
Abstract
Introduction
There is lack of consensus regarding best operative fixation strategy for periprosthetic femoral fractures (PFFs) around a stable stem. Evidence exists that some patterns of fracture around a stable stem are better treated with revision surgery than with standard fixation. Anyway, a more aggressive surgical procedure together with medical treatment could allow for stem retention, and reduced risk of nonunion/hardware failure, even in these cases.
Significance
This paper is placed in a broader context of lack of studies on the matter, and its aim is to shed some light on the management of PFFs around a stable stem, when peculiar mechanical and biological aspects are present.
Results
Based on our casuistry in the treatment of nonunions after PFF successfully treated with original stem retention, and on review of Literature about risk factors for fixation failure, an algorithm is proposed that can guide in choosing the ideal surgical technique even for first-time PFFs with a stable stem, without resorting to revision. Mechanical (major and minor) and biological (local and systemic) factors that may influence fracture healing, leading to nonunion and hardware failure, and subsequent need for re-operation, are considered. The proposed surgical technique consists of rigid fixation with absolute stability (using a plate and structural allograft) plus local biological support (structural allograft and autologous bone marrow concentrate over a platelet-rich plasma-based scaffold) at fracture site. Systemic anabolic treatment (Teriparatide) is also administered in the post-operative period.
Conclusion
Mechanical factors are not the only issues to be considered when choosing the surgical approach to PFFs over a stable stem. Systemic and local biological conditions should be taken into account, as well. A therapeutic algorithm is proposed, given the prosthetic stem to be stable, considering mechanical and biological criteria.
Keywords
Introduction
Prolonged life expectancy and the ever-expanding indications for total hip arthroplasty (THA) are leading to an increasing number of implants being placed in both young and elderly patients with high functional demands. Consequently, this increase in THAs annually performed is associated to a global raise of complications, including periprosthetic femoral fractures (PFFs) whose incidence ranges between 0.7% and 11% over a primary and between 1.2% and 18% over a revised hip stem.1-6
Modified Vancouver Classification of PFFs.

This fracture was first described as a pseudo-AL or new-B2, with a loose stem, by Van Houwelingen and Duncan in 2011; later on, Capello et al described it as clamshell type, being the stem stable (A1) or loose (A2); clamshell (and reverse clamshell, as well) PFFs with a stable stem are included in type B1 PFFs.
Treatment Indications for PFFs According to Modified Vancouver Classification.
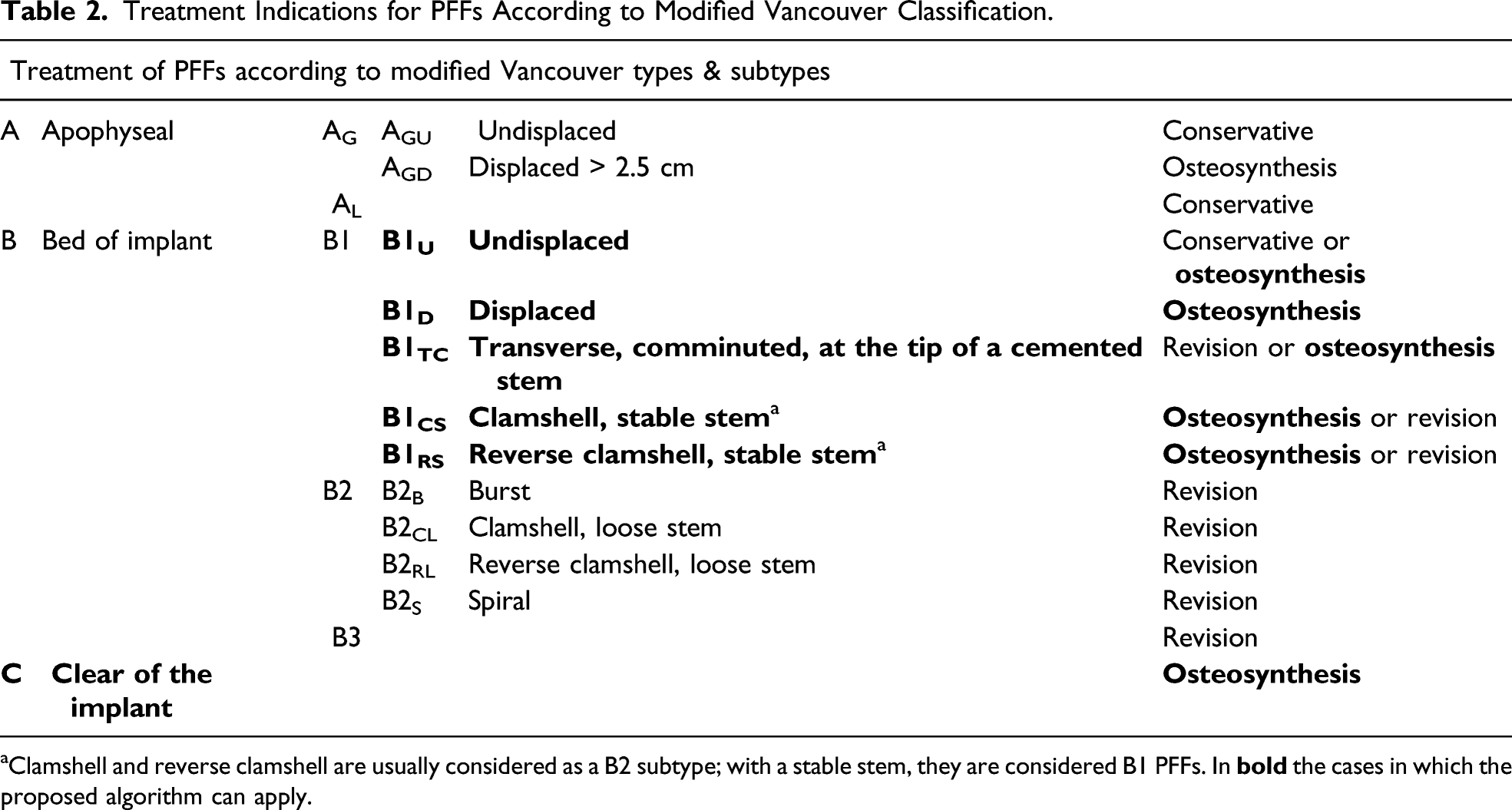
Clamshell and reverse clamshell are usually considered as a B2 subtype; with a stable stem, they are considered B1 PFFs. In
To date, most of the studies have produced therapeutic algorithms that focus on implant stability, leaving the choice of treatment to the habit of the surgeon, not defining the best surgical strategy. Both minimally invasive plate osteosynthesis (MIPO) obtaining an elastic fixation or open reduction and internal fixation (ORIF) with plate and cerclage with or without a structural allograft (or a second plate) have been advocated, based on mechanical issues.8,25,26,28,44-49 Revision arthroplasty has been proposed as a valid option in some B1 PFFs, again mainly based on mechanical issues.30,45,50-58 Anyway, the biological aspect of the patient has been neglected, considering it as not fundamental for the type of PFF and the surgical approach. Instead, patients with prostheses can present biological systemic and local issues that commonly include multiple medical comorbidities and long-lasting medical therapies such as glucocorticoids (GSs), and difficulties with post-operative rehabilitation. 59 Also, the PFF can happen over a bone of very poor quality and/or present a pattern such that mechanical issues are not the only local factors to consider to be deficient.
Moreover, studies are present in the Literature suggesting that the antiosteoporotic agent Teriparatide can be useful in fractures’ and nonunions’ management, as well.60-68 This drug works by stimulating osteoblasts and reducing osteoblast apoptosis, increasing callus formation, improving mechanical strength, and resulting in increased osteoblast life span. To date, the administration of Teriparatide is reserved for severe osteoporosis (T-score -2.5 or less plus at least one fragility fracture), but it is also prescribed to promote fracture healing, especially in atypical femoral fractures (AFFs) occurring in patients treated with bisphosphonates (BPs) for a long period.69,70
The aim of this paper is to propose an algorithm of treatment of PFFs over a stable stem (Vancouver B1 and C types), considering both mechanical and biological (local and systemic) criteria that can guide the surgeon in choosing the ideal approach, based on results in the Literature and starting from our own results in the treatment of nonunions/hardware failure on PFFs. At our Institutions, no Institutional Review Board nor Ethical Committee Approval is necessary for retrospective studies and reviews of Literature. Patients gave their consent to data collection and anonymous use of them for scientific and teaching purposes.
Methods
Suggested “short” phosphocalcic metabolic panel, including only blood testing without any precise preparation nor a 24-hour urine collection. ALP: alkaline phosphatase, Ca: calcium, P: phosphorus, PTH: Parathyroid hormone, CTX: C‐telopeptide of type I collagen, P1NP: aminoterminal pro-peptide of type I procollagen, 25(OH)D: cholecalciferol (vitamin D3).


Histological finding of giant osteoblasts (arrows), consistent with an AFF, were found in a type C PFFs.
Patients’ Medical History and Management of Their Fractures.

A systematic literature review of studies reporting on risk factors for nonunion and hardware failure in PFFs treated by fixation was performed according to Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines, as well. Two researchers independently searched the Scholar and MEDLINE databases to identify articles published until April 2021, limited to English language. The terms used were as follows: (failure) AND (periprosthetic femoral fracture). Reference lists of related papers were manually searched to identify potential eligible studies.
Based on findings in our clinical series and on Literature review, a list of biological local and systemic criteria to be take into consideration as risk factors for nonunion and hardware failure in PFFs treated by fixation was set up, together with already known mechanical criteria. All cases were reviewed and evaluated in the light of these proposed criteria. Biological bone healing capability was impaired in all our cases: each patient was administered long lasting BPs or GCs therapy. As regards the surgical technique, we noticed that in one case the femoral stem entirely occupied the canal and did not allow for screw fixation but cerclages only. In this scenario, the construct could have been characterized by rotational instability that led to fixation failure, and the addition of strut grafts may have improved stability and therefore outcomes. Based on the reassessment of our case series, an algorithm has been hypothesized, considering mechanical AND biological criteria, to guide the surgeon in the therapeutic choice, given the prosthetic stem to be stable (Vancouver type B1 and C) and willing to retain it.
A correct assessment of the fracture type according to the Vancouver classification is of paramount importance. Plain radiographs alone may not be sufficient to establish a precise diagnosis, so that CT scans with metal suppression or 3D reconstruction may be able to provide additional information regarding fracture characteristics such as the medial extension of the fracture gap or the presence of comminution. However, a precise and accurate review of the patients’ medical history is also just as important.
We therefore thought to create a therapeutic algorithm and started to treat patients presenting with first-time PFF according to it.
Criteria and Proposed Algorithm

Resorption, wedge fracture, or comminution.
Osteoporosis, rheumatic and/or autoimmune diseases, primary or secondary endocrinological diseases, osteomalacia, Paget’s disease, ..

A fluted tapered uncemented long revision stem is occupying the entire canal in an osteoporotic patient. In such a case, there is any place not even for monocortical screws; only one bicortical screw could be used, but it would be too much close to the fracture line, therefore not guaranteeing any rotational stability to the fixation.

Comminution of fracture (over a well-fixed Zweymueller-type stem, not visible in radiographs) is a minor mechanical criterion, but it can hide impaired biology. The patient was on chronic GSs therapy for myasthenia gravis and presented secondary hypoparathyroidism, too, both due to a thymoma.
Biological local criteria are: 1) a fracture around a cemented stem, 2) estimated wide surgical dissection or a previous open access at the affected site, or 3) an atypical pattern of the fracture; systemic criteria are: 4) diseases affecting phosphocalcic metabolism (osteoporosis, rheumatic and/or autoimmune diseases, primary or secondary endocrinological diseases, osteomalacia, Paget’s disease, ..), 5) long lasting pharmacological therapies with GSs or BPs, 6) heavy smoking (≥ one pack/day). Some of these biological criteria can link each other (for example: an atypical pattern of fracture seems more frequent in osteoporotic patients on long lasting BPs therapy) and can coexist. As for cemented stems, in our opinion, it is more a biological issue than a mechanical one: an overlooked failure of the stem-cemented interface has been advocate as a mechanical cause of failure in PFFs around a cemented stem,29,72 but a reduce capability of bone healing (less viable area, no endosteal callus formation) and an absent opportunity for re-osseointegration are biological issues that are undoubtedly present. Alike, a transverse fracture at the tip of the stem has always been considered a mechanical problem but it also implies biological issues (less surface for bone healing).
Based on these criteria, an algorithm is proposed (Figure 4). If no criterion or just one minor mechanical criterion is present, a MIPO or ORIF technique achieving relative or absolute stability without adding any biological support can be indicated. If one major mechanical criterion is present, an ORIF technique with the addition of a medial cortical structural allograft, achieving absolute stability of the construct with some osteoconductive support is preferred. If one biological criterion is present, absolute stability plus osteoconductive support (ORIF with one medial or anterior structural graft) or relative stability plus anabolic support (MIPO and post-operative Teriparatide) are aimed to. If two or more criteria are present (no matter if mechanical ones are major or minor), an aggressive surgical approach is indicated: ORIF with double structural allograft plus osteoinductive/osteogenic support with apposition of autologous bone marrow cells concentrate (BMC) and platelet-rich plasma (PRP) at the site of the fracture. The proposed therapeutic algorithm for PFFs over a stable stem (Vancouver type B1 and C). In case of two or more criteria, no matter if mechanical ones are major or minor.
Post-operative systemic anabolic pharmacological therapy with Teriparatide can be added in all cases. Anyway, being this use of Teriparatide an off-label application, we reserve it to patients with one biological criterion or with two or more criteria (or in cases of delayed union).
Proposed Surgical Technique (2 or More Criteria Present)
Surgery (whose expected duration is around 2 hours) is usually conducted under general anesthesia. Our preferred position is the lateral contralateral decubitus that allows to extend the surgical access as a posterolateral approach to the hip in case proximal extension is required. Standard antibiotic prophilaxis is admistered (usually Cefazolin 2 g 30 minutes before surgery). Antithrombotic prophilaxis is started at trauma with low-molecular weight heparin and continued until complete weight-bearing is possible. Whole blood sample from peripheral vein and percutaneous bone marrow blood samples from the ipsilateral iliac crest are collected and PRP and BMC are prepared in accordance with the recommendations of the manufacturer (Regen Lab SA, Le Mont-sur-Lousanne, CH). The massive fresh-frozen allograft is prepared on a side table by an assistant while surgery is performed. The diaphyseal allograft can be cut in halves or thirds or more tangentially then from the center, depending on dimension of both the host femur and the allograft itself. At the end of surgery, local tranexamic acid is used to reduce bleeding in the manner previously described elsewhere. 73
We aim to obtain a rigid construct (absolute stability) with biological (osteoconductive, osteoinductive, and osteogenic) support. Our preferred hardware is a low contact lateral plate with polyaxial angular stability screws and cerclages (NCB system, ZimmerBiomet, Warsaw, IN, USA) or a hook trochanteric plate with screws and cerclages (Cable-Ready Extended GTR Plate, ZimmerBiomet, Warsaw, IN, USA) in case a more proximal PFFs occurs, even if the latter plate does not guarantee for angular stability and requires bone-plate contact.
A double structural allograft (medially and anteriorly placed, at 90° each other) is also used. A diaphyseal fresh-frozen allograft is obtained through our Regional Bone Bank; a fresh-frozen graft is preferred to a freeze-dried one as mechanical properties are more preserved. Also, a femoral diaphysis is preferred, for size and shape, but sometimes a tibial or a humeral one is available. In our setting, they come as an entire diaphysis, so it is possible to obtain more sticks from one graft. We aim to bridge the fracture by at least 2 diaphyseal diameters per side: a minimum length of 10 cm is then required for transverse fracture, while longer struts are suggested for different fracture patterns. For the anteriorly placed strut graft, a flat stick is prepared to allow for some flexion and better fit to the anteriorly bowed host diaphysis. The ends are chamfered to reduce encumbrance and to look for a smooth transition both for the medial and the anterior strut. The medial strut will take up space against the vessels, while the anterior one will stuff the extensor apparatus. Moreover, a bevel end seems to guarantee a gradual transition of forces. 74 The fracture is debrided and reduced with forceps and/os cerclages; the struts are positioned together with the lateral plate. Then cables and/or screws are used to secure the struts to the host bone and to the plate. The medial strut is secured with as much screws as indicated (tricortical screws) and cables through the plate, while the anterior one through cables to the plate and possibly with 2 screws to the host bone. The structural grafts will carry mechanical and osteoconductive support.
At the same time, autologous bone marrow aspirate is obtained from the same or contralateral iliac crest, and autologous peripheral blood is drawn in a sterile way. They are both centrifugated in the operating theater to BMC and PRP. The PRP is further prepared with fibrin to obtain a PRP-based membrane (Regenkit BMC and Regenkit Extracell Membrane glue, RegenLab). The BMC is embedded into the PRP-based scaffold, which will be placed at fracture site and between graft and host bone at the end of fixation, before wound closure (Figure 5). This will bring osteoinductive and osteogenic support. The PRP-based scaffold embedded with BMC is placed at fracture site and between graft and host bone before wound closure.
In the post-operative period, patients are also pharmacologically treated with Teriparatide (Forsteo, Eli Lilly and Company, Indianapolis, IN, USA) for at least three months. Teriparatide is prescribed off-label after adequate informed consent is acquired and under guidance of the Bone Metabolic Unit. This will bring an anabolic support for bone healing (Figure 6). The final construct of case in Figure 3 (
Discussion
Limitations of the proposed algorithm are present. First, the small cohort of patients from whom the idea came out is not the index indication we would like to apply the algorithm to, and it was a small series. The proposed combined aggressive surgical and medical approach was applied to a particular group of patients presenting nonunion/fixation failure of a PFF that were treated successfully with repeated osteosynthesis and stem retention. Anyway, the retrospective evaluation of risk factors showed that all failures were related to the presence of both mechanical and biological issues. Also, revision arthroplasty for failed osteosyntheses can guarantee good results,75,76 and it could be a valid surgical alternative. However, we based our proposal of such a therapeutic algorithm to reduce failures in PFFs’ treatment not only on the analyses of our series but also on the review of Literature.25,28,34,46,77
Fractures with a stable stem (Vancouver B1 and C) are commonly treated by ORIF or by MIPO. The variety of methods and implants used, and their combinations implies that no “gold standard” exists. Elastic fixation (relative stability) with minimal soft-tissue damage seems to be preferred,43,44,78,79 relying on biological potentiality of the fracture, while a rigid fixation (absolute stability) is advocate in some other cases.7,45,80 ORIF can be enhanced with a structural allograft or with a second plate. 81 Anyway, authors have focused their attention over mechanical issues of the PFF,51,82,83 without taking into account patient’s biological criteria.
As for mechanical criteria, these are already well known. Characteristics of the fracture and type of hardware have been evaluated, with biomechanical studies51,81,84-90 confirming clinical remarks.51,81,84-90 The use of bicortical screws around the stem is preferable over cerclages alone or cerclages plus monocortical screws, even if a recent clinical study showed no differences in results when only proximal cables where used with a non-locking plate. 91 Also, it can be advisable to span the whole femur with the plate. 92 However, there are fracture’s patterns, such as the comminution/resorption of the medial cortex, the presence of a transverse or short oblique fracture at the tip of the stem, the comminution or poorness of bone-stock at fracture site, in which an adequate torsional/sagittal and bending stiffness cannot be guarantee by a lateral plate alone. In these cases, a second mechanical support appears useful. A structural allograft is recommended medially while anteriorly both a structural allograft or a second plate can be used,28,77,83,93,94 sounding better a medial than an anterior reinforcement. 86 A structural allograft is in our opinion better than a second plate as it can bring osteoconductive support as well, especially if a pharmacological anabolic treatment is performed.
Mechanical elements are not the only factors that should indicate the use of a structural allograft, and biological issues must be considered, as well. A PFF around or at the tip of a cemented stem,21,72,95 or over an osteoporotic bone are known to have higher complication rate than other cases. 96 Conditions such as osteoporosis and rheumatoid arthritis or other autoimmune or endocrinological diseases, long lasting GCs or BPs assumption, AFFs or previous surgeries are indicators of a local and systemic biological impairment that suggest the use of structural allograft even if mechanically it would be unnecessary.7,10,31,97 Also, smoking is known to be a negative prognostic factor for bone healing, and it has been found in a systematic review as the only biological patient-depending risk factor for nonunion. 98
As for fracture’s healing, it is well known that an adequate environment includes mechanical stability and biological osteoconductive, osteoinductive, and osteogenic support.99-101 Also, metabolic pharmacological therapy with Teriparatide showed promising results when mechanical issues are present.24,64-66
Our initial experience on re-fractures,65,67,71,102 the one with AFFs when intramedullary nailing is not possible (over a deformed bone or in “periprosthetic” AFFs) 64 and with proximal femur fractures in the elderly (in whom an osteometabolic study should always be done, and eventually proposed an antiosteoporotic pharmacological treatment together to the Bone metabolism Unit) and the review of Literature,60,103-105 lead us to proposed such a surgical aggressive and combined pharmacological treatment even to some first-time PPFs. We therefore started to apply the proposed algorithm to first-time PFFs. To now, we have treated 7 PFFs with the described approach (rigid fixation + biological local support and systemic anabolic therapy), all of them presenting clinical and radiological signs of bone healing at 3 months.
In PFFs with a stable stem that may fail to heal because of mechanical or biological issues, we propose a combined mechanical-biological approach that consists in a rigid fixation (absolute stability) with a lateral plate and structural allograft (better if possible, a double structural allograft, at 90° each other, medially and anteriorly) with apposition of autologous BMC and PRP at the fracture site plus medical therapy with Teriparatide in the post-operative period. In our experience it appeared evident that patients who already failed in previous fixation are likely to achieve a complete healing without further complications.
Only cortical structural allograft is a known option for the treatment of PFFs around a stable femoral stem as adjunctive fixation when a plate is used. 106 A structural allograft has both mechanical and biological properties: it confers stability to fracture site, allows a longer working length of the screws if put medially, it has osteconductive properties, and it can incorporate and ultimately increase the femoral bone-stock. 107 On the other hand, extensive soft-tissue dissection and longer operating time for allograft application result in decreased periosteal blood supply to the fracture site and this can be a reason for a longer time-to-heal (even to nonunion) and a higher infection rate.45,79,108 If we have only one structural allograft, we use to put it medially; anyway, it also depends on femoral bowing, level of fracture and length of the stem with revision stems more likely to need an anteriorly placed allograft as straight stem can head to the anterior cortex and stresses are to be counter on the sagittal plane as well. Anyway, in our hospital setting, fresh-frozen structural allograft are entire diaphyses and not emidiaphyseal, so we usually can prepare and use a double structural allograft.
To reduce such a risk of delayed union or nonunion related to extensive dissection, we look for osteoinductive ed osteogenic properties, as well.62,99-101 BMC is derived from autologous bone marrow, and it is composed of a variety of cells, including mesenchymal stem cells that can contribute to the regeneration of mesenchymal tissues, capable of self-renewal and differentiation into various cell types such as bone, muscle, tendon, and ligament. These properties have a positive influence on bone formation, neoangiogenesis, and fracture healing.64,102 Also, a PRP-based membrane as a scaffold for BMC has already shown enhanced osteogenic and angiogenic properties. 109
Lastly, systemic anabolic support can be of help especially in biologically impaired patients. PTH is a single-chain 84-aminoacid secreted polypeptide that plays a critical role among the calcium regulating hormones. Although hyperparathyroidism is associated with bone loss, intermittent administration of PTH or its N-terminal 1-34 fragment (Teriparatide) is known to increase bone mass, as anabolic properties of PTH dominate over its catabolic effects. Also, PTH acts upregulating the marker genes associated with osteoblast differentiation. Physiological PTH actions include stimulation of osteogenesis by direct effects on cells responsible of bone formation (osteoblasts) and indirectly by increasing intestinal absorption of calcium and increasing the renal tubular reabsorption of calcium and elimination of phosphate. Evidence is present in the Literature that Teriparatide can be useful in the treatment of nonunions, delayed unions and AFFs.60-66 Also, in an animal model a combined administration of subcutaneous Teriparatide and systemic human mesenchymal stem cells showed a synergic positive effect on bone healing. 110
We therefore are proposing such an anabolic medical treatment, together with the Bone Metabolic Unit, in foreseeable difficult cases or when surgical dissection is wide and devascularization is likely.
For those reasons, in our opinion, in selected cases, it is worthwhile a more aggressive and multimodal approach to avoid re-fractures in PFFs. A more invasive surgery (rigid fixation and absolute stability of the fracture) with local biological support and systemic anabolic medical therapy are key to fracture healing. The intent of our proposal is to shift attention toward biological parameters to better frame the patient and avoid failures. More studies and even multicentric evaluation can be useful to validate or to reject this algorithm, and to evaluate eventual increase in other complications such as infections.
Conclusions
Nonunions, re-fractures, and hardware failures can happen after treatment of PFFs. The choice of a correct surgical strategy is essential to reduce complications and ensure complete healing. In our experience, MIPO does not always completely meet biological or mechanical criteria such as to make treatment with locking plate alone sufficient to grant fracture healing. On the other hand, ORIF especially if associated to structural allograft can jeopardize local vascularization due to the extensive exposure needed. The proposed therapeutic algorithm is designed to have a more complete vision of the patient, and to give a more satisfactory surgical approach to these fractures. This combined biological and mechanical approach has been proven successful in re-fractures over PFFs cases and other impaired cases (such as AFFs).
In our opinion, the implementation of such a comprehensive approach even at first-time PFFs can increase healing rates and reduce failures. Application of this algorithm in type B1 and C PFFs is ongoing at our Institution, to assess its feasibility and safety, as first evaluation point. More cases, case-control matched studies, and multicentric evaluations are needed to confirm, or reject, the hypothesis of the algorithm.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.