
Abstract
Introduction
Surgical site infection (SSI) following fragility hip fracture (FHF) surgery is associated with increased morbidity and mortality.
Significance
Prediction of patients at risk for SSI is fundamental. We aimed to determine whether subcutaneous radiographic fat measurement (SRM) is associated with increased SSI risk.
Methods
A retrospective case-control comparison of SRMs at 3 locations around the hip. Patients diagnosed with SSI in the first post-operative year were matched with age, gender, surgical year, Charlsons’ co-morbidity index score, and surgical type controls, not diagnosed with SSI, at a 1:2 ratio. Measurements included the distance between (1) the sourcil to skin surface (SS), (2) the tip of the greater trochanter to skin surface (TGTS), and (3) the most prominent lateral aspect of the greater trochanter to skin surface.
Results
1430 patients were operated during the study period, of whom 45 patients presented with a diagnosis of SSI and compared to 90 controls. Infections occurred 27.4 ( ± 24.8) days following surgery. SRM significantly differed between groups, and all were higher in the study group; SS, 86.8 ± 25.5 cm vs 74.2 ± 15.3 cm; TGTS, 59.8 ± 26.3 cm vs 47.0 ± 15.8 cm; and LGTS, 45.4 ± 25.1 cm vs 33.2 ± 15.1 cm (P = .003, .004, and .004, respectively). Intraclass correlation coefficients (intra-rater) were high for all measurements (.999 for all). Intraclass correlation coefficients (inter-rater) for SS, TGTS and LGTS were high, .749 (.663.815), .792 (.719.847) and .817 (.751.866), respectively.
Conclusions
SRMs were found to be a valid and reproducible tool for predicting high risk of SSI in geriatric patients sustaining FHFs.
Level of Evidence
III.
Keywords
Introduction
Surgical site infection (SSI) is a devastating complication following fragility hip fracture (FHF) surgery, associated with deteriorated walking ability, loss of independence, increased medical costs, and increased mortality.1,2 Particularly, when SSI occurs, the reported rates of 90-day mortality triple, and one-year mortality doubles reaching over 50%.2-4
Several factors were identified as related with SSI, amongst which are age, assisted living, diabetes mellitus, immunosuppression, liver and kidney diseases, warfarin treatment, tobacco and alcohol consumption, peripheral vascular disease, and obesity.5-9 As body mass index (BMI) does not take into consideration body composition, it is not a specific predictor for SSI, and body fat percentage was found to be a more sensitive and precise measurement of SSI risk.10,11 Subcutaneous radiographic fat measurement (SRM) is an emerging tool for SSI risk prediction in the field of general surgery12,13 and orthopedic surgery.14-17
Due to the devastating consequences of SSI in the fragile FHF population, early identification of risk factors is of critical importance. In this study, we explore whether SRM is associated with increased risk for SSI following fragility hip fracture surgery. We hypothesized that increased subcutaneous fat thickness identified in different SRMs in perioperative radiographs is an independent risk factor for developing SSIs following surgery.
Materials and Methods
Study Design
Following approval of the institutional review board, a retrospective cohort study of patients 65 years and older, who underwent surgery following fragility hip fractures (31A1, 31A2, 31A3, 31B1, 31B2, and 31B3) 18 between January 2011 and June 2018, in a single orthopedic department was conducted. Surgical therapy was defined as closed reduction, open reduction, or hemiarthroplasty (either cemented or cementless, antibiotics was not embedded in the cement). Exclusion criteria were pathological and impending fractures, fracture sustained during hospitalization due to other medical cause (to reduce confounding causes for SSI), fractures sustained over five days before presentation, and patients with technically inadequate radiographs (skin edge not visible due to either cassette positioning or extremely large pelvic girth). For patients who presented with a contralateral fracture during the study period, only the first fracture was included.
All patients who presented with SSI in the first post-operative year were collected and compared to matching controls who did not present with an SSI in a 1:2 ratio. Matching was based upon gender, age, year of surgery, Charlsons' co-morbidity index score,19-21 and surgical type (fracture fixation or hemiarthroplasty).
Variables and Measurements
Primary outcome was defined as the association between SRM and the incidence of SSI in the first post-operative year. Secondary outcome was one-year post-operative mortality.
Procedure
Upon arrival to the emergency department, all patients were clinically evaluated by an orthopedic surgeon and x-ray imaging was acquired. Patients were hospitalized either to the orthopedic or the geriatric wards depending on vacancy. Patients admitted to geriatrics were prepared for surgery there, spent the first post-operative day in the orthopedic department, and returned to the geriatric department for the rest of their hospital stay, where a daily orthopedic surgeon assessment was performed. In case the patients had a concurrent active medical problem, they were admitted to an internal medicine department. Surgery was performed within 48 hours of admission unless the patient was determined as clinically unfit for surgery by the anesthesiology team. Following surgery, all patients received daily sessions of respiratory and ambulatory physical therapy. Thromboprophylaxis with low molecular weight heparin (enoxaparin, 40 mg once daily) was routinely initiated on the first post-operative day. For patients under chronic anticoagulant treatment, regular treatment regimen was returned starting POD3 in accordance with physical examination and hemoglobin levels.
Data Collection
Demographic data, including 1-year mortality, walking ability, and living arrangements, was collected. The Charlson’s comorbidity index (CCI)19,20 was used to evaluate patients' co-morbidities. Hospitalization characteristics such as admitting department, time to surgery (defined as time from admission to operating room), implant used for fracture fixation, length of hospital stay (LOS), the need for blood transfusions, in-hospital infections other than SSI, and pre-surgical laboratory values (white blood count, hemoglobin, platelets, creatinine, and international normalized ratio [INR]) were gathered.
The diagnosis and type of SSI was based on accepted Centers for Disease Control (CDC) criteria and established from the hospital records and microbiology results. 22 Intra-operative tissue samples were cultured on blood and MacConkey agar plates, with an extra blood agar plate for anaerobic bacteria. A fraction of the specimen was also incubated in thioglycolate broth for enhanced sensitivity. Upon colonies’ growth, bacterial identification was performed using the Bruker MALDI-TOF MS system and/or the Vitek2 system. Antibiogram was performed using disk diffusion assay as well as Etest for minimum inhibitory concentration (MIC), with interpretations based on Clinical and Laboratory Standards Institute (CLSI).
For patients presenting with surgical site infection in the post-operative year, information regarding data related to the infection itself, including results of peripheral blood and of deep tissue cultures obtained during surgery, treatment course, and outcome were collected.
Data was gathered via a shared electronic medical record program, which allows access to data from healthcare facilities countrywide.
Subcutaneous Radiographic Measurements
Radiographic measurements were performed on the pre- or post-operative standardized anteroposterior (AP) pelvis x-rays in the supine position and 1525° of internal rotation of the hips.
Subcutaneous fat was measured in three anatomical landmark-based locations as described by others.
17
Measurements included the distance between (1) the sourcil to skin surface (SS), (2) the tip of the greater trochanter to skin surface (TGTS), and (3) the most prominent lateral aspect of the greater trochanter to skin surface (Figure 1). Subcutaneous radiographic measurements.
Radiographs were calibrated using the inserted implant or previously inserted implant of known caliber. For example, in patients with intramedullary nails, the known diameter of the nail was used as a reference for the subcutaneous measurements. In patients with a hemiarthroplasty, the known diameter of the head component was used as reference. Finally, in patients with a dynamic hip screw (DHS), the known cephalic screw length was used as a reference (Figure 2 A-C. Subcutaneous radiographic measurement calibration. (A) Proximal femoral nail antirotation. Measurements were calibrated based on the known length of the inserted nail. (B) Bipolar hemiarthroplasty. Measurements were calibrated based on the known diameter of the inserted head component. (C) Dynamic hip screw. Measurements were calibrated based on the known length of the inserted screw.
All measurements were taken twice on different occasions for intra-observer correlation. Inter-observer correlation was also obtained.
Statistical Analysis
Continuous variables are presented as mean and standard deviation (SD). Quantitative and ordinal variables are presented as absolute and relative frequencies. The Fisher’s exact tests was used for categorical variables, the Wilcoxon test for ordinal variables, and the Student’s t-test for numeric variables. KaplanMeier survival curves were used to demonstrate 1-year survival. Intra-observer correlation between the two measurements was determined using Pearson’s correlation coefficient All reported P-values will be two-tailed. Statistical significance was defined as P < .05. Statistical analysis was performed using R Core Team (2020) (R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria).
Results
1430 patients aged 65 years and older have presented with proximal hip fracture during the study period. Of whom, 46 have returned with a post-operative SSI in the first post-operative year. They were matched with 92 controls who did not present with an SSI. One patient from the study group and 2 patients from the control group did not meet inclusion criteria and were excluded, leaving 45 patients (27 hemiarthroplasties, 15 cemented, and 18 ORIF) and 90 controls (55 hemiarthroplasties, 21 cemented, and 35 ORIF) for analysis.
Patients' baseline characteristics.

aData were unavailable for 2 patients from the study group and for 3 patients from the control group.
bData were unavailable for one patient from the control group.
cData were unavailable for 7 patients from the study group and for one patient from the control group.
Hospitalization characteristics.
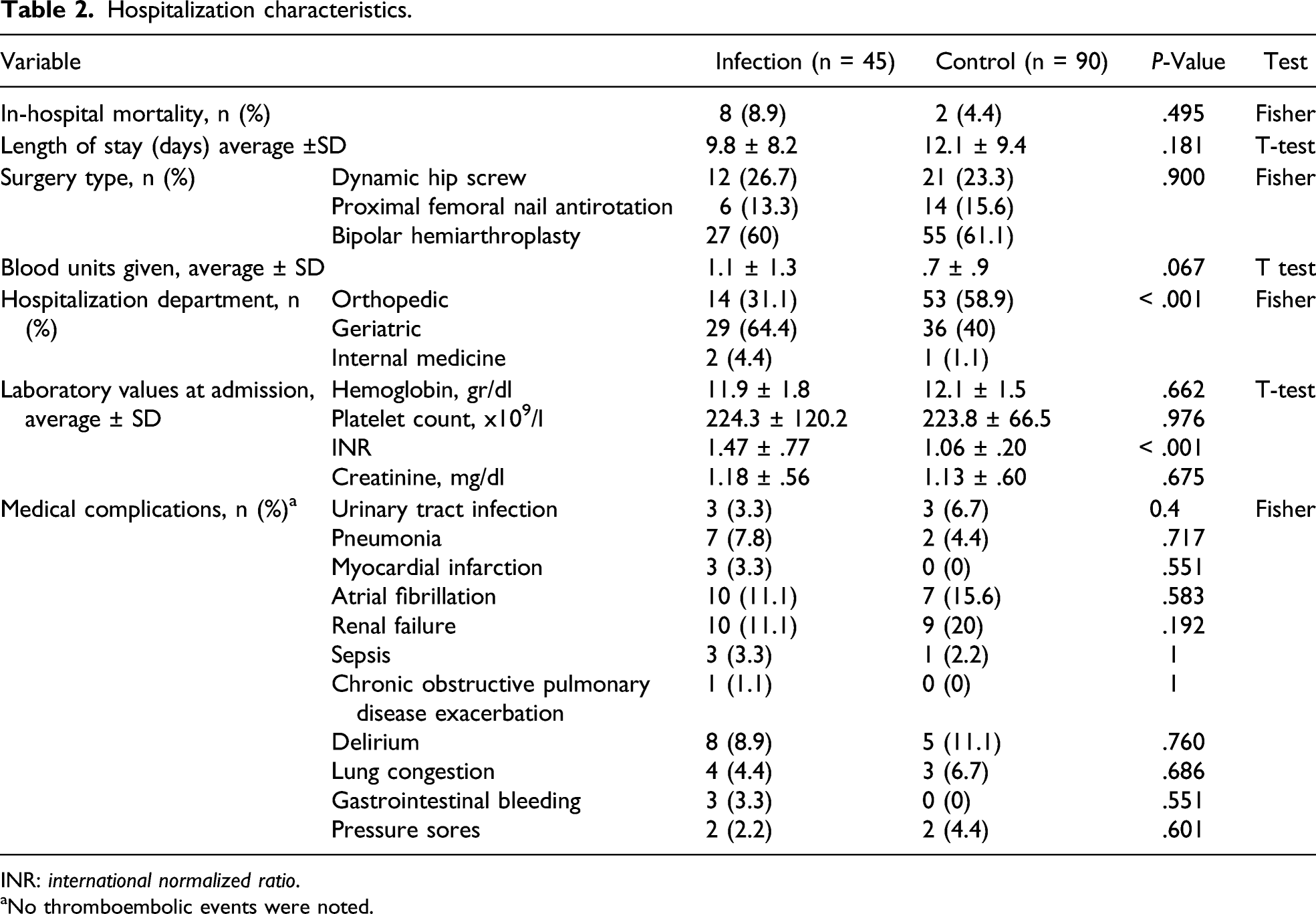
INR: international normalized ratio.
aNo thromboembolic events were noted.
Subcutaneous fat measurements.

INR: international normalized ratio.
aFat measurements also significant when controlling for anticoagulation use.
Significant co-linearity exists between fat measurement variables; sourcil to skin surface and tip of greater trochanter to skin surface, Pearson’s r = .89; sourcil to skin surface and lateral greater trochanter to skin surface, Pearson’s r = .85; and tip of greater trochanter to skin and lateral greater trochanter to skin surface, Pearson’s r = .94.
One-year mortality significantly differed between study groups and was higher for the study group (44.4% and 23.3% for the infection and control group, respectively, P = .017) (Figure 3). No significant association was found between subcutaneous fat measurements and mortality when controlling for infection. One-year survival.
Surgical site infection characteristics.

aData were unavailable for 4 patients.
bMethicillin-resistant Staphylococcus aureus (7), Escherichia coli extended-spectrum beta-lactamase (1), Klebsiella pneumonia extended-spectrum beta-lactamase (1), and Proteus spp. extended-spectrum beta-lactamase (1).
Discussion
Subcutaneous radiographic fat measurements were found to be related to surgical site infection risk following fragility hip fracture surgery, in line with our hypothesis. This was true for all three measurements, with a high intra-observer and inter-observer agreement. In-turn, SSI was associated with increased mortality in the first post-operative year.
Elevated subcutaneous radiographic fat measurements are known as risk factor for SSI in the field of general surgery. Fujii et al 12 found fat distribution in computerized tomography (CT) scans to be independently associated with SSI in colorectal surgery, and Kozlow et al 13 have demonstrated similar outcomes between fat distribution measured on CT scans and SSI risk following sternal reconstruction surgery. In orthopedic spinal surgery, Mehta et al23,24 reached comparable conclusions for both surgical cervical and lumbar spine fusions. Interestingly, in the field of joint arthroplasty, the few available studies in the literature reveal conflicting results. When addressing total knee arthroplasty, while Watts at al 14 have found elevated SRM to be associated with increased risk for SSI, Gupta el al 25 have actually described higher SRM to be a protective factor. Likewise, following total hip arthroplasty, Sprowls et al 16 have found thick subcutaneous fat to be related with SSI, while Bell at al 17 did not reach similar results.
To our knowledge, only a single previous study has suggested an association between the SRM at the hip and the risk of SSI in elderly patients with surgically treated hip fractures. Bernaus et al 9 have measured subcutaneous fat thickness at the level of the tip of the greater trochanter and found a 2.24-cm greater mean SRM to be related with increased infection risk. Our findings are concurring for measurements at three locations, yet we did not find a specific threshold value. When the fat measurements were analyzed as a dichotomous variable with a cutoff at the top quartile, none was found to be associated with increased risk for infection (P. value: .060, .060, and .102 for sourcil to skin, lateral greater trochanter to skin, and tip of greater trochanter to skin, respectively) (in accordance with Bell et al’s 17 measurements following total hip arthroplasty). Analysis using receiver operator characteristic curves did not find an alternative threshold that is clinically relevant. Although increased subcutaneous fat measurements were found to be associated with increased risk of infection, in our study, they do not have high enough sensitivity and specificity to be considered as sole predictors of infection.
Several explanations can be suggested for the relation between the increased SRM and the elevated infection risk. First, obese patients’ drug distribution is altered because of different distribution volume, changes in regional blood flow, and different plasma protein binding. 26 Even when prophylactic antibiotic dosage is doubled and plasma drug concentration is high, the tissue penetration is substantially lower in obese patients, and was shown to be below the minimum inhibitory concentration for aerobic and anaerobic microorganisms.26,27 Second, an extensive subcutaneous fat tissue is a risk for potential dead space, leading to the accumulation of a seroma or a hematoma, in which an infection can develop. 28 Third, it might be that the thick subcutaneous tissue handling during surgery is more time consuming, leading to a prolonged surgical duration, which in turn is associated with SSI following fragility hip fracture surgery.3,29,30 Finally, the elevated infection risk might be related with the metabolic activity of the subcutaneous fat tissue, which includes proinflammatory cytokine signaling. 31
Limitations of this study include the retrospective manner of data collection. While a patient’s allocation to the orthopedic and geriatric ward was random by nature, we found that infection rate was higher for patients admitted to the geriatric ward, independent of INR and SRM. This might be related to the vicinity of the operated patients to other patients hospitalized perhaps for infectious diseases. We found that while patients who were hospitalized to the geriatric ward had similar rates of DM and PVD at presentation (known risk factors for SSI), the incidence of post-operative infections (pneumonia, urinary tract infection, and sepsis put together) was higher (5.9% for patients in the orthopedic ward and 21.5% for patients in the geriatric ward, P = .009). However, due to the retrospective nature of this study, this hypothesis could not be examined, and further studies are required. Lastly, elevated INR values were also found to be related with SSI, independently from SRM. While surgery was performed when INR was 1.5 or lower, a value considered safe for surgery, 32 this could be related to a hematoma formation of to a suggested immunomodulatory effect of warfarin. 4
Conclusions
This study suggests high risk for post-operative SSI in fragility hip fracture patients with elevated SRM. For patients at risk, we recommend special care to be taken for adequate soft tissue approximation during wound closure to reduce seroma, and hematoma formation, and meticulous wound surveillance in the post-operative period, as most patients presented within the first post-operative month while still under medical surveillance in rehabilitation facilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
Tal Frenkel Rutenberg and Rotem Markman have contributed equally to this work.
Ethical Approval
The study has been performed in accordance with the ethical standards in the 1964 Declaration of Helsinki and approved by the institution review board.