
Abstract
Introduction:
Although there is evidence of improved functional outcomes with our “integrated care pathway” for geriatric hip fractures, we do not know if there is a significant difference in functional recovery of activities of daily living and attainment of independence in self-care between patients who underwent fixation and those treated with arthroplasty.
Objective:
To determine whether such a difference exists in surgically fixed hip fractures.
Materials and Methods:
Patients with hip fracture treated surgically were divided into group A (internal fixation, n = 213) and group B (arthroplasty, n = 199). Demographic data, Charlson comorbidity index (CCI) score, time to surgery, and length of stay were recorded. Inpatient complications and mortality rates were also documented. Modified Barthel Index (MBI) scores were recorded for the following intervals: prefall, discharge, 6-month, and at 1-year follow-up.
Results:
The mean age (A: 80 years and B: 81years), CCI (A: 5.41 and B: 5.43), and length of stay (A: 13.6 days and B: 15.2 days) were not significantly different. However, there was a significant difference (P < .05) in time to surgery (A: 102.2 hours and B: 86.6 hours). Complication rates were about 6% in both groups (A = 6.57%: urinary infections = 13, wound infections = 1 and B = 6.03%: urinary infections = 10, wound infections = 1, pressure ulcer = 1). The preinjury MBI scores were significantly different (P < .05; A: 91.65 and B: 88.19), however, there was no significant difference in scores measured at discharge (A: 60.79 and B: 59.39), 6 months (A: 77.65 and B: 77.47) and 1 year (A: 80.71 and B: 83.03). Patients who underwent surgery for hip fracture had overall recovered 90.9% of their preinjury function (overall MBI at 1 year: 81.83).
Conclusion:
The MBI scores reflect the extent of attainment of independence in self-care, and actual functional recovery is gauged from the percentage of recovery of preinjury function at 1 year postsurgery. We conclude that the type of surgery may not be a significant factor in determining independence in self-care although patients who had arthroplasty had recovered more function at 1 year postsurgery than those who underwent fixation (percentage recovery of preinjury function—A: 88.1% and B: 94.1%).
Introduction
Functional recovery post hip fracture is an important outcome measure as it provides independence in mobility in the elderly patients. Studies have also shown that age is not a factor influencing the functional outcome, 1 and significant prefracture (preinjury) function can be regained after surgery in the elderly patients. We hypothesize that patients undergoing arthroplasty after a neck of femur fracture will have a similar functional recovery and independence in self-care at 1 year postsurgery compared to those treated with internal fixation for pertrochanteric fractures in the presence of a well-established orthogeriatric model of care. Hence, the objective of the study is to determine whether the Modified Barthel scores as a measure of functional independence are similar in both situations and if not, does a significant difference exist. We have also considered the overall results of our surgically fixed hip fractures to gauge the effect of our integrated pathway on surgically treated hip fracture functional outcomes.
Materials and Methods
The implementation of the Integrated Care Pathway for hip fracture management began in October 2011. The goal was to achieve uniformity in care, early surgical intervention, minimize complications, and maximize the rehabilitation efforts to restore a preinjury functional status. 2–6 Geriatric patients who were admitted to the orthopedic department with fragility hip fractures were included in the pathway. Patients with cognitive impairment were excluded from the study. Majority of the patients came from their own homes. The patients were prospectively divided into 2 broad fragility fracture groups—intertrochantric (group A) and neck of femur fractures (group B), which are treated very differently with surgery—the former with fixation by a sliding hip screw or a proximal femoral nail and latter with an arthroplasty (hemi or total replacement). The difference in functional outcomes between these 2 groups was analyzed.
We excluded patients less than 60 years of age, those with pathological hip fractures, and those with multiple injuries. Demographic details, Charlson comorbidity index (CCI) score, time to surgery, and length of stay (LOS) was documented. Complications and mortality were also documented. Modified Barthel Index (MBI) scores were recorded for preinjury function and for postoperative intervals including at discharge, at 6 months, and at 1 year follow-up. The MBI scores between intervals in respective groups were used as an outcome measure of functional recovery in activities of daily living (ADLs) based on percentage scores with the reported preinjury scores being the baseline. The scores at each interval were then compared between the 2 groups. Statistical analysis was performed using SPSS version 15.0. All data were recorded based on hospital charts, direct assessment of patient during hospital stay, and follow-up and telephonic consultations.
Rehabilitation in our model of care is initiated preoperatively, and mobilization is started immediately postoperatively, and the patient’s progress is monitored daily by physiotherapist and an occupational therapist. Therapy facilities are available in our dedicated hip fracture ward, and this facility avoids unnecessary delay caused by transportation to a separate therapy department. The pathway begins from the emergency department and is followed through discharge until a follow-up at 1 year for functional scoring.
Results
The study included a total of 412 patients (group A = 213 and group B = 199) who underwent surgical treatment for a hip fracture and were followed up for a period of 12 months. The mean age for group A was 80 years and the mean age for group B was 81 years (P = .05). Both groups had a female predominance (75%). The CCI score was used for estimation of the comorbid status. The mean CCI with consideration of “age” was 5.41 (group A) and 5.43 (group B), respectively, that was not significantly different. The mean time to surgery was significantly shorter in group B (86.6 hours) compared to group A (102.2 hours). The mean LOS was 13.7 days in group A compared to 15.3 days in group B with no significant difference. Complications rates were about 6% in both groups (A = 6.57%: urinary infections = 13, wound infections = 1; and B = 6.03%: urinary infections = 10, wound infections = 1, and pressure ulcer = 1; Figures 1 and 2).
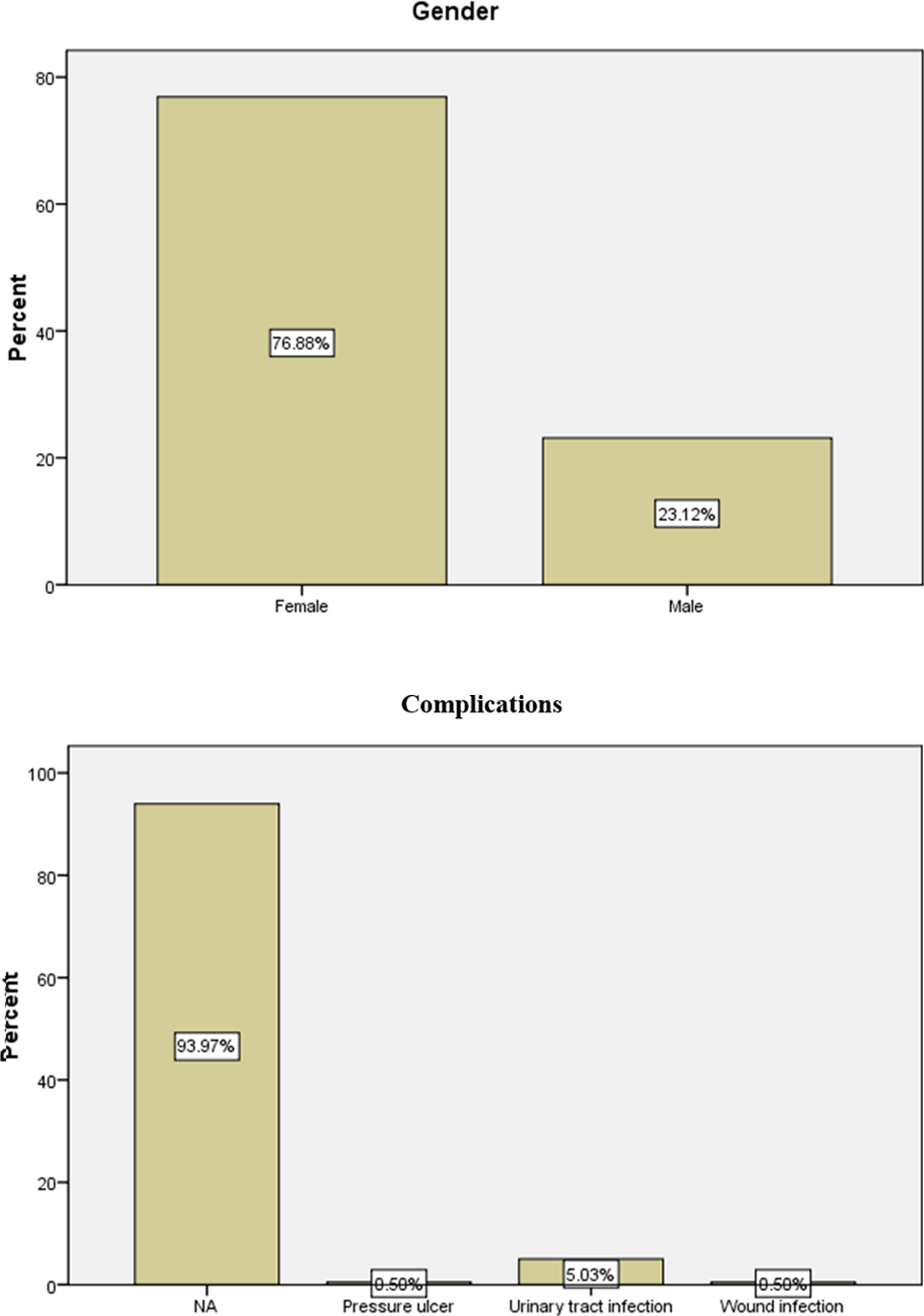
Fixation (group A).
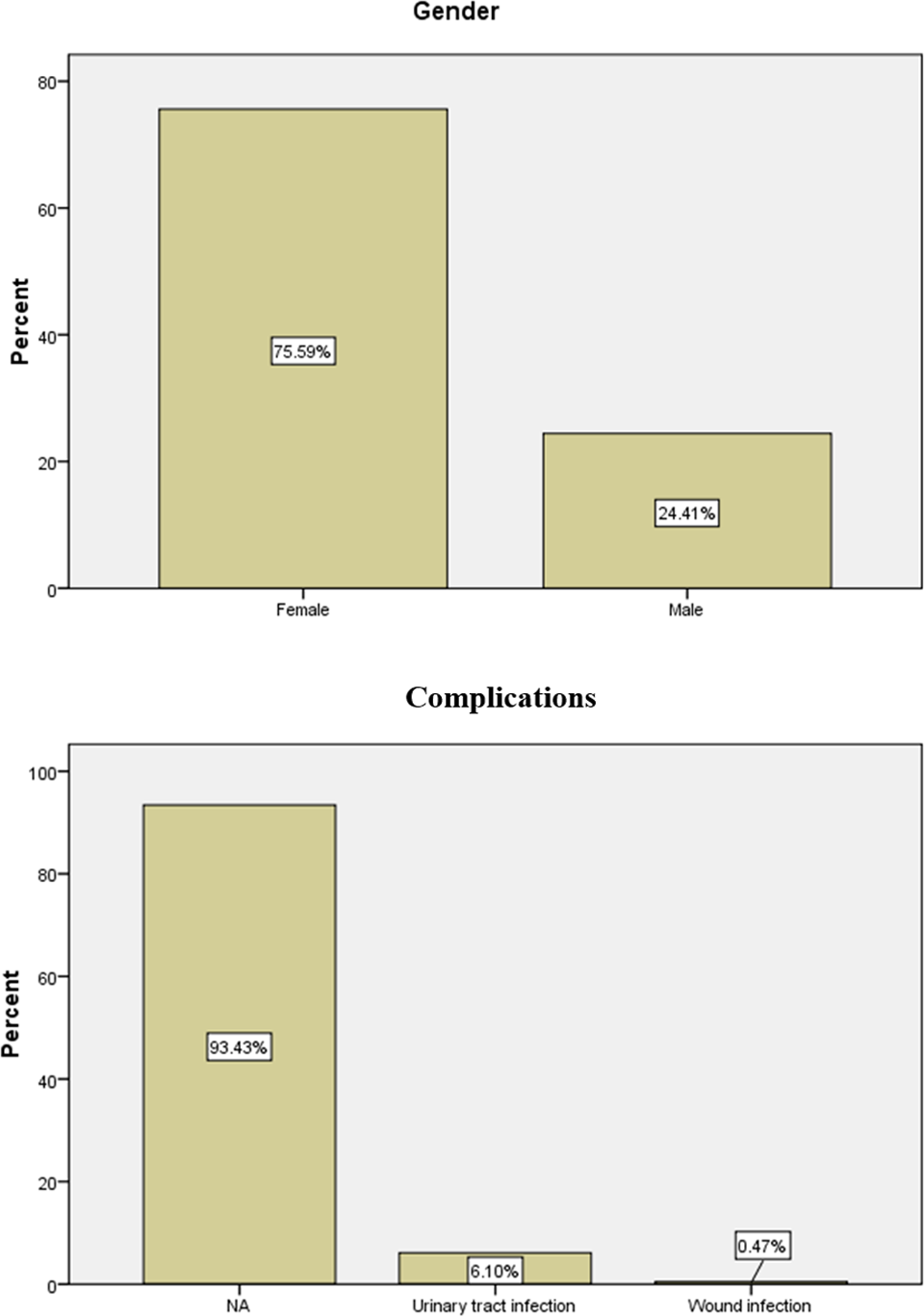
Arthroplasty (group B).
The mean functional preinjury MBI scores were significantly higher (P < .05) in group A (91.65) compared to group B (88.19). Postsurgery, group A had consistently higher scores at discharge (A = 60.79 and B = 59.39) and at 6 months (A = 77.65 and B = 77.47), but the difference was not statistically significant. However, both groups had comparable independence in self-care at 1 year postsurgery as evidenced from the similar Barthel scores—group B (83.03) compared to group A (80.71) but again was not found to be statistically significant (Figure 3 and Table 1). But group B achieved a significantly higher functional improvement of 94.1% of preinjury function compared to 88.1% improvement in group A (Figure 4 and Table 2).

Comparison of Barthel scores of fixation and arthroplasty.

Comparison of recovery patterns of fixation and arthroplasty.
Patient Characteristics and Outcome Parameters.

Abbreviations: CCI, Charlson comorbidity index; NS, not significant.
Improvements in Mean MBI Scores at Time Intervals.

Abbreviation: MBI, Modified Barthel Index.
Combining the individual arthroplasty and fixation groups, we were able to arrive at the overall functional outcomes of all our surgically treated hip fractures. The mean age of a hip fracture patient was 80.8 years, the mean waiting time for surgery was 94.87 hours, and the mean Charlson score was 5.42. The MBI preinjury score was 89.98, and patients were able to attain 90.9% of their preinjury function at 1 year postsurgery (mean MBI score at 1 year was 81.83; Table 3).
Overall Analysis of Results of 1-year Hip Fracture Study.

Discussion
With better health care leading to longevity, the focus for our aging population now is on adding “quality of living” to years of life. 7 Independence in walking and ability to perform “activities of daily living” are important in achieving the above goal. Proximal femoral fractures are the most common injury sustained in falls in the elderly patients, 8 and it can adversely affect patient’s return to preinjury function even after rehabilitation.
Studies have shown significant benefits in surgical treatment (both fixation and arthroplasty) 9 compared to conservative management even in nonagerians 10 and centenarians. 11 A number of factors such as demographics, comorbidities, fracture characteristics, and type of surgery may possibly affect recovery. 12,13 Recognizing the extent of influence of individual factors may help us identify the characteristics of a “poor outcome cohort,” so that targeted rehabilitation would maximize gains and optimize resource utilization.
Although many studies have been done on demographic factors 14,15 and comorbidities, 16,17 the potential predictive value of fracture characteristics and type of surgery have not been sufficiently investigated. Intertrochantric fractures are fixed with sliding screw 18 or a femoral nail depending upon the degree of comminution. Neck of femur fractures are complicated by avascular necrosis and nonunion postfixation needing revision, 19,20,21 and hence the treatment of choice is arthroplasty. 22
We considered 2 important parameters when analyzing function—percentage of recovery of preinjury function at 1 year and independence in ADLs as measured by MBI scores. Studies have shown that early functional outcomes and independence in mobility predict survival at 1 year. 23,24 When a patient reaches an MBI score of 60, he or she moves from the dependent to assisted independence group and can be discharged from tertiary hospital to a nursing home or home depending on community support. Until a score of 80, patient will require a number of community services like day care services to cope. At higher scores, patient gradually regains ability to independently transfer from bed and chair and walk or use wheel chair on their own. So MBI scores help us to predict the type and amount of social services and support needed and also perform a goal-based rehabilitation aimed at independence. Also standardizing results utilizing validated 25 and easily usable 26,27 scoring systems such as Charlson scoring for comorbidities and Modified Barthel score for ADLs have reduced interobserver variation and bias making results more reliable.
Although studies have found intertrochantric fracture to be more common than neck of femur fractures as age advances, 28 the mean age for both groups in our study population was not significantly different (A = 80.4 and B = 81.4). Besides the age, it was also interesting to note that the Charlson scores (A = 5.41 and B = 5.43) were similar too. This is important as it avoids a significant bias when comparing both groups, 29 making the study an automatched cohort amenable to comparison of outcome parameters (Modified Barthel scores).
Both groups in our study had almost similar LOS, although the time to surgery for hip fractures requiring arthroplasty was significantly shorter. Most of the functional recovery occur within the first 3 to 6 months postsurgery, 30,16 and the challenge after this period is to consolidate the gains and prevent the patient from deconditioning. 14,31 So ADL scores at discharge, 6 months, and 1 year would reflect the entire spectrum of outcomes—recovery from surgery, attainment of rehabilitation goals, and consolidation of functional improvement. In our study population, we found that the scores for both groups at discharge (A = 60.79 and B = 59.39), 6 months (A = 77.65 and B = 77.47), and 1 year (A = 80.71 and B = 83.03) to be similar.
Although the preinjury functional scores were significantly higher for group A compared to group B, the recovery pattern was similar for both groups as there was no significant difference in the rate of improvement in functional score from discharge to 6 months and from 6 months to 1 year. Nevertheless, the final functional scores at 1 year were higher for group B who underwent arthroplasty though the difference was not statistically significant. With regard to percentage of improvement based on the baseline preinjury functional scores, those requiring joint replacement surgery achieved 94.1% improvement compared to 88.1% for those requiring fixation at 1 year. (Table 2 and Figure 4) The higher scores may be due to the fact that there is no role of bone healing and pain when mobilizing in the joint replacement group as compared to the internal fixation group. Nevertheless, the absence of significant difference in attainment of independence of self-care in both groups from our study cohort signifies the important benefits of the rehabilitative process that has been delivered through our integrated model of care.
Conclusion
We conclude that the type of surgery may not be a significant factor in determining independence in self-care although patients who had arthroplasty had recovered more function at 1 year postsurgery than those who underwent fixation (percentage recovery of preinjury function: A: 88.1% and B: 94.1%). Further, overall attainment of 90.9% preinjury function in surgically treated hip fractures emphasizes the importance of early surgery and effective and targeted rehabilitation through an integrated care pathway.
Limitation
The sample sizes are small to generalize outcomes, and a longer follow-up at 2 years may reveal a clearer functional result. Barthel score is a measure of functional independence and does not specifically ascertain the hip strength in totality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.