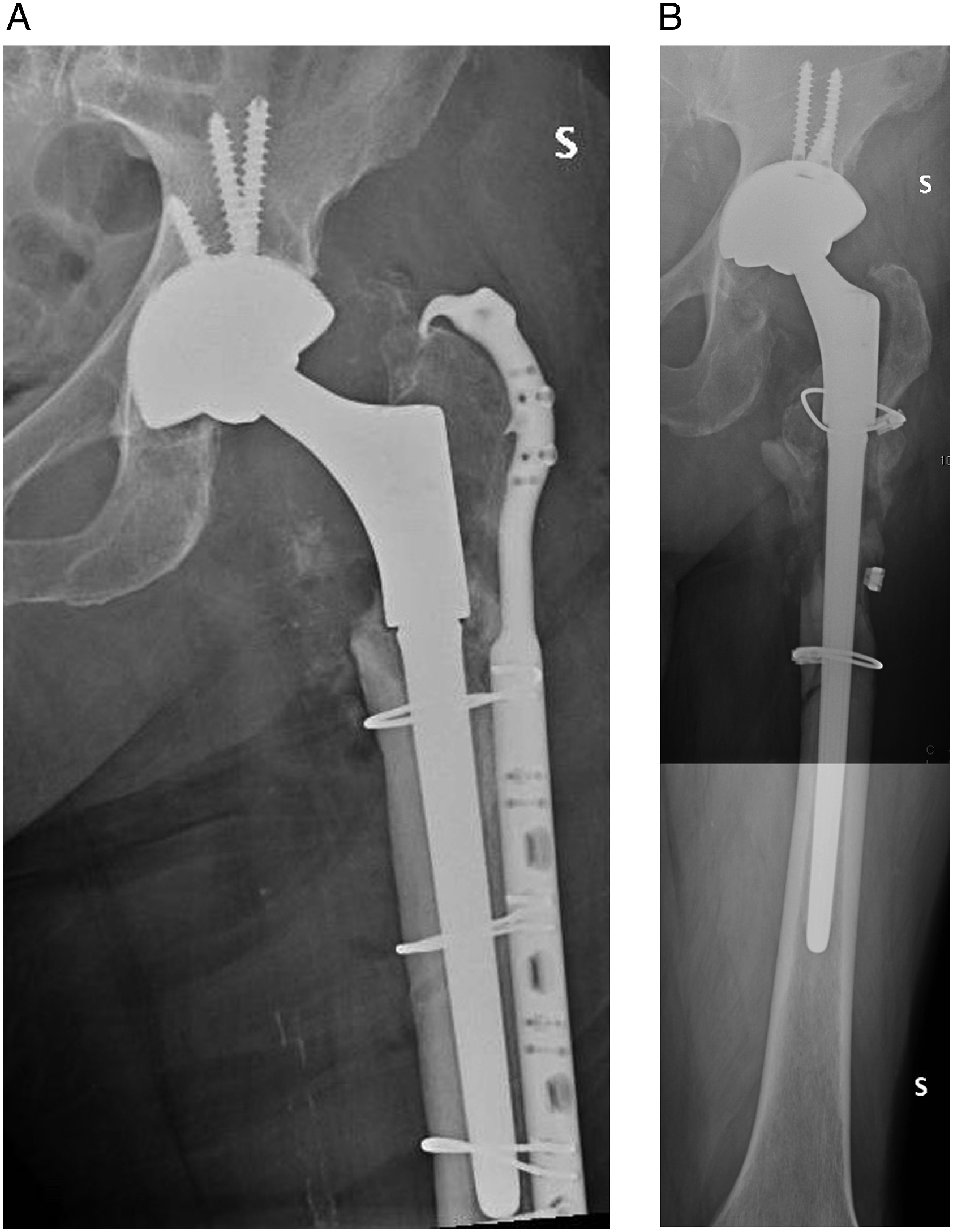
Vancouver subtype B1 PFFs (diaphyseal cortical perforation)
Cortical perforations may be intentional (fenestration for stem removal or coring for screw removal) (Figure 4(A)) or accidental during canal preparation.84,85 They should be bypassed with a long stem by at least 2 femoral diameters,
64
and ideally sealed with autograft. This is more valid in case of lateral/anterior cortex involvement of the subtrochanteric region, as stresses are higher at these levels. If the longest available stem has already been used but protection seems inadequate, a structural graft or a plate should be added. If intra-operatively the pitfall is overlooked, and the perforation at risk of fracture is seen on post-operative radiographs, weight-bearing should be restricted, or revision surgery performed, to avoid predictable consequences (Figure 4(B)).9,39,60 Intra-operative Vancouver subtype B1 PFF. A perforation due to screw removal was not adequately considered intra-operatively nor on post-operative radiographs (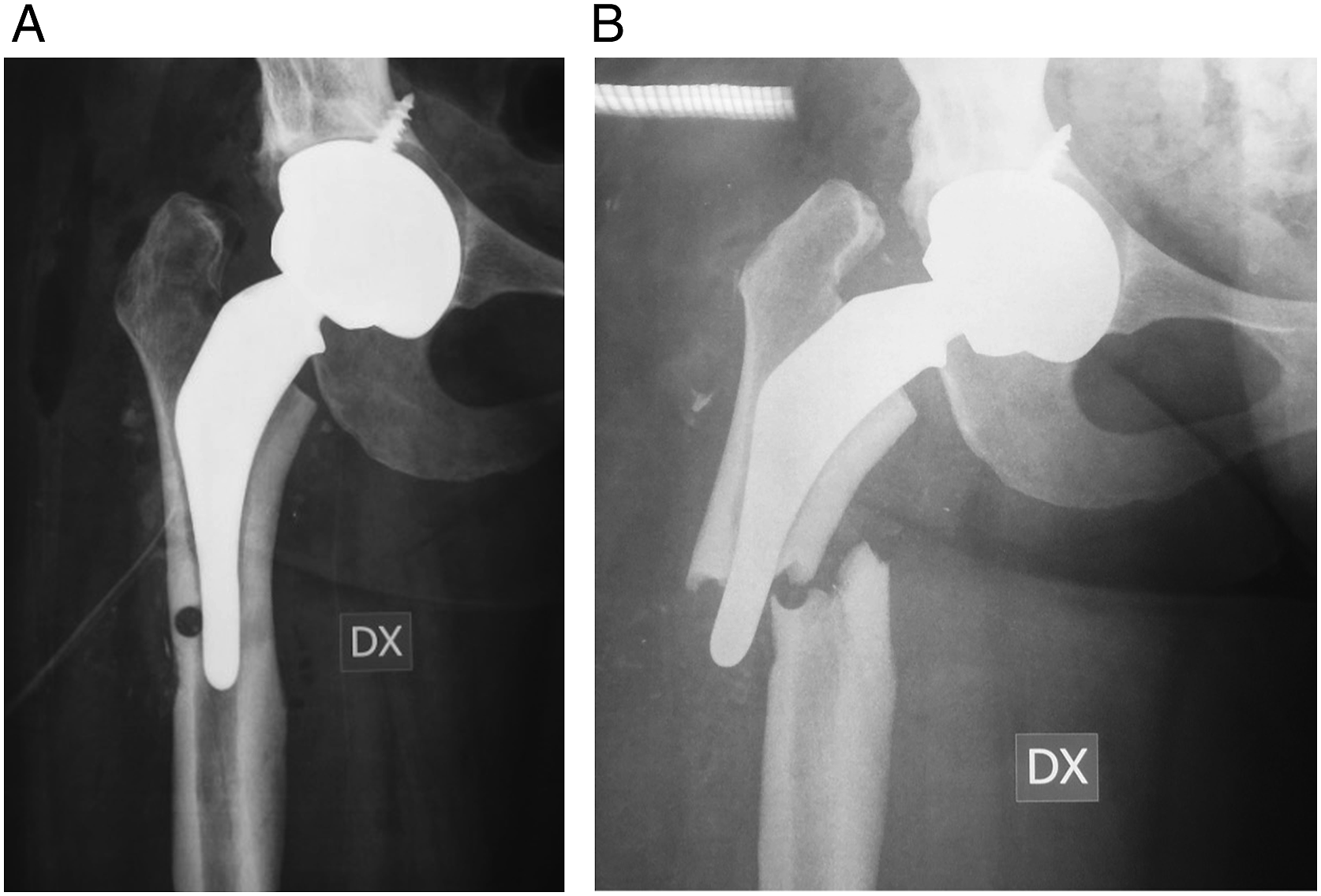
Vancouver subtype B2 PFFs (undisplaced linear crack)
These fractures are usually attributed to hoop stresses from broaching or insertion of an uncemented stem.63,81,86 If recognized intra-operatively, cerclage wire to prevent propagation of the fracture line before stem insertion should be performed. A stable fracture configuration recognised after surgery can be treated with observation and protected weight-bearing for up to 12 weeks. Unstable fracture configurations (short oblique or transverse near the tip of the stem) should be treated operatively, as B3 fractures.9,39,60
Vancouver subtype B3 PFFs (displaced fractures of the mid-shaft)
These fractures usually occur in revision settings during femoral dislocation63,87 or vigorous canal preparation, or in highly osteoporotic patients.22,88,89 The fracture must be stabilized before implanting a long stem prosthesis. Double structural grafts placed perpendicular to each other (anterior and lateral cortex) or a combination of structural graft and a plate can be useful to augment bone stock.36,50,65 Cortical onlay structural grafts increase cortical strength and have shown good clinical results, and they can also be used prophylactically.
65
Even if cerclage fixation can appear sufficient to provide fracture stability, a long stem bypassing the fracture by 2 cortical diameters is necessary to achieve axial stability (Figure 5).9,35,36,39,50,60,65 Intra-operative Vancouver subtype B3 PFF. A B3 PFF occurred during hip dislocation for THA in an osteoporotic patient. The diaphyseal component of the fracture was synthetized with multiple cerclages and an uncemented diaphyseal-fitting modular stem was implanted. After that, suture wires were used to stabilize the greater and the lesser trochanters to the proximal body of the prosthesis.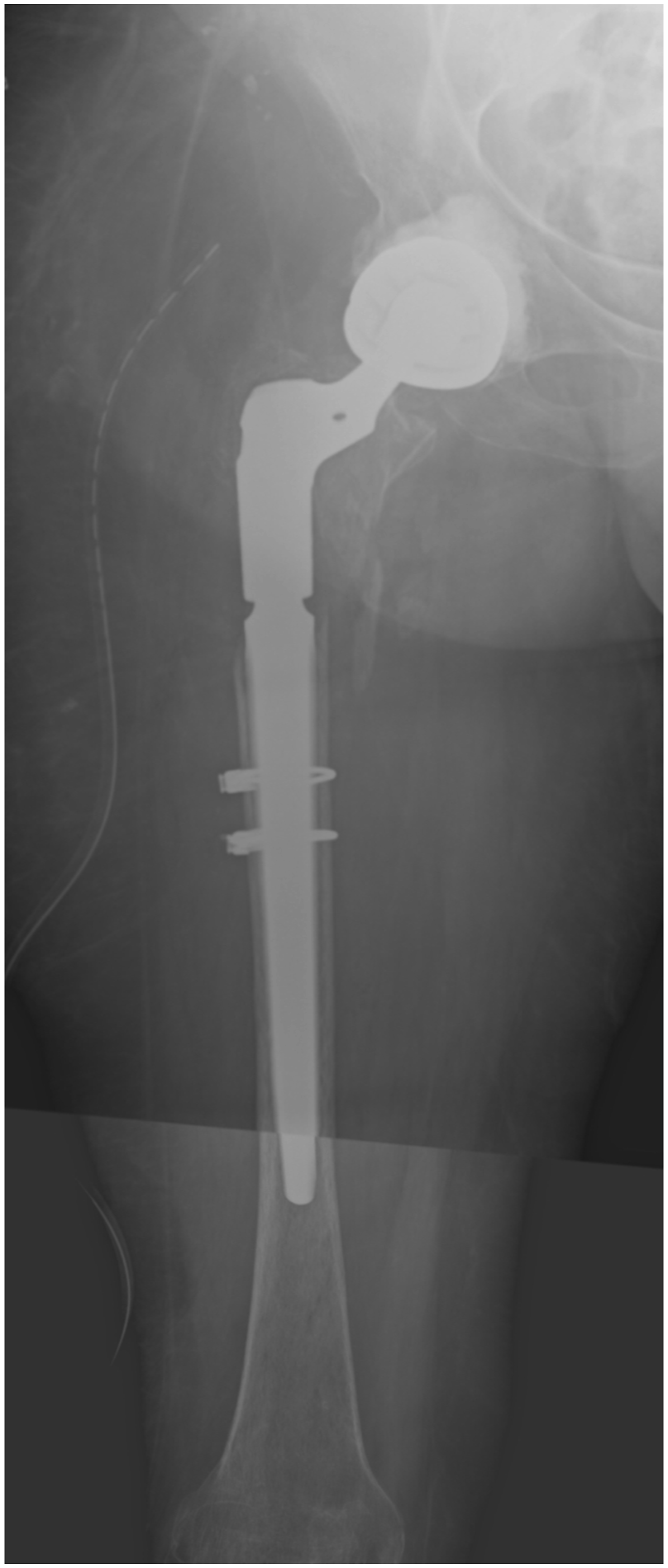
Vancouver subtype C1 PFFs (cortical perforations distal to the stem)
Structural allograft or autograft of small defects is important to avoid leaving a stress concentrator for potential post-operative fracture, and to prevent cement leakage during cementation. If the perforation is large and not well below the stem, a stress riser with higher risk of post-operative fracture exists, therefore the defect should be overlap with structural graft or a plate.9,39,60
Vancouver subtype C2 PFFs (undisplaced linear crack extending just above the knee)
Fractures with inherent stability (long spiral) can be treated by multiple cerclages. Unstable fractures or those with deficient bone stock should be treated using structural grafts and/or plates (as described in subtype B3).9,39,60
Vancouver subtype C3 PFFs (displaced fracture of the distal femur that cannot be bypassed by a long femoral stem)
These fractures are treated by fixation using locking or standard plates depending on bone quality. If such a fracture propagates to the tip of the stem, the plate should overlap the stem sufficiently to prevent a stress riser between the 2 implants. If the fracture is distal, and the stem is short, it is theoretically possible to treat this fracture with a retrograde intramedullary nail, but it would require a new approach and therefore it seems less feasible than distally extending the already open approach to the femur.9,39,60
Vancouver type D PFFs (dividing a hip and a knee arthroplasty)
Type D fractures were not contemplated in the modified Vancouver classification for intra-operative PFFs. They should be treated in accordance with their appearance as type B or C PFFs, with special consideration not to create a stress riser between implants. Therefore, plate fixation (eventually augmented with structural graft) should overlap the stems of the THA and of the total knee arthroplasty (TKA) if stemmed, to distribute gradually the stresses along the entire femur.
POST-OPERATIVE Fractures
Classification
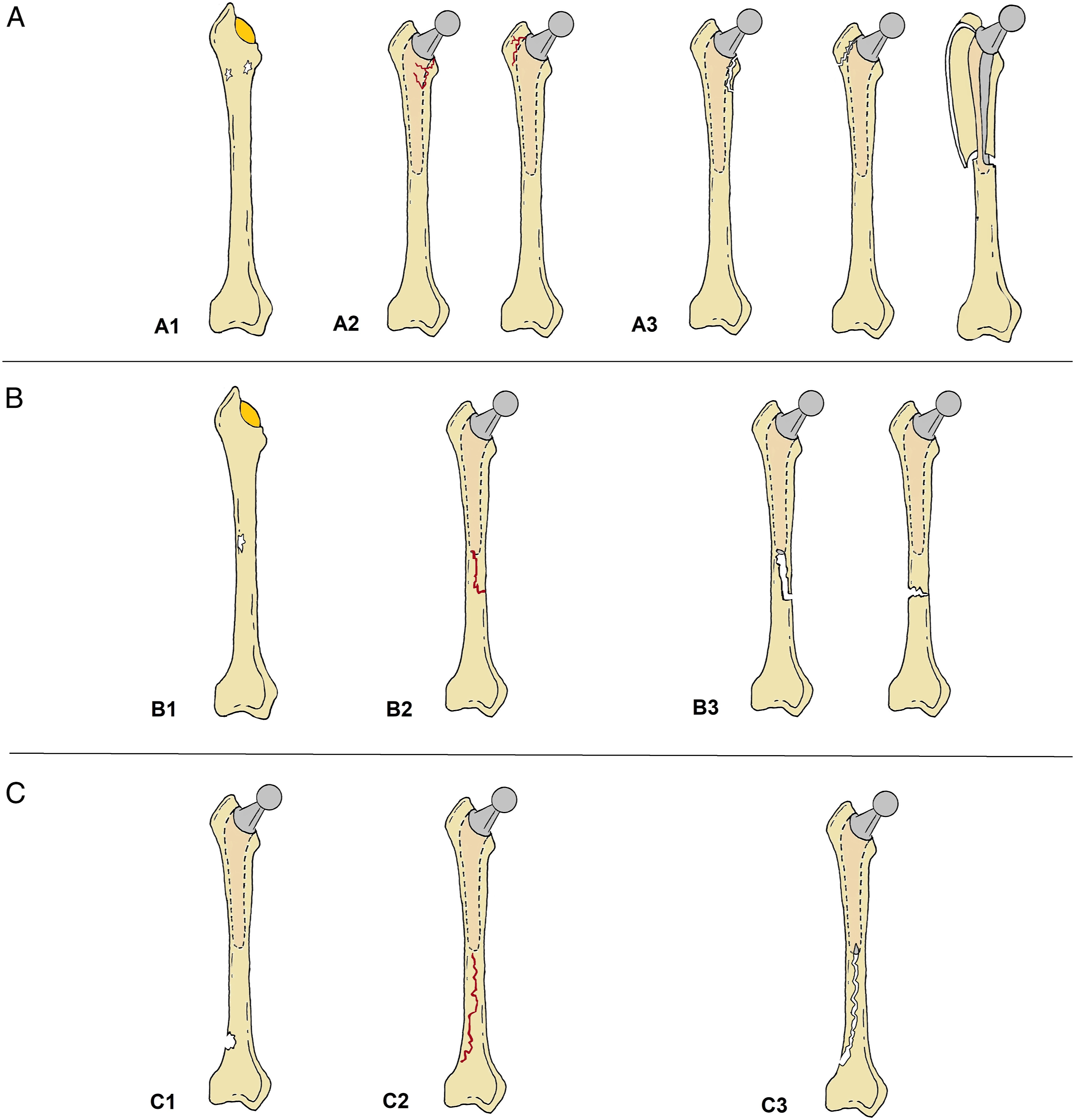
Modified Vancouver classification of post-operative PFFs. Clamshell type was first described as a pseudo-AL or new-B2, with a loose stem, by Van Houwelingen and Duncan in 2011. Later, Capello et al described it as clamshell type, being the stem stable (A1) or loose (A2). Afterwards, they have been presented as a subtype B2, but they should be properly divided into B1 and B2 PFFs (a proposal: B1CS, B2CS). The same applies to reverse clamshell patterns: stem stability also depends on where the fracture “exits” on both medial and lateral cortices.
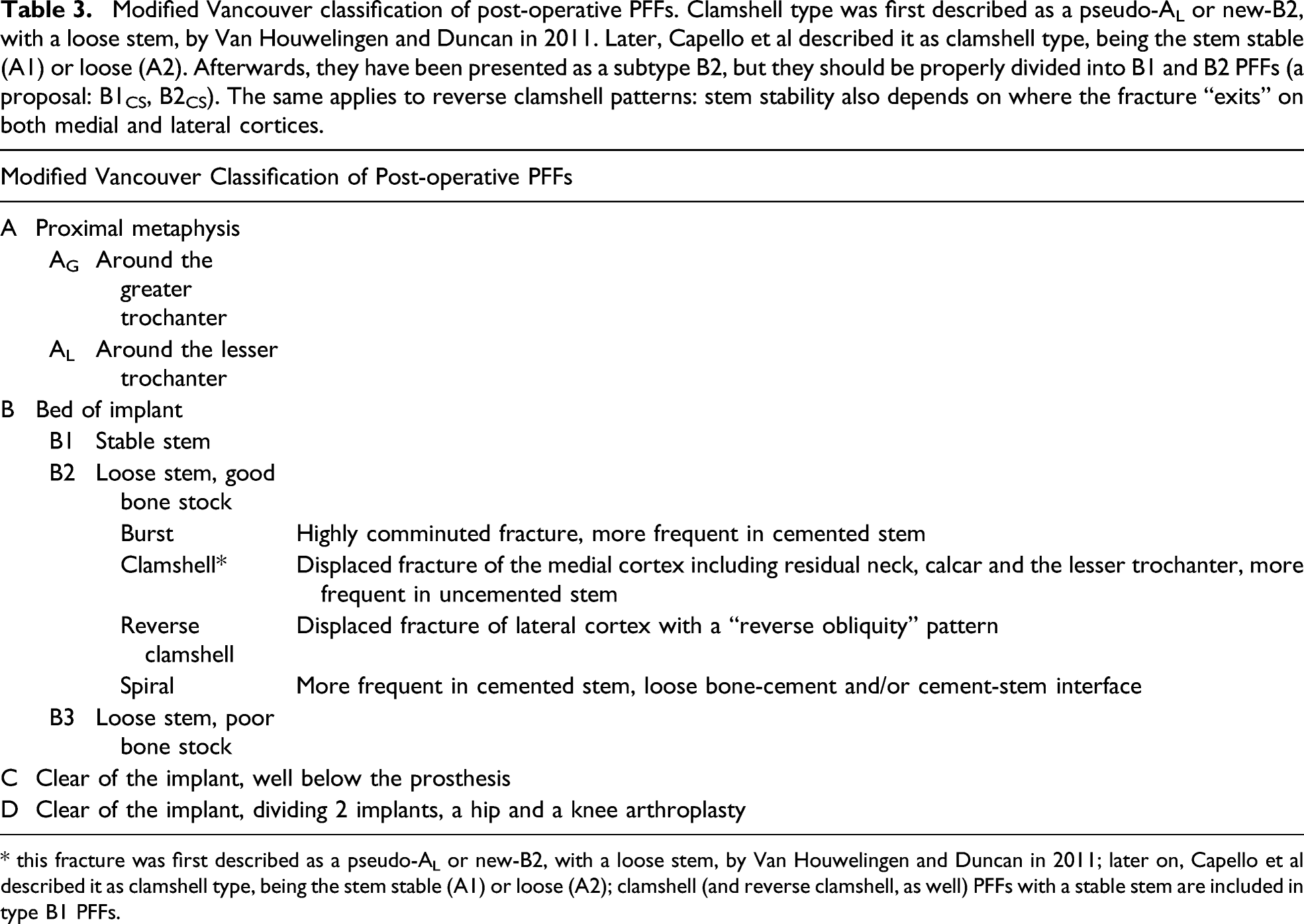
* this fracture was first described as a pseudo-AL or new-B2, with a loose stem, by Van Houwelingen and Duncan in 2011; later on, Capello et al described it as clamshell type, being the stem stable (A1) or loose (A2); clamshell (and reverse clamshell, as well) PFFs with a stable stem are included in type B1 PFFs.

Graphical illustration of the modified Vancouver classification of post-operative PFFs.
Type A fractures are located in the trochanteric region (“apophyseal”) and are subdivided in fractures involving the greater (AG) or the lesser (AL) trochanter.
Type B fractures are those around or just distal to the stem (“bed” of the implant), and they are the most common type (up to 80% of all post-operative PFFs). These fractures require surgical management except under exceptional circumstances. Type B PFFs are subdivided in 3 groups: in type B1 fractures, the stem is considered stable and the bone stock adequate; in type B2 fractures, the stem is loose, but satisfactory bone stock is present; in type B3 fractures there is severe bone loss with a loose stem. Furthermore, subtypes of B2 PFFs have been described (burst, 96 clamshell, 14 reverse clamshell, 95 spiral). 97 Also, evidence exists that different B2 subtypes present with different prevalence over uncemented or cemented stem and apparently over stem geometry.13-18 Burst fractures, with a highly comminuted pattern, are more frequent in cemented stems. 96 Clamshell fractures involve the medial cortex including residual neck, calcar and lesser trochanter, the stem can be stable or loose, and they are more frequent in anatomical and wedge design uncemented implants.13,14 The reverse clamshell pattern presents a displaced fracture of lateral cortex with a “reverse obliquity” pattern, and the stem is frequently loose. 95 Spiral pattern seems to be more frequent in cemented implants. 97
Type C fractures are those well below the tip of the stem (“clear” of the implant), while type D PFFs (introduced with the UCS-PF)11,12 are those between the tip of the femoral stem of the THA and the femoral component of a TKA (“dividing” the implants). In type D fractures, there are some key points to consider about the knee implant: the location of the fracture with respect to the knee femoral component, the possible loosening of the TKA, and the type of implant (primary or revision). This concept was first introduced by Su et al 98 and later developed by Fakler et al. 99
Management of Post-operative PFFs
Treatment of post-operative PFFs according to modified Vancouver type and subtypes (see also caption of Table 3).

*a treatment algorithm for B1 and C PFFs with potential mechanical and/or biological impairment has been proposed. 46
While obtaining the history, care should be taken to note any previous groin or thigh pain to assess for potential issues with the THA prior to the injury, as infection or loosening. If pre-injury radiographs are available, they should be examined and scrutinized as well. First of all, infection must be ruled out, especially whenever loosening is identified. 102 Pre-operative aspiration for cultural growth may require up to 2 weeks for a definitive results, and therefore is not feasible in case of PFFs. Therefore, at surgery aspiration of joint fluid for intra-operative Gram stain and intra-operative alpha-defensin testing, and peri-prosthetic soft tissues sampling for intra-operative frozen section are recommended. 102 The one-stage revision should be abandoned in favour of a two-stage procedure if suspicion is high and confirmed by intra-operative testing.
Stem stability and adequate bone quality can be difficult to be evaluated from radiographs, therefore pre-operative distinction between type B1 and B2 PFFs is not always possible. Computed tomography (CT) scan can be useful to evaluate bone-stem interface. 103 Despite careful scrutiny of preoperative images, roughly 20% of stems that were concluded to be stable were found to be loose intraoperatively.47,67
Pre-operative planning is essential. Even if osteosynthesis is scheduled, it is recommended to have a revision implant available in case of possible mobilization found intra-operatively. Also, structural allograft should be available. In fact, they can be used both in fixation and revision settings as they provide fixation with the potential to restore bone stock and increase cortical strength.104-106 Their aim is to augment both mechanically and biologically the construct. 107 In fixation procedures, they are used in conjunction with a plate, both on the medial and/or the anterior aspect of the femur, being the biplanar configuration more stable than the uniplanar 1. In revision settings, they have been used to reinforce the fracture, the calcar on the posteromedial aspect of the proximal femur,10,51 or to bypass stress risers (eg the tip of the revision stem touching the anterior cortex). 108 Intra-operative radiographs help to improve the accuracy of fracture reduction, the position of the implant and allow for dynamic screening to check stability of the construct. Post-operative rehabilitation is individualised, and protected weight-bearing may be required up to 12 weeks until radiological healing has occurred.
Vancouver subtype AG PFFs (fracture of the greater trochanter)
These fractures are usually stable. Proximal migration of the fragment of less than 2 cm should be treated conservatively (Figure 7(A)) with protected weight-bearing and avoiding active hip abduction for 6 to 12 weeks. Surgical indications are proximal migration of more than 2.5 cm, instability and weakness in abduction, or nonunion with pain.37,38,71 Fixation of the greater trochanter is achieved through the use of cerclage wire or the use of a trochanteric claw plate
69
; autologous graft is recommended in case of nonunion or residual defect (Figure 7(B)).38,39 Post-operative Vancouver subtype AG PFF. A fracture of the greater trochanter (Vancouver AG) can be treated conservatively if undisplaced (
If the fracture is associated with proximal femoral osteolysis, and the stem is stable, this is usually attributed to polyethylene wear that can be treated with acetabular revision, impaction grafting and greater trochanter fixation. If the osteolysis extends more distally, the stem can be loose and revision may be advised.9,10,35,36,55
Vancouver subtype AL PFFs (fracture of the lesser trochanter)
These fractures are treated conservatively. A large postero-medial calcar fragment (though unusual) may compromise proximal stem stability, making stem revision necessary with distal diaphyseal fixation.9,10,35,36,38,39,55,69 Anyway, a large fragment involves the “bed” of the stem and therefore should be better classified as a type B PFF (with stable or unstable stem).13,14
Vancouver subtype B1 PFFs (fractures at the level of a stable stem)
Undisplaced B1 fractures can be treated conservatively if the fracture presents inherent stability, but operative treatment is nowadays preferred if the patient is surgically fitted (Figure 8).66,69 Displaced fractures are operatively treated (Figure 9(A) and Figure 9(B)). In both undisplaced and displaced cases, minimally invasive plate osteosynthesis (MIPO) or open reduction and internal fixation (ORIF) can be advised, depending on fracture’s pattern, the need for anatomical reduction, the need for cerclaging around the stem and for structural graft augmentation, and surgeon’s preference and habits.9,10,35,36,38-43,47,70 Post-operative undisplaced Vancouver subtype B1 PFF. A clamshell type fracture with a stable stem (Vancouver B1, or A1 as proposed by Capello et al) can be treated with stem retention and internal fixation. Post-operative displaced Vancouver subtype B1 PFF. A reverse clamshell type fracture (

If the fracture is transverse or short oblique, or presents medial comminution, or is over a cemented stem, 44 mechanical and biological healing potential are reduced. In these occurrences, revision to a long stem that could be possibly augmented with a structural allograft has also been proposed,45,47,72 or a combined surgical and medical approach,33,46 to reduce the risk of failure of the fixation construct.
Vancouver subtype B2 PFFs (fracture around an unstable stem, with adequate bone quality)
These fractures should be treated by revision with long stem bypassing the most distal fracture line by at least 2 femoral diameters (Figure 10(A) and Figure 10(B)).9,35,64 The fractured proximal femur should be always stabilized to the prosthesis and/or to distal femur. Additional rotational stability may be necessary in some cases, using an extramedullary augmentation (plates or structural allografts, or a combination of them).38,48,49,52,53 Impaction grafting technique and cemented stem have also been used.10,50,51,69 Post-operative Vancouver subtype B2 PFF. 
Vancouver subtype B3 PFFs (fracture with unstable stem and inadequate bone quality)
These fractures are difficult to treat due to deficient bone stock (Figure 11(A)). Anyway, these fractures should be treated with long stem revision or an allograft-prosthetic composite (APC)38,77 or proximal femoral replacement.57,78 A distally locked stem is advised in low demand patient as a salvage procedure.38,79 The remnant of the host proximal femur can be wrapped around the new construct (Figure 11(B)).36,77,78 Double mobility implants are often used with these constructs to improve joint stability.
9
Impaction grafting technique and cemented stem have also been used.10,50,51,69 Post-operative Vancouver subtype B3 PFF. A type B3 PFF (
Vancouver type C PFFs (fracture clear of the stem)
When the fracture occurs below the tip of the stem (Figure 12(A)), the implant is usually considered stable, but the bone-implant interface should still be carefully examined for any signs of loosening. These fractures can be treated using standard osteosynthesis techniques,10,55 singular lateral plate fixation has been the mainstay of treatment for Vancouver C-type PFFs (Figure 12(B)).
69
When possible, indirect reduction techniques and MIPO should be applied to preserve blood flow to the fracture site by placing the plate in a submuscular, epiperiosteal plane.39,47 It is important to avoid a stress riser between the plate and the femoral stem9,38: fractures close to the tip of the stem require therefore a longer plate that span the stem proximally. Ideally, the entire length of the femoral stem should be plated up to the subtrochanteric region. Over the stem, a combination of cables and locking screws seems to guarantee stability of the construct.
36
Post-operative Vancouver subtype C PFF. A type C PFF (
Vancouver type D PFFs (fracture between 2 implants)
With regards to Su et al classification, considering a stable femoral component (Su type 1-2), the PFF is treated as a Vancouver type C as previously described.36,75,76 In the case of a fracture on a primary TKA with an open box femoral component, a possible surgical option is represented by locked retrograde intramedullary nail.36,54,75 A PFF over a stable TKA with a closed box or a stemmed femoral component will require, on the other hand, osteosynthesis with a plate.36,74-76 When loosening of the TKA femoral component is observed, due to fracture (Su type 3) or aseptic mobilization, the only possible treatment consists of total revision of the TKA.36,75,76 Attention must be paid, in all cases, not to leave a segment of weakness between the tips of the hip and knee stem. In order to avoid increased mechanical stresses and a new subsequent interprosthetic fracture, it is recommended to reinforce the construct with additional preventive plating and/or the use of structural graft overlapping the 2 implants.58,73 A total femur prosthesis can also be taken into account when both the hip and the knee femoral implants would not have adequate stability.38,56,57,59 Flowchart of Table 1.
Conclusions
Because of the increase in the THAs annually performed, PFFs are going to become more frequent, and their treatment poses a significant challenge to the orthopedic community. The extreme variability of stem designs, the possibility of having cemented or uncemented stems, the difficulty in identifying the “real” level of the fracture and the actual stability of the stem can prevent the definition of a standardized treatment. Both when revision surgery and osteosynthesis are indicated, it must be considered the procedure not as a revision of a stem nor as the fixation of a fracture. PFFs present peculiar characteristic that must be considered and special features that must be addressed. Single plating (even with the biologically preserving MIPO technique) presents limitation especially in B1 PFFs with an unstable fracture configuration or biological impairment. Locking plates are useful in osteoporotic bone and polyaxial locking plates are useful around a stem. Modular uncemented revision stems (fluted-tapered or fully coated) are easy to use but at least 5 cm of intact diaphysis are required to guarantee stable distal fixation, and synthesis of the proximal fragment is of paramount importance for function (muscle attachment) and bone stock conservation. Structural grafts can add both mechanical and biological support, either in revision or in fixation procedures, and help to restore bone stock for future surgery. Stress concentrators should be avoided, and a plate or a structural graft overlapping the points at risk should be used. If massive bone loss is present, the use of APC or tumor prostheses are justified by evidence in Literature. Cement-in-cement revision can be proposed in selected cases with good and stable cement mantle. Also, impaction grafting with long cemented revision stem for B2 and B3 PFFs has been successfully used.
In conclusion, high expertise is fundamental for the surgical management of PPFs, so this kind of fractures should be treated only in specialized centres with both high volume of revision joint arthroplasty and trauma surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.