
Abstract
Introduction:
There are increasing demands to perform surgery of hip fractures without delay. However, few studies have assessed the time to surgery in relation to outcome measurements.
Methods:
A total of 643 consecutive patients with a minimum age of 60 years underwent total hip arthroplasty (THA) for an intracapsular hip fracture. For this retrospective case series, demographic data and the outcome measurements—(1) any surgical revision, (2) implant failure, and (3) mortality—were documented from a prospective clinical database. The time from admission to surgery was also documented prospectively and then data were divided into 4 groups according to the time of surgery: (1) within 12 hours, (2) >12 to 24 hours, (3) >24 to 48 hours, and (4) later than >48 hours. The study end point was 2 years after surgery. Final evaluation was conducted for any missing data through a telephone interview.
Results:
The patients comprised 456 women (70.9%) and 187 men (29.1%) with a mean age of 80.2 years (range 60-104 years; standard deviation ±7.4). Descriptive data were without effect in all 4 groups. Time to surgery did not significantly influence revision for any reason (P = .323), implant failure (P = .521), and mortality (P = .643). Cox regression analysis identified male sex (P < .001; 95% confidence interval (CI), 1.27-2.44), American Society of Anesthesiologists score ≥3 (P < .001; 95% CI, 2.12-21.59), C-reactive protein level >21 mg/L (P < .018; 95% CI, 1.09-2.60), hemoglobin level <12.0 g/dL (P = .033; 95% CI, 1.04-2.68), and dementia (P < .000; 95% CI, 1.50-2.86) as independent significant risk factors for mortality.
Conclusion:
Time to surgery had no effect on revision for any reason, implant failure, and mortality in patients undergoing THA for an intracapsular hip fracture.
Introduction
Intracapsular hip fracture is an injury that usually occurs in the elderly patients due to a benign fall and is often treated with arthroplasty. 1 Due to the increasing number of hip fractures requiring surgical treatment and the resulting medical expenses, 2,3 there are demands to perform this surgery within 24 hours, but no later than 48 hours after admission to reduce complications and the hospitalization duration. 4,5 These considerations are based on registry data including a large number of cases, showing that a delay in surgical treatment results in higher morbidity and higher mortality. 6 -9 However, registry data are usually collected on the basis of transmitted diagnostic-related group codes, which have a high potential for incorrect analyses. For example, time to surgery is often recorded to the nearest days, but not to hours. This results in less accurate times being recorded with deviations of up to 23 hours. 6 -10 Consequently, the conclusions are not rigorously or appropriately discussed. 9,11
Using a large number of cases and a homogeneous patient collective, we compared outcome measurements in 4 groups divided according to a prospective and accurate documentation of time to surgery. We evaluated the following outcome measures: (1) revision for any cause, (2) implant failure, and (3) mortality. Our hypothesis was that time to surgery would not significantly influence the outcome measures.
Material and Methods
Evaluation
This retrospective case series exclusively enrolled patients with a minimum age of 60 years who underwent total hip arthroplasty (THA) for an intracapsular hip fracture. The treatment period was from January 1, 2006, to December 31, 2014. All patients younger than 60 years and those treated with the use of devices or hemiprosthesis were excluded. Hemiprosthesis was used only for multimorbid (bedridden) patients. Polytraumatic patients and those with histologically confirmed benign or malignant pathological hip fractures were also excluded; however, those with osteoporosis-related hip fractures were included. On the basis of these criteria, we examined our prospective database that contained details of the surgeries and all outpatient consultations. Apart from demographic data (Table 1), the incidence of revision for any cause was determined. Mortality information was obtained through telephone conversations with family members or general practitioners. The end point of the study was 2 years after surgery for every living patient. Data collection also included the exact timing of the patient’s admission to the emergency department (in minutes) as well as the beginning of the surgery (time of the first surgical incision). This enabled meticulous determination of the exact surgical timing as a basis for this study analysis.
Basic Demographic Variables of the Study Patients According to Time Intervals.

Abbreviations: CRP, C-reactive protein; ASA, American Society of Anesthesiologists.
Patients and Treatment
We included 643 consecutive patients. As there were no missing data, the follow-up rate was 100% with respect to the 3 outcome measurements.
Depending on the bone structure of patients and the experience of surgeons, a total of 511 cemented, 87 partly cemented (hybrid), and 45 noncemented THA prostheses were implanted. Zimmer (Warsaw, Indiana) implant designs were used exclusively, namely, the CLS Spotorno, Müller straight stem, Durasul cemented cup, and Allofit cementless cup. In all cases, the surgical approach of Bauer et al or Watson-Jones was used. 12,13 A dorsal approach was not used in any of the cases. Endotracheal anesthesia was used in all patients. All patients received a single injection of antibiotics at the time of anesthesia administration—and no antibiotics were given postsurgery.
Definitions of Infection
For the diagnosis of an infection, positive clinical findings and microbiological detection of a pathogen according to the criteria by Parvizi et al were required. 14
Hip dislocations treated using a closed reposition were considered revisions despite conservative treatment.
Implant failure was defined as a requirement for procedures ranging from component exchange (eg, inlay or head exchange) to complete removal of the arthroplasty device (eg, Girdlestone procedure for infection control).
The study was approved by our institutional review board. Verbal consent was obtained from all contacted patients.
Statistical Methods
Statistical analyses were performed using SPSS for Windows, version 24.0 (SPSS Inc, Chicago, Illinois). Metric variables are reported as mean values, whereas measures of dispersion are reported as standard deviations. The categorical and/or nominal data are reported as absolute and relative frequencies. Metric variables were assessed for normal distribution using the Kolmogorov-Smirnov test. The tested variables were not normally distributed (Kolmogorov-Smirnov test: P < .05). Therefore, nonparametric tests were used for non-normal distribution for sample comparisons. Where the distribution was not normal, the Mann-Whitney U test was used to compare 2 independent samples and the Kruskal-Wallis H test was used when there were >2 independent samples. In contrast, categorical data were evaluated using the χ2 test and Fisher exact test. The survival rates were assessed using Kaplan-Meier analysis. 15 The log-rank test was used to compare survival probabilities. All tests of significance were assessed bilaterally and a P value of <.05 was considered statistically significant. In the multivariate analysis, the parameters were reviewed with respect to their independent influence on survival, using a Cox regression model.
Results
The patient collective comprised 456 women (70.9%) and 187 men (29.1%). The mean age at the time of surgery was 80.2 years (range: 60-104 years; standard deviation ±7.4). The mean age of female and male patients (80.7 years vs 78.8 years) was not markedly different. All other evaluated variables are summarized in Table 1, including 2 laboratory values at the time of the patient’s admission to the emergency department. Within 2 years, a total of 85 (13.2%) surgical revisions were conducted. The indications for revision are provided in Table 2. A total of 42 patients died within 30 days, 68 patients within 90 days, 117 patients within 1 year, and 165 patients within 2 years after surgery, representing a mortality rate of 6.5%, 10.6%, 18.2%, and 25.7%, respectively. In the univariate analysis, the affected side (P = .593), duration of surgery (P = .175), need for surgical revision (P = .499), implant failure (P = .947), and length of hospitalization (P = .127) did not influence the survival rate.
Indications for Surgical Revisions.
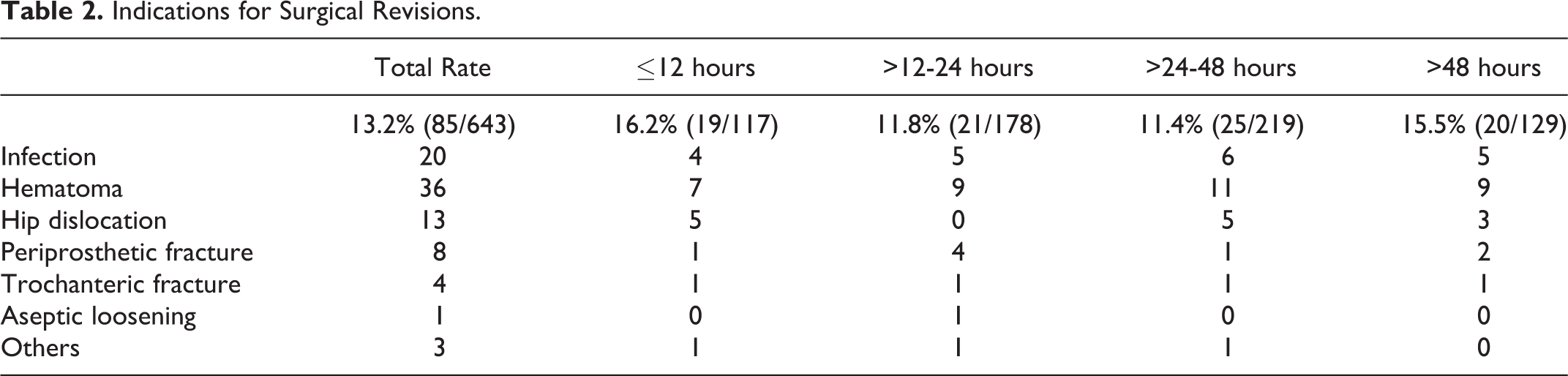
The time to surgery was not a determining factor with regard to survival (Figures 1 and 2), either in univariate (P = .647) or multivariate (P = .213) Cox regression analysis. In fact, patients who underwent surgery >48 hours after admission had the lowest 2-year mortality rate (21.7%); however, the difference was not statistically significant (P = .643).
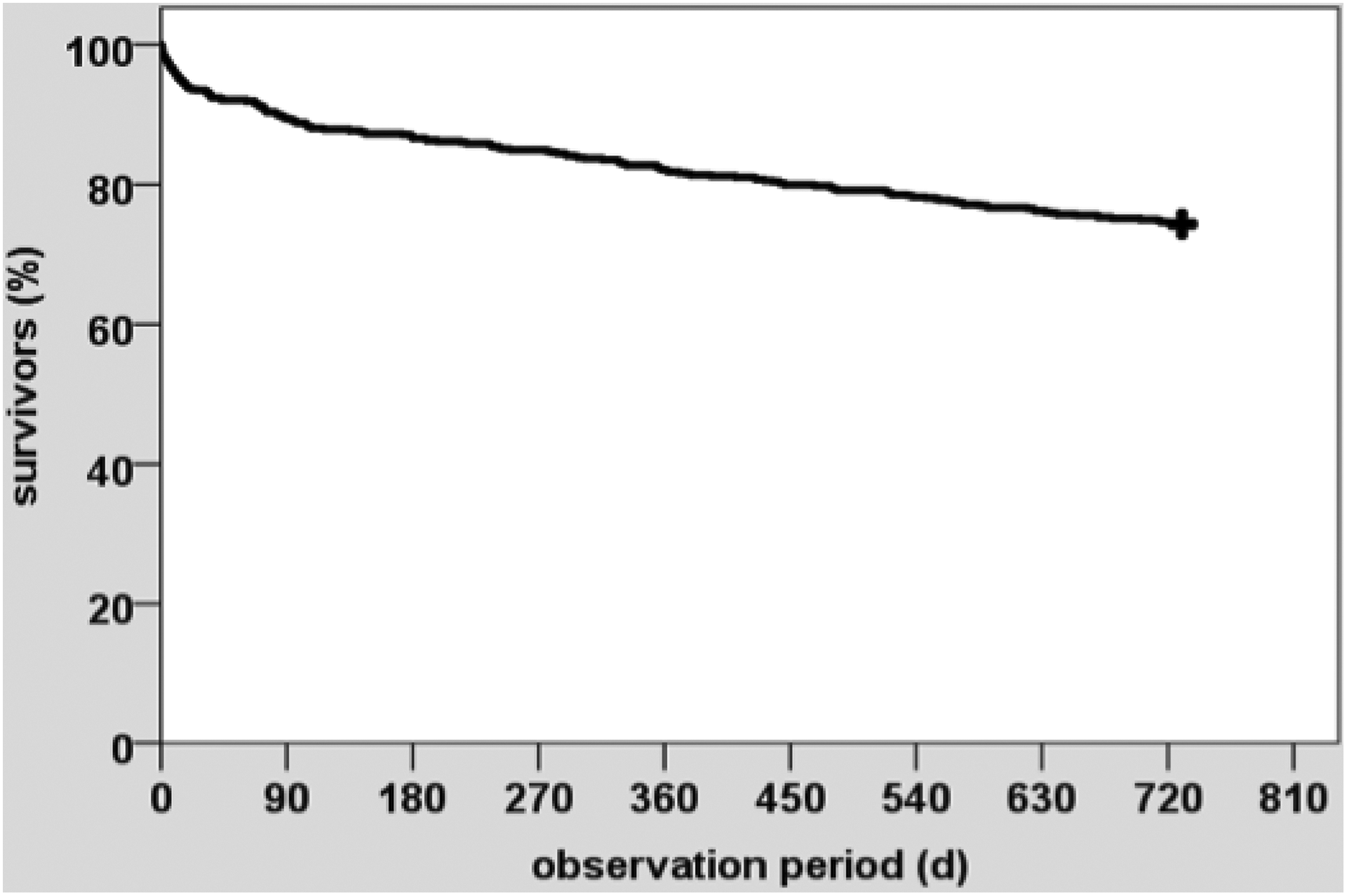
Kaplan-Meier survival analysis estimates for the entire population (N = 643).
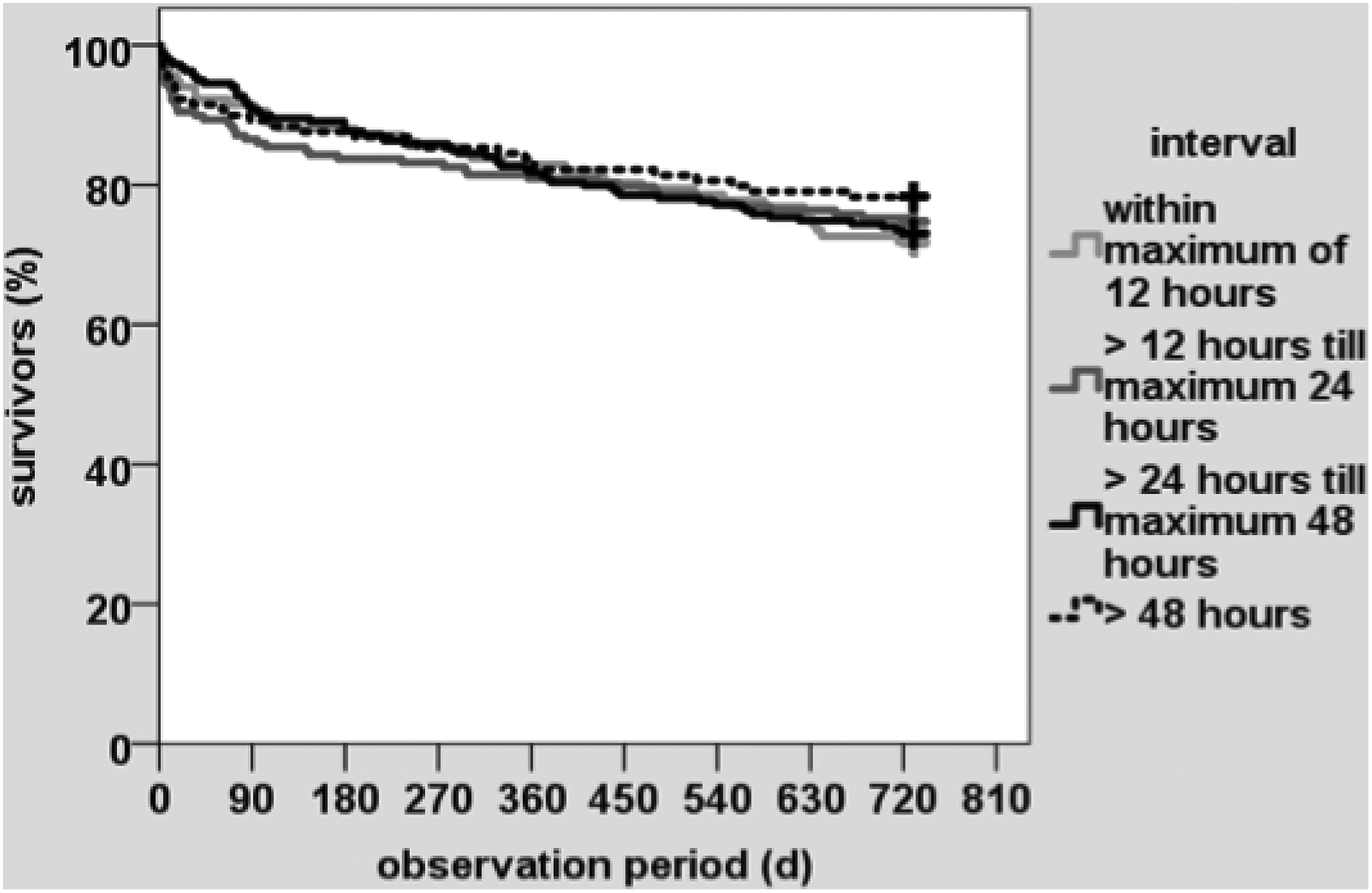
Kaplan-Meier survival analysis estimates with regard to the timing of the patient’s referral for surgery. There are no statistically significant differences.
The Cox regression analysis identified male sex, higher American Society of Anesthesiologists (ASA) score, higher initial C-reactive protein level, lower initial hemoglobin level, and dementia as independent negative risk variables for survival (Table 3). In the univariate analysis, age was also a statistically significant risk factor, although this result was not found in the Cox regression analysis (P = .307). If the surgical delay was >48 hours, the length of hospitalization was significantly longer (P < .000). The reasons for a delay >48 hours are outlined in Table 4, showing that 54 surgeries were delayed for logistical reasons. The 1-year mortality rate of these patients was 16.7%.
Cox Regression Analysis of Factors Associated With Survival.

Abbreviations: CI, confidence interval; CRP, C-reactive protein; ASA, American Society of Anesthesiologists.
Reasons for a Delay in Surgery of >48 hours After Admission.

Discussion
Few clinical studies have assessed outcome measures in relation to time to surgery and total arthroplasty for hip fractures in elderly patients. Our case series with a large number of patients confirmed our hypothesis that surgical timing has no effect on revision for any cause, implant failure, and mortality up to 2 years after surgery.
Our basic data (age and sex) were relatively consistent with the results of other large-scale studies. 16 -19 Furthermore, most of our patients (80%) were referred for surgery within 48 hours of admission. However, fewer than half (45.9%) were referred for surgery within the 24 hours, as proposed in the current guidelines 4 ; however, this ultimately made it possible to allocate a higher number of patients (n > 100) to each of the 4 different time intervals.
The study is characterized by a large number and a homogeneous collective of patients, which included only elderly patients with an intracapsular hip fractures, who were referred exclusively for THA. Moreover, we additionally analyzed objective variables, thus minimizing the risk of data inaccuracy or bias.
In this study, the time from admission to surgery was based on a prospective and exact time documentation for all patients. The accuracy in other studies was compromised because time was expressed in days and not to minutes or hours. In our opinion, this diminishes the scientific power of the results of those studies. 6,7,9,18,20
For example, if a patient was admitted at 11:00
Another example is when a patient was admitted at 1:00
A common feature of multicenter or registry studies is the inclusion of a large number of patients but with the presence of methodical difficulties. 6,7,9,21,22,23 For example, Weller et al enrolled >50 000 patients with hip fractures but failed to specify the fracture types or surgical procedures. 9 McGuire et al included a total of 18 209 patients with different fracture types and different treatment procedures. 7 Moreover, 35% of these patients had missing severity scores (eg, ASA score). Bottle and Aylin were critical of their own data collection, which involved more than 100 000 study patients, explaining that they documented only in-hospital mortality. 6
Most studies analyzed survival rate only up to 30 or 90 days postsurgery, sometimes with conflicting results and conclusions with regard to surgical delay. For instance, the Danish Fracture Database Collaborators 21 showed a significantly higher risk of 30-day mortality with a surgical delay of >12 hours, whereas the risk of 90-day mortality was significantly increased only with a surgical delay of >24 hours. The registry also included a very heterogeneous patient collective, including younger patients (50 years and older), with almost half of the procedures involving trochanteric fractures treated with implants. Moreover, surgical delay was recorded from the time of diagnostic imaging, rather than from the time of admission to the emergency department. As a result, the time interval in this study would be shorter than that in ours. Thus, a comparison with our data is possible only to a limited extent. Finally, the high mortality rate in that study (almost 11% within 30 days and 17% after 90 days) must be emphasized. Our evaluation showed a considerably lower mortality rate (6.5% and 10.6%) with the same-sex and age distribution.
The meta-analyses conducted by Shiga et al and Moja et al likewise concluded that a surgical delay of >48 hours was associated with increased mortality in elderly patients with hip fractures. 24,25 However, most of the included studies only assessed 30-day mortality.
In contrast, our data suggest that delay does not increase the risk of mortality in elderly patients treated with THA for a hip fracture. Therefore, our data agree with the Scottish Hip Fracture Audit, 22 a registry analysis of 18 817 patients with hip fractures, which did not find any influence of surgical delay on the survival rate at up to 120 days postsurgery caused by extrinsic factors such as the surgical timing or other management variables, in contrast to patient-related risk factors (eg, age, sex, ASA score). Moreover, intra- and extracapsular fractures, subtrochanteric fractures, and even some pathological fractures were included in that study.
Furthermore, a systematic review by Khan et al involving 25 studies with nearly 280 000 patients also concluded that surgical delay may not affect survival. 26 Lastly, a current data registry and 1 multicenter study with a large number of patients also failed to document any significant effect on the survival rate. 19,27
Our analysis revealed that 5 patient-related risk factors significantly influenced survival and that these factors could not be changed. On the other hand, all 3 modifiable factors—shorter duration of surgery, prevention of the need for revision, and a faster referral to surgery (the main question of this study)—had no significant effect. These results have previously been demonstrated by different authors in a similar form. 18,28,29 For example, Hu et al identified 12 different variables during their meta-analysis of proximal femoral fractures. 29
Most studies did not provide any explanation about why surgical delay occurred. 18,20,21 Our detailed investigation of delayed surgery (>48 hours) failed to detect any patient-related reason in nearly half of the patients. Therefore, delay was only for logistical reasons, for example, a lack of operating room availability. Surprisingly, the mortality rate of these patients was not adversely affected. Moreover, our analysis revealed that a surgical delay of >48 hours was significantly associated with prolonged hospitalization (>2 days). This result is self-explanatory and in line with several other studies. 18,30,31 Therefore, it is simple to understand why insurance providers are demanding that surgery occurs without delay—to reduce the costs of extended hospitalization.
Our study also assessed all revisions carried out in the 2-year period after THA, including also any surgical revision for the treatment of hematomas. A rate of 5.6% (36/643) seems to be high, but the authors detected no objective reasons for that. There was no significant correlation between time to surgery and either implant failure or revision surgery. To date, neither of these complications, which both contribute to morbidity, have been scientifically investigated in the context of surgical delay.
Finally, the limitations of this study should be disclosed. As this was a retrospective, consecutive case series, the level of evidence is low. Despite the large number of patients in our study, the collectives were reduced because patients were divided into 4 groups; however, each group still comprised at least 100 patients. Within the study period, the treatment of choice was THA and not the frequently recommend hemiarthroplasty. The study design did not involve further radiological or clinical follow-up examination, as this would have been difficult or impossible in multimorbid patients who often have dementia. As a result, other possible complications such as chronic hip dislocation or aseptic loosening were not documented. Despite the high mortality rate, the 2-year endpoint of our study makes it a short- to medium-term evaluation.
Conclusions
In this single-center study, time to surgery did not significantly influence revision for any cause, implant failure, or mortality in patients undergoing THA for an intracapsular hip fracture. Therefore, it is not absolutely necessary to perform this surgery within 24 or 48 hours of admission. The main reasons for avoiding surgical delay are ethical and economical in nature, such as to minimize costs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.