
Abstract
Background
To evaluate the incidence rate of urinary tract infection (UTI) and postoperative urinary retention (POUR) in the initial indwelling urinary catheter (IIC) and intraoperative indwelling urinary catheter (IOC) groups of hip fracture patients who had undergone either fracture fixation or hemiarthroplasty operation within 48 hours.
Methods
Between June 2023 and October 2024, 110 patients who met the eligible criteria were enrolled in this study. We prospectively randomized all patients into the IOC (n = 55) and IIC (n = 55) groups. The postoperative incidence of UTI and POUR was compared between the two groups and evaluated 24 h postoperatively.
Results
The incidence of UTI was significantly higher in the IIC group (23.6%) than in the IOC group (9.1%) (P = .039). However, the incidence of POUR was not significantly different between the groups (16.4% vs 9.1%; P = .252).
Conclusion
For hip fracture patients undergoing early surgery within 48 h, intraoperative urinary catheterization significantly reduced the incidence of POUR, while the incidence of UTI did not differ significantly between the groups.
Keywords
Introduction
Hip fracture is a common problem in elderly individuals, particularly those aged >60 years.1,2 It is associated with a high morbidity and mortality rate, reaching as high as 14%–36%. 3 Performing surgery to repair a fracture or hemiarthroplasty within 48 hours of hospital admission significantly reduces complications and mortality rates.4-6 Two of the most common and clinically significant complications that occur following hip fracture surgery are postoperative urinary tract infection (UTI) and postoperative urinary retention (POUR). The incidence of UTI is approximately 11% and that of POUR ranges from 5.5% to 46.3%, depending on surgical and patient-related factors.7,8
Initial indwelling catheters and intermittent catheterization are commonly used, with catheter removal typically performed within 24 h postoperatively.6,9,10 Most patients with hip fracture experience significant pain, immobility, and difficulty to void. These conditions are associated with urinary retention, which subsequently increases the risk of developing UTI. 11 Therefore, the practice of initial indwelling urinary catheter (IIC) at hospital admission is necessary; however, prolonged urinary catheterization is a risk factor for catheter-associated UTI (CAUTI).12-18 Meanwhile, the intraoperative indwelling urinary catheter (IOC) is another acceptable option. However, during the waiting period before operation, most patients experience pain resulting from urinary retention and require monitoring of urinary output for guiding fuid resuscitation. 19 Therefore, an appropriate timing for urinary catheterization remains unclear.
This study aimed to compare the incidence of postoperative UTI and POUR between the IIC and IOC groups of hip fracture patients who had undergone either fracture fixation or hemiarthroplasty within 48 hours. Our hypothesis was that IOC would reduce the incidence of postoperative UTI and POUR.
Methods
The study was approved by the ethics committee of our institution (COA number 105/2566) and was registered with Clinical Trial Registry (TCTR20241231004). Written informed consent was obtained from all participants prior to their inclusion in the study. This prospective, randomized study was performed between June 2023 and October 2024. Patients were randomized into two groups: IIC (n = 55) and IOC (n = 55) (Figure 1). A computerized block randomization (block size of 4) was generated by an independent researcher. Group allocation was concealed using opaque sealed envelopes, which were opened only after patient enrollment. As participants or the surgical team could not be blinded, only the outcome assessors and data analysts were blinded to group allocation. Consort Flow Diagram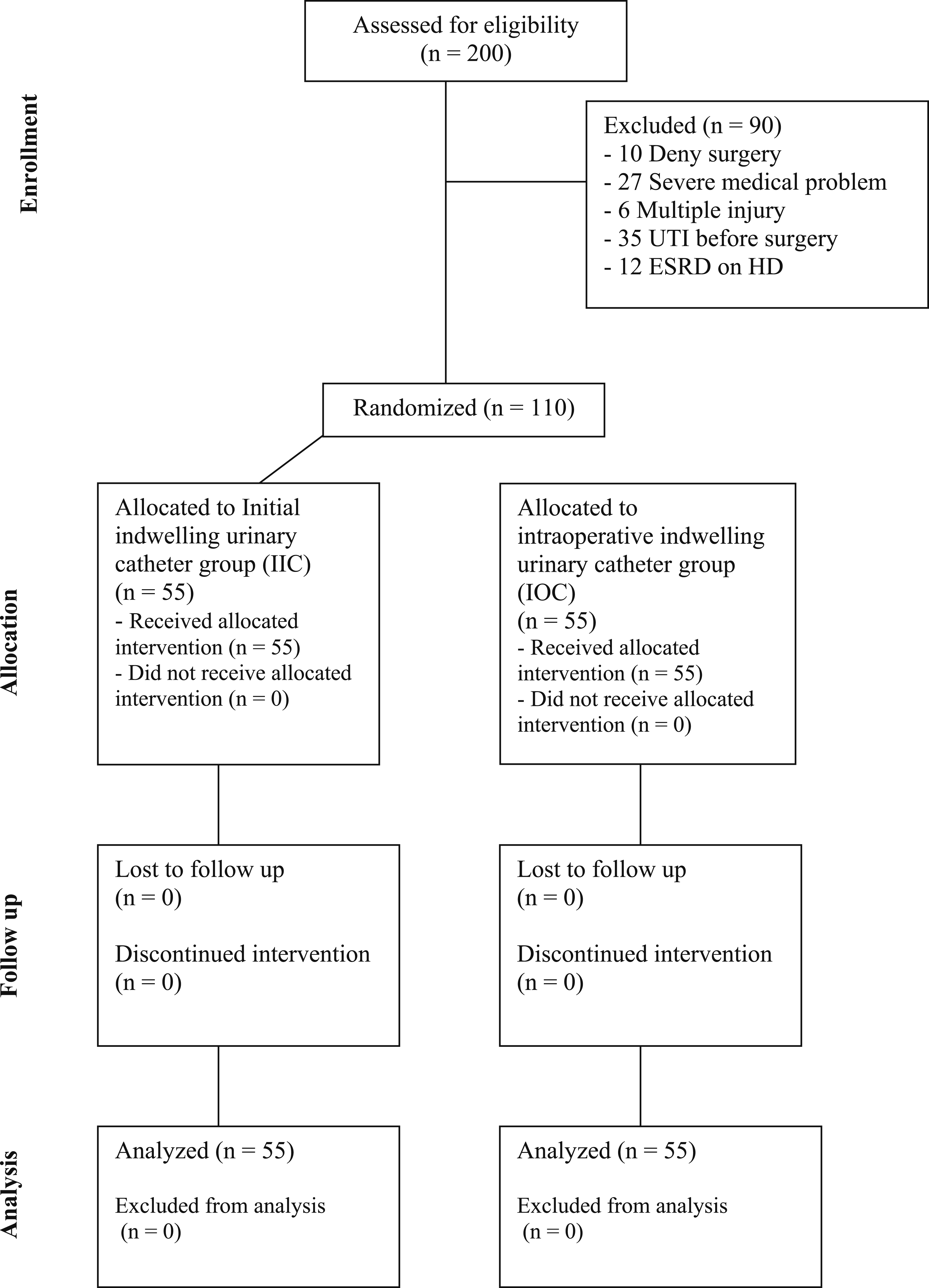
Surgical treatments including fracture fixation and hemiarthroplasty were performed with proper indication. Patients diagnosed with hip fracture, including fracture neck of femur and peritrochanteric, who had undergone fracture fixation or hemiarthroplasty within 48 hours were included in this study. Patients with a pre-existing indwelling urinary catheter, pathological fractures from metastasis, urological disorders (eg, benign prostatic hyperplasia and neurogenic bladder), diabetes mellitus with HbA1C ≥7%, end-stage renal disease, pre-existing UTI, and chronic steroid use were excluded. Baseline data, including age, sex, body mass index (BMI), relevant comorbidities, and time from admission to surgery, were collected for all patients.
IIC and IOC
Among patients in the IIC group, a urinary catheter was inserted immediately upon hospital admission and kept in place until 24 h after surgery. Urine specimens were collected for urinalysis (UA) and urine culture (UC) at two time points: at admission (via catheter) and at 24 h postoperatively upon catheter removal. Meanwhile, among patients in the IOC group, UA and UC were performed using the midstream urine sample technique. Hip fracture operation including fracture fixation and hemiarthroplasty was performed under spinal anesthesia by a specialized hip surgeon team within 48 hours after admission. On the day of surgery, in patients in the IOC group, a urinary catheter was inserted after anesthesia. Then, the urinary catheters in both groups were removed at 24 h postoperatively, and urine samples were collected for UA and UC. POUR was assessed within 6 h after catheter removal. If patients were unable to void independently, had a distended bladder on physical examination, or had a post-void residual volume exceeding 400 mL, they were diagnosed with POUR. 20 Finally, UTI was confirmed based on postoperative UC, and bacteriuria was defined as the presence of ≥105 colony-forming units per milliliter (CFU/mL)) bacteria in urine. 21
Statistical Analysis
Data were analyzed using SPSS version 27 software (SPSS Inc., IL, USA). The sample size was calculated based on previous studies reporting postoperative UTI incidences.22,23 Using a two-sided test for comparing two proportions, with an alpha error of 0.05 and 90% power, the minimum sample size was calculated to be 50 patients per group. After accounting for the potential loss to follow-up, a total of 110 patients (55 per group) were enrolled. Continuous variables are presented as mean ± standard deviation (SD), and categorical variables are presented as frequencies and percentages. Differences in baseline characteristics were analyzed using an independent t-test for continuous variables and a chi-square test for categorical variables. The incidence of postoperative UTI and POUR between groups was compared using the chi-square test. A P-value of <.05 was considered statistically significant, and the results are presented with 95% confidence intervals.
Results
Patient Characteristics
Demographics Data and Baseline Characteristics of the IIC and IOC Groups
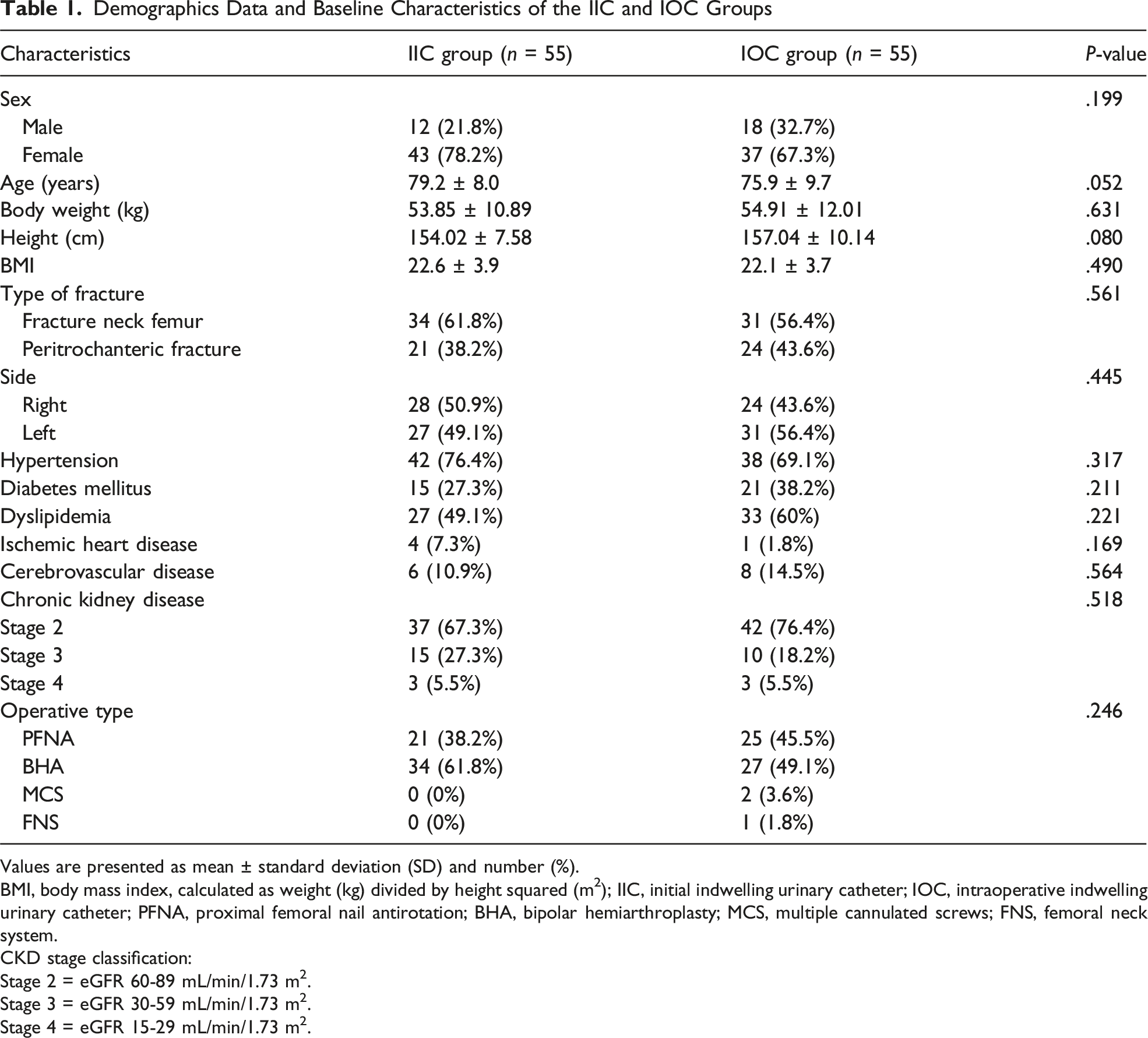
Values are presented as mean ± standard deviation (SD) and number (%).
BMI, body mass index, calculated as weight (kg) divided by height squared (m2); IIC, initial indwelling urinary catheter; IOC, intraoperative indwelling urinary catheter; PFNA, proximal femoral nail antirotation; BHA, bipolar hemiarthroplasty; MCS, multiple cannulated screws; FNS, femoral neck system.
CKD stage classification:
Stage 2 = eGFR 60-89 mL/min/1.73 m2.
Stage 3 = eGFR 30-59 mL/min/1.73 m2.
Stage 4 = eGFR 15-29 mL/min/1.73 m2.
Incidence of UTI and POUR in the IIC and IOC Groups

Values are presented as number (%). *Statistically significant (P < .05).
UTI, urinary tract infection; POUR, postoperative urinary retention; IIC, initial indwelling urinary catheter; IOC, intraoperative indwelling urinary catheter.
Incidence of Postoperative UTI and POUR
Thirteen patients (23.6%) in the IIC group developed UTI compared with five patients (9.1%) in the IOC group, representing a statistically significant difference (absolute risk reduction 14.5%, 95% CI: 0.7 to 28.4; P = .039, Table 2). The calculated number needed to treat was 6.87, which indicated that treating approximately 7 patients with intraoperative catheterization, instead of initial catheterization, would prevent one UTI case. For POUR, no statistically significant difference was observed between the groups; 9 patients (16.4%) in the IIC group and 5 patients (9.1%) in the IOC group showed POUR (P = .252, Table 2).
Univariate and Multivariate Logistic Regression Analyses Results

BMI, body mass index, calculated as weight (kg) divided by height squared (m2); IIC, initial indwelling urinary catheter; IOC, intraoperative indwelling urinary catheter. *Statistically significant (P < .05).
UTI Cases With Antibiotic Treatment

Discussion
A prospective, randomized controlled trial was conducted to compare the incidence of UTI and POUR in the IIC and IOC groups of elderly patients undergoing early hip fracture surgery. The IIC group showed a higher incidence of UTI than the IOC group, whereas the incidence of POUR was not significantly different between the two groups. These results suggest that delaying catheter insertion until intraoperative timing reduces UTI risk without increasing POUR incidence.
UTI is a common complication in elderly patients with hip fractures.22,24 Whether indwelling urinary catheterization should be performed immediately at admission or intraoperatively before surgery is a subject of debate, with no universally accepted standard protocol regarding optimal timing.15,25 At our institution, all patients with hip fracture undergo surgery within 48 h of hospital admission, which is consistent with recommendations from a previous study advocating early surgery to reduce UTI risk. 26
Our logistic regression analysis confirmed that initial catheterization was an independent predictor of UTI, even after adjusting for potential confounders. The peritrochanteric fracture type was also found to be independently associated with an increased UTI risk. These results strengthen the inference that earlier catheterization contributes to a higher risk of infection, likely due to prolonged catheter dwell time and an increased opportunity for bacterial colonization. No factors were found to be significantly associated with POUR in a multivariate analysis.
Few studies have reported findings similar to ours. Bliemel et al. found that indwelling catheters on admission in 24% of surgically treated geriatric hip fracture patients resulted in a UTI. 27 Thus, the use of indwelling for the shortest time possible (24-48 h) may be beneficial to reduce the risk of UTIs.28,29 This finding was consistent with that of previous studies suggesting that prolonged catheterization increases the risk of UTIs in hip fracture patients because of extended exposure to bacterial contamination.12-18 Consequently, these results highlight the importance of minimizing catheter duration to mitigate UTI risk. In the present study, even POUR was higher in the initial catheter group (16.4%) than in the intraoperative group (9.1%); however, it was not statistically significant (P = .252). POUR remains a major concern as it can lead to discomfort, bladder distention, and increased morbidity. 30 Steven et al reported that patients who were subjected to indwelling catheterization before hip fracture surgery experienced less pain and reported convenience with voiding, without an increase in POUR rates, compared with those subjected to intermittent catheterization.{Papp, 2024 #363}
Prolonged duration of the urinary catheter in the IIC group might be the reason for higher UTI incidence compared with the IOC group, even when the operation was performed within 48 h. Initial urinary catheter or IIC can easily monitor fluid intake and urine output, thereby aiding in patient’s nusing care. However, it is associated with the risk of CAUTI and can cause discomfort in patients and predispose them to the risk of urinary trauma. In contrast, IOC remains a commonly preferred practice in many hospitals as part of patient preparation. In addition, if urinary catheterization can be avoided initially at admission, CAUTI can be avoided. Moreover, in our study, the urinary catheter was removed within 24 h postoperatively to facilitate early rehabilitation. In a meta-analysis by Zhang et al, early removal of indwelling catheter in patients undergoing total joint arthroplasty (24-48 h) prevented UTI. 19 Cacciatore et al. reported that harmonized evidence regarding perioperative urinary catheterization management in older patients with hip fracture is lacking. 25 The findings of the present study suggested that patients who are able to mobilize immediately after undergoing hip surgery have a lower tendency to develop UTI and POUR than those who are unable to mobilize early.
Among hip fracture patients undergoing surgical prodcedure, intraoperative urinary catheterization should be perfomed for reducing of UTI without significant POUR. Our study was a randomized controlled trial that provided high-quality evidence by minimizing bias and confounding factors. Furthermore, the groups were well-balanced in terms of baseline characteristics. In addition, the fast-track protocol ensured standardized care without delay operation. This study had several limitations. First, the sample size was relatively small, which may have limited the statistical power to detect differences in secondary outcomes; however, UTI was explained. Second, the follow-up period was only immediate postoperative phase, which may have led to overlooking of late-onset UTIs or delayed urinary issues. Third, while our findings suggest that intraoperative catheterization is beneficial, specific patient subgroups such as those with pre-existing urinary conditions may still benefit from early catheterization. Finally, this was a single center study; thus, the generalizability of the findings to other settings with different policy is limited. To overcome this limitation, the hip fast tack protocol was used for standardization of the treatment policy.
In conclusion, intraoperative urinary catheterization is associated with a lower incidence of UTIs compared with initial catheter placement, without a significant increase in POUR. Further studies with larger sample sizes and longer follow-up are recommended to validate these findings and support clinical decision-making.
Footnotes
Acknowledgements
The authors acknowledge the financial support provided by the Navamindradhiraj University Research Fund.
Ethical Considerations
This study was conducted in accordance with the ethical standards outlined in the 1964 Declaration of Helsinki and the regulations of the U.S. Health Insurance Portability and Accountability Act (HIPAA). Ethical approval was obtained from the Institutional Review Board of the Faculty of Medicine (COA number: 105/2566). The study was prospectively registered in the Thai Clinical Trial Registry (TCTR20241231004). This prospective, randomized study was performed between June2023 and October2024.
Consent to Participate
Written informed consent was obtained from all participants prior to their inclusion in the study.
Author Contributions
P.N. and N.H. conceptualized and designed the study protocol. P.N. drafted the manuscript as the first author, while N.H. served as the corresponding author. I.O. performed data collection alongside N.H., and P.N. conducted data analyses. N.H. and I.O. validated the analysis results. All authors contributed to the manuscript revision, approved the final draft, and agreed to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Navamindradhiraj University Research Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed in this study are available from the corresponding author upon reasonable request.