
Abstract
Introduction
The optimal surgical treatment for Vancouver B2 and B3 fractures has not been determined, and bone defects and delays in fracture healing significantly affect treatment outcomes. Some authors have argued that when a serious bone defect is present, the use of cortical strut allografts for the treatment of type B2 and B3 periprosthetic femoral fractures (PFFs) after hip joint replacement may be beneficial. This study aimed to determine the usefulness of cortical strut allografts based on mid-to long-term clinical radiologic results after surgical treatment of Vancouver B-type PFFs.
Methods
We retrospectively reviewed the outcomes of 48 patients with postoperative PFFs. The mean duration of follow-up was 6.7 years. The 22 patients were treated with cortical strut allograft. Each case was characterized and described in detail, including the length of allograft and the union period, and possible correlations between allograft length and strut-to-host bone union were analyzed. Clinical evaluations included Parker mobility and Harris hip scores. At the final follow-up, we assessed the radiological results using the Beals and Tower’s criteria, stem subsidence, and fracture union time.
Results
All 48 fractures united at an average of 21.5 weeks, and strut-to-host bone union was typically observed within 32 months. No positive correlation was identified between the allograft length and incorporation period. There was one deep infection and four cases of dislocation, but there was no fracture or malunion of the cortical strut allografts. No evidence of femoral loosening was observed in any of the patients.
Conclusion
Cortical strut allografts used to treat type B PFFs showed high rates of bone union and survival. In mid-to long-term follow-up, the cortical strut allograft length did not affect to incorporation time. The author concluded that cortical strut allografts are useful treatment for PFFs regardless subtype classification of the Vancouver type B.
Keywords
Introduction
Recent increases in the number of hip replacements have resulted in parallel increases in total hip revision surgeries and periprostatic femoral fractures (PFFs).1,2 Unlike general fractures, PFFs can be unstable, making internal fixation difficult. Therefore, special attention is required to treat PFFs. Accordingly, considerable effort has been made to accurately classify and determine the optimal treatment for these fractures.
Analysis of the Postoperative Periprosthetic Femoral Fractures.

Since they were first described by Penenberg in 1989, cortical strut allografts have been used as a major fixing method for B1-and C-type PFFs, or as an auxiliary fixing method when metal plates are used. 5 Furthermore, the use of cortical strut allografts provides advantages in terms of PFF fixation, restoration of partial femoral defects, redirecting stress, and stabilizing proximal femoral allograft-host junctions.
Accordingly, some authors have argued that when a serious bone defect is present, the use of cortical strut allografts for the treatment of type B2 and B3 PFFs after hip joint replacement may be beneficial.6,7 The optimal surgical treatment for Vancouver B2 and B3 fractures has not been determined, and bone defects and delays in fracture healing significantly affect treatment outcomes. Recent studies have demonstrated that prosthetic loosening is the most important mid-to long-term problem after Vancouver B2 or B3 surgery. 8 This study aimed to determine the usefulness of cortical strut allografts based on mid-to long-term clinical radiologic results after surgical treatment of Vancouver B-type PFFs.
Methods
Study Population
Fifty-two patients with Vancouver type B PFF were treated at INHA University Hospital by internal fixation or revision arthroplasty with or without cortical strut allografts from December 2001 to December 2020. Four patients were died during follow up. Fourty eight of these patients [14 men (29%) and 34 women (71%); average age 76.79 (±13.46 years)] were followed up for at least 2 years and constituted the study cohort. The average follow-up period was 6.7 years (range, 2.3-13.8 years). The average patient BMI was 23.54 kg/m2 and the average BMD was a T-score of −3.3. Prior to PFF, these patients cumulatively underwent 6 total hip replacements, 42 hemiarthroplasties, and 4 cemented and 44 cementless stems were implanted. Four cases were used cemented stems in primary THA, but all revised stems were used uncemented. All surgeries were performed by the senior author.
Classification and Operation
PFFs were classified using the Vancouver system; 32 and 14 patients were classified as Vancouver type B1 or B2, respectively, and 2 patient was classified as Vancouver type B3 (Table 1). In general, Vancouver type B1 patients were treated with internal fixation, B2 patients underwent revision arthroplasty, and type B3 patients underwent revision arthroplasty and supplementary internal fixation.
3
However, in our study, 16 of 32 Vancouver B1 patients underwent only internal fixation, and the remaining 16 patients underwent cortical strut allograft and internal fixation (Figure 1). A 43-year-old male patient suffering from a periprosthetic fracture resulting from a fall underwent open reduction, internal fixation and cortical strut allograft. (A) Preoperative X-ray reveals a Vancouver type B1 fracture. (B) Anterior posterior and axial views of the femur following open reduction, internal fixation and cortical strut allograft. (C) One-year postoperative X-ray showing complete incorporation.
Of the fourteen Vancouver B2 patients, 10 underwent revision arthroplasty with internal fixation and the remaining four patients underwent revision arthroplasty and cortical strut allograft (Figure 2). Two patient with Vancouver type B3 were treated with revision arthroplasty and internal fixation with cortical strut allograft placement. LCP-DF (Locking compression plate-distal femur) (Johnson & Johnson, USA, New Jersey) were used in 2 cases using strut allografts in Vancouver type B2, and LC-LCP (Limited contact-locking compression plate) (Johnson & Johnson, USA, New Jersey) curved broad were used in the remaining cases. The average number of LCP-DF holes was 11 and the length was 310 mm, and the average number of LC-LCP curved broad holes was 10.7 and the length was 238 mm. The criteria for cortical strut allograft placement were extensive bone loss during surgery, instability after internal fixation, revision arthroplasty, or a transverse fracture at the end of the stem. All strut allografts were mainly located on the medial side of femur. However, if size of strut graft was large, graft bone was covered anterior chamber too. A 76-year-old female patient suffering from a periprosthetic fracture resulting from a fall underwent Revision THA, internal fixation and cortical strut allograft. (A) Preoperative X-rays demonstrate a Vancouver type B2 fracture. (B) Anterior posterior and axial views of the femur following Revision THA, internal fixation and cortical strut allograft. (C) Complete incorporation was observed after 16 months.
Clinical and Radiologic Evaluations
Clinical Factor of Periprosthetic Femoral Fractures.

*ORIF: open reduction internal fixation.
**THRA: total hip replacement arthroplasty.
Comparison of Those Treated With or Without a Cortical Strut Allograft
Vancouver type B patients were divided into two groups based on the receipt of a cortical strut allograft (CSA (n = 22) and non-CSA (n = 26) groups), and demographic factors (sex, BMI, BMD, ASA score), clinical factors (Harris hip score, Parker mobility before and after surgery), and radiological factors (subsidence, fracture site union) were compared. Fracture union was defined as the presence of osseous trabeculae that crossed the fracture line.
Postoperative Rehabilitation
We recommended partial weight bearing in type B1, B2, or B3 after postoperative 6 weeks. However, fracture, perforation during surgery, decreased bone density, or relative unstable fixation cases were restricted weight bearing until 8 weeks after surgery.
Statistical Analysis
For categorical variables, the chi-square test was used to compare patient's demographic, clinical, and radiographic factors. For normally distributed variables, ANOVA and Student’s t-test were used. Spearman’s correlation analysis was used to evaluate the correlation between cortical strut allograft length and time to incorporation, and Kaplan-Meier analysis was used to evaluate the union rate of allografts or removal of cortical strut allografts rates. The analysis was performed using SPSS version 22.0.0, and statistical significance was accepted for P < .05. The study protocol was approved by the Institutional Review Committee of Inha University Hospital (INHAUH 2022-02-001-000).
Results
Cortical Strut Bone Length and Incorporation Time.

*ORIF: open reduction internal fixation.
**THRA: total hip replacement arthroplasty.
Demographic Factors of CSA* & non-CSA*.
*CSA: cortical strut allograft.
Regarding postoperative complications, in one case (2.0%) of Vancouver B2 fracture treated with internal fixation and a cortical strut allograft, hardware and cortical strut allografts were removed due to postoperative deep infection and then discharged under resection arthroplasty. Postoperative dislocation occurred in four Vancouver B2 fracture cases (8.3%) and was treated by manual reduction; no fractures or misalignments were found. Kaplan-Meier survival analysis showed that the survival rate for union was 95.8% (Figure 3) at the final follow-up. Kaplan-Meyer survival curve. The survival rate at the final follow-up was 95.8% when the endpoint was set as the time of nonunion and removal of cortical strut allografts.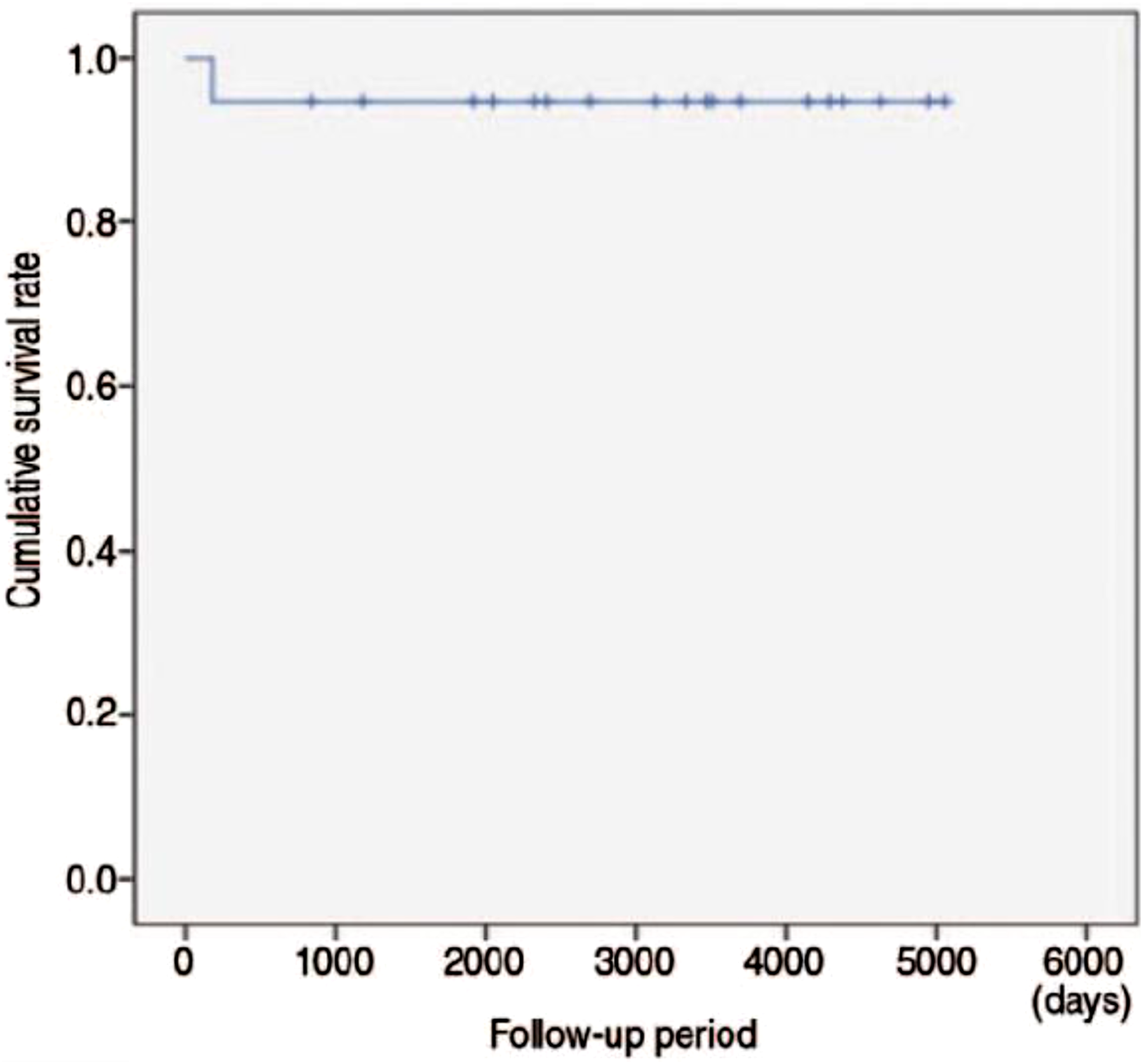
Discussion
PFFs are complex fractures that must be treated in the absence of clear agreement on appropriate fixation methods due to a lack of consensus and high-level comparative studies. Vancouver type B fractures are complex and affect the femur around the stem. The treatment objective of reconstructing Vancouver type B2 or B3 fractures is to obtain solid component stability and satisfactory restoration of the bone stock. Several studies have suggested that the use of cortical strut allografts might aid in the treatment of Vancouver type B fractures.12,13 Cortical strut allografts act as biological plates that stabilize fractures when used alone or in combination with other high-fixation devices and provide mechanical stability, enhance fracture healing, and increase bone mass in affected areas. 14 In addition, cortical strut allografts have elasticity moduli similar to those of the host bone, and thus, the stress shield of the host bone is less than that of harder internal fixation methods. 15 Hao-bo et al reported high clinical success rates and functional recoveries in five patients with Vancouver type B2 or B3 fractures treated with revision arthroplasty with cortical strut allografts. 11 Hedad et al also recommended that cortical strut allografts be used routinely to treat PFFs, based on observations of improved fixation and healing. 12 Hao-bo et al reported that the average time to union at the fracture site was 5.2 ± 1.4 months for patients treated with cortical strut allografts after revision arthroplasty. 11 In the present study, the mean time to fracture site union for the Vancouver classification types was 21.1 weeks (range, 10-36 weeks) for type B1 fractures, 22.1 weeks (range, 17-28 weeks) for type B2 fractures. For type B1 fractures within CSA group, time to fracture site union was 16.2 weeks and for B2 fractures within CSA group, time to fracture site union was 16.5 weeks. The use of cortical strut allografts resulted in faster union than that with revision alone.
Although there was a bone defect, in the group using the cortical strut allografts in type B with bone defect, the fracture site union time was shorter than that in the non-CSA group.
The cortical strut allograft length has not been previously reported to affect the time to allograft incorporation. Gross et al 16 used an average cortical bone length of 154 mm in internal fixation patients with fractures around the stem but did not mention the relationship between cortical strut length and time to allograft incorporation. In the present study, we used an average cortical strut allograft length of 167.23 mm (128-209 mm) and found no correlation between cortical strut allograft length and time to allograft incorporation.
Cortical strut allografts have been reported to be associated with infection and increased costs, 17 and the infection rate of hip arthroplasty containing cortical strut allografts is between 0% and 2%. 18 In the present study, one patient (2.0%) was discharged in the resection arthroplasty state after all implants and graft materials were removed. According to Tomford et al, the infection rate is associated with the complexity of surgery and not with cortical strut allograft placement. 19 Therefore, thorough postoperative wound management is mandatory to prevent the development of deep infections.
If osteoporosis proceeds after cortical strut allograft placement, the risk of graft-site fracture also increases. Berry et al reported that the risk of fracture at replacement sites was highest two-three years after surgery. 20 However, in the present study, no complications such as bone reabsorption or fracture occurred in the cortical strut allografts.
According to Head and Malinin, after 9.5 years of follow-up, a 97% survival rate was achieved in patients who underwent cortical strut allograft. 21 Barden et al reported that cortical strut allografts had a 100% survival rate after 4.7 years, 22 whereas Emerson et al reported a 93% survival rate at 8.4 months for cortical strut allografts at eight months. 23 In the present study, the survival rate (no infection, non-incorporation of cortical bone allografts, or bone removal) at the final follow-up as determined by Kaplan-Meier estimates was 95.8% for cortical strut allografts.
This study has several limitations. First, the number of cases reviewed was small. Additionally, the study results were interpreted by a single observer. In other words, interobserver differences in terms of time to union and degree of radiological bone union were not addressed, although it should be noted that the author was an expert in this field.
Conclusion
Cortical strut allografts used to treat type B PFFs have shown high bone union and survival rates. In mid-to long-term follow-up, the cortical strut allograft length did not affect to incorporation time. The author concluded that cortical strut allografts are a useful treatment for PFFs regardless subtype classification of the Vancouver type B.
Footnotes
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Institutional Review Committee of Inha University Hospital (INHAUH 2022-02-001-000).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the INHA UNIVERSITY HOSPITAL Research Grant.