
Abstract
Introduction
The purpose of this study was to assess the hospital quality measures and outcomes of operative hip fracture patients before and after implementation of an anesthesiology department protocol assigning decision for a preoperative transthoracic echocardiogram (TTE) to the hospitalist co-managing physician.
Materials and Methods
Demographics, injury details, hospital quality measures, and outcomes were reviewed for a consecutive series of patients presenting to our institution with an operative hip fracture. In May of 2019, a new protocol assigning the responsibility to indicate a patient for preoperative TTE was mandated to the co-managing hospitalist at the institution. Patients were split into pre-protocol and post-protocol cohorts. Linear regression modeling and comparative analyses were conducted with a Bonferroni adjusted alpha as appropriate.
Results
Between September 2015 and June 2021, 1002 patients presented to our institution and were diagnosed with a hip fracture. Patients in the post-protocol cohort were less likely to undergo a preoperative echocardiogram, experienced a shorter time (days) to surgery, shorter length of stay, an increase in amount of home discharges, and lower complication risks for urinary tract infection and acute blood loss anemia as compared to those in the pre-protocol cohort. There were no differences seen in inpatient or 30-day mortality. Multivariable linear regression demonstrated a patient’s comorbidity profile (Charlson Comorbidity Index (CCI)) and their date of presentation (pre- or post-protocol), were both associated with (P<0.01) a patients' time to surgery.
Conclusion
A standardized preoperative work flow protocol regarding which physician evaluates and determines which patients require a preoperative TTE allows for a streamlined perioperative course for hip fracture patients. This allows for a shortened time to surgery and length of stay with an increase in home discharges and was associated with a reduced risk of common index hospitalization complications including UTI and anemia.
Introduction
Hip fractures remain a major public health concern as a result of the aging population and recent growth in elderly populations. 1 From 2010 to 2020, there was a 4.7% increase (18.2% to 22.9%) in people over the age of 60 in the United States.2,3 Similarly, the proportion of the US population expected to be older than 60 in 2050 is projected to double from the population seen in 2010 (40.2 million to 88.5 million Americans). 4 Among elderly patients, hip fractures are more common and especially more likely to result in morbidity, mortality, and loss of independence.5,6 Additionally, older patients often also have associated medical comorbidities that can lead to a worse prognosis.7,8 As such, hip fracture incidence has increased in recent years, highlighting the importance of proper care and management of patients in this particular population. 9 Operative treatment via fixation or arthroplasty remains the standard of care for the majority of patients who sustain hip fractures. 10
Cardiovascular disease is highly correlative to age, and therefore very prevalent in older patient populations.11,12 It is estimated roughly 70–75% of individuals 65 and older have some form of cardiovascular disease, with 82% of all deaths in people aged 65 or older being attributable to cardiovascular disease.13,14 In addition to the high prevalence and associated risk of morbidity and mortality for patients with cardiovascular disease at baseline, cardiac events are currently one of the most common complications after hip fracture surgery. 15
Transthoracic echocardiogram (TTE) is a noninvasive imaging modality used to assess the structure and function of the heart. Given the operator dependent nature of obtaining the imaging and routine need for cardiologist evaluation, utilization of a preoperative TTE has been demonstrated to prolong time to surgery and subsequently increase perioperative mortality risk and associated healthcare costs in hip fracture patients.16,17 Despite this, many physicians routinely utilize a preoperative TTE for perioperative assessment of moderate to higher risk cardiovascular patients in hopes of improved medical optimization. This may include patients with moderate or severe clinical valvular pathology (stenosis, regurgitation) and recent clinical symptoms or no recent TTE, and other high-risk patients with poor functional capacity deemed to benefit from cardiac stress testing in particular. Both are recommended to undergo preoperative TTE in accordance with guidelines constructed by the American College of Cardiology/American Heart Association (ACC/AHA).18,19 These have shown to be effective, especially in orthopedic patients, although there remain challenges in the proper adherence and execution across different specialties.20,21 Therefore, the implementation of standardized protocol to appropriately abide by these guidelines and assess preoperative cardiovascular risks remains of interest.
The purpose of this study was to assess the hospital quality measures and clinical outcomes of patients undergoing hip fracture repair or arthroplasty surgery before and after implementation of an anesthesiology department protocol assigning the Hospitalist co-management service to determine need for a preoperative transthoracic echocardiogram, compared to the prior arrangement where the need for preoperative TTE evaluation was at the discretion of the patient’s medical doctor or attending anesthesiologist providing anesthesia during the case.
Materials and Methods
A consecutive series of 1002 patients presenting with a hip fracture [AO/OTA 31A, 31B, and 32A-C] between September 2015 and June 2021 were evaluated at one orthopedic specialty hospital. Treatment options for each patient included arthroplasty or operative fixation. Demographics, injury details, hospital quality measures, and outcomes were collected for each patient. Patients were excluded if they underwent non-operative management.
Prior to the new policy, individual anesthesiologists, medical doctors and or private cardiologists would make recommendations regarding the need for a pre-operative TTE as part of the medical clearance prior to hip fracture surgery. On May 22, 2019, the Department of Anesthesiology developed and instituted a new policy that mandated the responsible co-managing hospitalist, with or without cardiology input, to provide the final decision for which patients would require a preoperative TTE as part of the medical optimization for each patient. Based on this new protocol, two cohorts, those who presented before the mandate (pre-protocol), those who presented after (post-protocol) were created.
The following baseline demographic data were collected: Age, sex, race, AO/OTA fracture classification, Glasgow Coma Score (GCS), Abbreviated Injury Score (AIS), ambulatory status before presentation, and medical comorbidities measured by the Charlson Comorbidity Index (CCI). Hospital quality measures collected included what type of fixation they received, time to surgery, length of stay, need for a higher level of care, and whether they were discharged home or not (home discharge including home independently and home with home health aide/assistance). Outcomes collected included inpatient and 30-day mortality, as well as inpatient complications. Complications collected include the development of sepsis, pneumonia, DVT/PE, myocardial infarction, acute renal failure, stroke, surgical site infection, decubitus ulcer, urinary tract infection (UTI), acute respiratory failure, anemia, or cardiac arrest. Finally, patients that underwent a preoperative transthoracic echocardiogram were collected.
Baseline demographics, injury details, hospital quality measures, and clinical outcomes were compared between the pre-protocol and post-protocol cohorts using chi-square tests, independent samples t-tests, and Mann–Whitney U tests with a Bonferroni adjusted alpha as appropriate. Multivariable analysis was completed using time to surgery as the dependent variable. Independent variables included age, female gender, high energy mechanism of injury (MOI), GCS, CCI, and whether the patient presented after the mandate was instituted (part of the post-protocol cohort).
Results
Demographics.
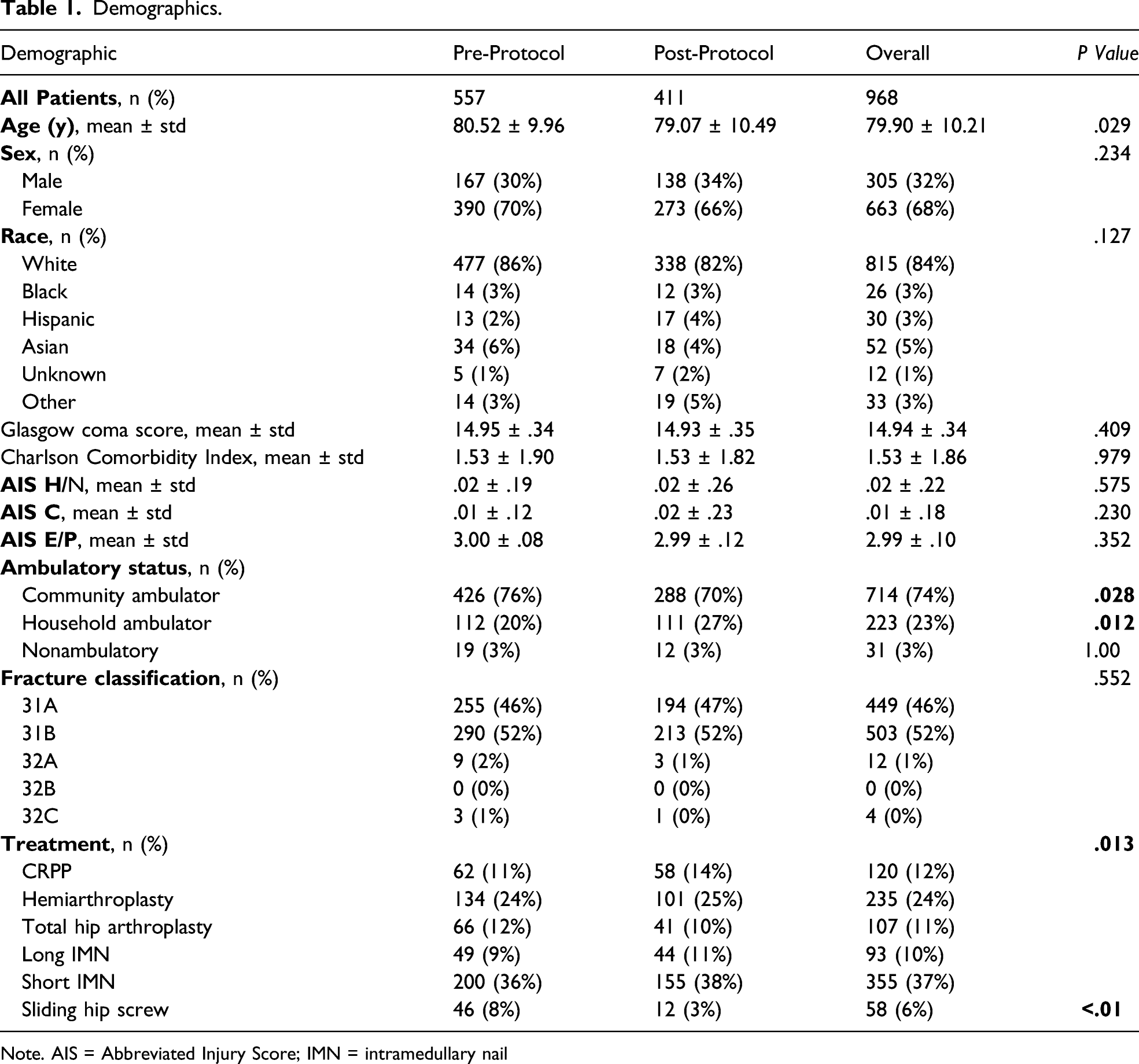
Note. AIS = Abbreviated Injury Score; IMN = intramedullary nail
Across both cohorts, the demographics were similar in regards to sex, race, GCS, CCI, AIS H/N, AIS C, AIS E/P, and AO/OTA fracture classification. Patients in the post-protocol cohort were younger (79.07 vs 80.52, P = .029), less likely to be a community ambulator (70% vs 76%, P = .028), and more likely to be a household ambulator (27% vs 20%, P = .012).
Outcomes.


Control chart (c-chart) showing number of cases with time from admission to surgery >24 hours before and after the protocol demonstrating the decrease in mean number of cases >24 hours.
Multivariable Regression for Time to Surgery.

Discussion
In this study, we compared the hospital quality measures and outcomes, most notably time to surgery, length of stay, need for an advanced level of care, and discharge home, among hip fracture patients who presented before or after an anesthesiology department mandate co-managing hospitalists would provide the final decision for which patients should undergo a preoperative transthoracic echocardiogram (TTE). For those in the post-protocol cohort, there were significant decreases in the number of patients undergoing a preoperative TTE, a shorter time to surgery and length of stay with significant increases in the amount of people discharged home despite a greater proportion of home vs community ambulators. Similarly, the post-protocol cohort also had a lower complication risk for urinary tract infections, and acute blood loss anemia during their hospitalization. The latter is likely related to the quicker turn around to surgery, faster rehabilitation, and greater home discharge.
Preoperative echocardiograms in patients undergoing non-cardiac surgery are associated with increased time to surgery.16,17 Preoperative TTEs are obtained as they can induce changes in medication, anesthetic choice, or illuminate need for additional workup.22-24 Therefore, it is hard to determine whether the surgical delay is due to the TTE itself or these associated alterations to the patient’s management. It is likely a combination. However, the lower rate of TTE with no evidence of increased postoperative cardiac and non-cardiac complications likely represents a previous standard of “overtesting.” The common use of preoperative echocardiograms in population studies further demonstrates their widespread usage and the need to optimize their inclusion in a patient’s management.25,26 Preoperative TTE may be necessary in certain patients; however, obtaining them in patients unnecessarily can increase time to surgery, length of stay, hospital costs, and potentially result in harm to the patient. Despite the ACC/AHA guidelines for perioperative assessment, studies have demonstrated that adherence to these guidelines can be a challenge when physicians from multiple specialties are involved in the care of the patient.21,27,28 Our study demonstrated the institutional implementation of a set protocol for co-managing hospitalist faculty to determine which patients should undergo preoperative echocardiograms rather than leave it up to various stakeholders, helped minimize this negative impact.
Our study demonstrated a shorter average length of stay in the post-protocol cohort. It is important to note the backdrop of the COVID-19 pandemic in spring 2020 (many of the post-protocol cohort patients) placed a large burden on the healthcare system, resulting in worse outcomes and hospital quality measures, notably, increased mortality rates and longer hospitalizations.29,30 The cause of this shortened length of stay is likely 3-fold. First, the protocol reduced the time to surgery which has been previously demonstrated to reduce overall length of stay and allow for more rapid rehabilitation and improvement in functional outcomes.31-35 Second, patients who presented following the protocol experienced lower complication rates of UTIs and acute blood loss anemia. Studies demonstrate both hospital-acquired urinary tract infections and perioperative anemia prolong length of stay.36,37 Therefore, our lower complication rate profile aligns with a shorter length of stay. Third, the protocol has caused a reduction in the amount of preoperative TTEs that are ordered, highlighting a more selective process that targets more at risk patients. This reduces the total burden of preoperative TTEs to allow for high-risk patients to get theirs much faster, and for lower-risk patients to proceed to surgery without the hassle of extra preoperative imaging. Our institution also has a standardized hip protocol that provides for a proactive assessment when needed as opposed to a reactive assessment based on what an anesthesiologist says preoperatively.
The proportion of patients undergoing a preoperative TTE dropped extensively in the post-protocol cohort with patients being 3.5x less likely to undergo a preoperative TTE. Similarly, the post-protocol cohort experienced a 1.5x higher rate of discharge home than pre-protocol cohort. While it is well documented that the COVID-19 pandemic played a role in the reduction of patients discharged to skilled nursing facilities instead of home, this is likely only part of the cause. The shortened time to surgery, length of stay, and lower complication rate both likely allowed for a larger proportion of patients to be discharged home.
The association between time to surgery and postoperative complications is well studied in the literature. 38 Our study demonstrated a significant reduction in the complication rates for urinary tract infections and acute blood loss anemia in all patients that presented after the protocol. Davis et al. also observed a trend towards lower UTI rates with shorter times to surgery, although this was not found to be significant. 39 Acute blood loss resulting in perioperative anemia without appropriate and timely management has been shown to worsen outcomes in hip fracture patients. 40 Our study demonstrates streamlined preoperative management allows for a shorter time to surgery and reduced risk of anemia, highlighting a proactive measure that can be taken to mitigate the effects of perioperative anemia on patient outcomes. As discussed previously, a faster time to surgery allows for more rapid rehabilitation prior to earlier discharge, lowering the risk of these common postoperative complications.
This study has several limitations. First, it is retrospective in nature. However, prospective study assessing the mandate’s impact is challenging as the mandate has already been instituted with downstream effects clearly apparent. Second, the onset and persistence of the COVID-19 pandemic during the post-protocol time period may have altered the hospital quality measures and outcomes seen within patients. The improved hospital quality measures and better outcomes seen in the post-protocol cohort demonstrate the pandemic’s impact may be minimal. Third, management changes prompted by each preoperative TTE are not characterized. This prevents an idea of what further inpatient management decisions can be expected in patients who undergo preoperative TTE. Fourth, there is no explicit recognition of which actions hospitalist faculty were more or less likely to pursue as compared to anesthesiologists or other providers, making it hard to generalize and compare to other protocols designed for streamlining the determination of which patients should undergo preoperative TTE. Fourth, there is no explicit recognition of cases where hospitalist faculty opted for a cardiology consultation to assist in the preoperative work up for the patient. The viewpoint of each specialty on certain patient presentations could help further illicit the improvements and changes in management that occurred as a result of the mandate.
In conclusion, our Department of Anesthesiology’s decision to implement the mandate authorizing co-managing hospitalist faculty to decide which patients required a preoperative TTE improved many aspects of our hip fracture patient’s care. We saw significant decreases in surgical wait times and length of stay, with a higher proportion of patient’s discharged home. While hard to directly attribute to the shorter admissions and faster time to surgery, patients presenting after the protocol also experienced a lower risk for common inpatient complications such as UTIs and anemia. The improvement seen by our institution may be an example for others to implement a similar protocol in hopes of offsetting the expected delays in surgery due to obtaining preoperative echocardiograms which can be unnecessary at times and potentially result in worsened perioperative outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.