
Abstract
Objective:
To evaluate the efficacy of the use of retentive cup primary total hip replacement (THR) in high-dislocation risk subcapital fracture patients.
Methods:
During the years 2008 to 2012, 354 patients with displaced subcapital fracture were operated at our institute. The patients were selected to undergo primary constrained THR according to the following criteria: (1) a preinjury grade 4 or more on the Functional Independence Measure mobility item “5. Locomotion: walking/wheelchair” and grade 4 is defined as “4. Minimal assistance Requiring incidental hands-on help only” (patient performs >75% of the task) and (2) a disease leading to poor motor control. Exclusion criteria were normal muscular control and known infection of the involved joint.
Results:
Of the 354 patients, 87 fulfilled the inclusion criteria and underwent constrained total hip. Average age was 78 years with a female predominance (73%). Fifteen patients had prior hemiparesis, 19 had Parkinson disease, and 35 had generalized sarcopenia. Eighty-five patients had an uneventful recovery, with an average Hip Disability and Osteoarthritis Outcome Score (HOOS) of 76 ± 7 at 2 years. In 2 patients, the prostheses dislocated. In both cases, the dislocation was due to ring displacement and the inner head dislocated. One case was infected and the patient was treated by a Girdlestone procedure. In the other case, the prosthetic head was revised. The patient remained asymptomatic and at 4-year follow-up had an HOOS of 85.
Discussion:
It appears that constrained prosthesis is a suitable treatment for patients with poor muscular control having subcapital fractures. The functional results appear to be superior to those of bipolar arthroplasty and similar to the results of primary total hip arthroplasty while the dislocation risk is <3%.
Conclusion:
Semielective total hip arthroplasty using a retentive cup liner appears to offer good functional results with a low dislocation rate in patients with poor muscular control.
Keywords
Introduction
In the last decade, the pendulum has shifted toward total hip replacement (THR) regarding the optimal treatment of subcapital fracture. 1 The THR has proven to be superior to hemiarthroplasty and internal fixation for functional rehabilitation and health-related quality of life. 2 However, the main concern with this treatment, namely instability or dislocation, is yet to be solved. The drawback of primary THR in this patient population, in contrast to the chronic osteoarthritis population, is a high dislocation rate of up to 20%. 3 Certain innovative designs, such as the retentive cup and large-diameter heads, 4 may reduce the incidence of dislocation.
Patients with neurological conditions have a higher risk for dislocation, due to associated paresis, spasticity, contractures, and tremors, potentially leading to poor muscle tone across the hip. Abnormal muscle tone predisposes arthroplasty patients to early failure resulting in dislocation. 2
A possible solution for patients with muscle abnormalities across the joint is the use of a constrained prosthesis. 5,6 This study 6 was performed using the Biomet Freedom liner, (Zimmer-Biomet Ltd., Warsaw, IN, USA) which is 36 mm in diameter. Of 81 patients, 9 were primary procedures mostly performed due to neurological injury or dementia. The overall success rate in dislocation prevention was 98.8%. 6 Unfortunately, the antidislocation ring renders the lever arm at the acetabular component much longer; although the force to dislocation in bench tests is high, impingement on the femoral component neck occurs at 110°. This might lead to loosening of the acetabular component with an odds ratio of 3.3. 7
The current series describes consecutive patients followed prospectively with subcapital fractures that were treated using a constrained total hip arthroplasty from 2008 to 2012.
The working hypothesis had been that the rate of dislocation in this high-risk patient group could be reduced using a retentive cup design, while the loosening rate will not be high, due to the limited muscle function and loading.
Methods
This is the report of a patient cohort operated at a single institution, and data were prospectively collected as part of routine clinical practice. The patient status was evaluated according to the Functional Independence Measure (FIM) score (UK modification
8
). During the years 2008 to 2012, 354 patients with displaced subcapital fracture were operated at our institute. The patients were selected to undergo primary constrained THR according to the following criteria: A preinjury grade 4 or more on the FIM mobility subscale item 5 is defined as “5. Locomotion: walking/wheelchair.” Grade 4 is described as Minimal assistance Requiring incidental hands-on help only (participant performs >75% of the task
8
; Table 1). A disease leading to poor motor control (decided after history taking and physical examination by a trained rehabilitation physiotherapist). Limited ability to cooperate with a rehabilitation protocol.
Clinical Details of Patients.

Abbreviation: BMI, body mass index.
Exclusion criteria were normal muscular control and known infection of the involved joint preventing replacement arthroplasty.
All patients were annually monitored at the outpatient clinic, with the average follow-up period being 5.0 years (range, 3-7 years). Preoperative evaluation included obtaining a plain radiograph of the pelvis, as well as anteroposterior views of the involved hip.
Patients’ demographic and clinical data were collected before surgery, including age, sex, body mass index, medical history, hemoglobin levels, diagnosis necessitating surgery, and muscle strength of the affected limbs before the fracture.
Functional assessment was carried out according to the preinjury ambulatory status, and a repeat assessment was performed 1 year after the implantation. Questionnaires were filled out by the patients or on behalf of the patients by their caretaker. Radiographs were available for all patients at 6 to 12 months postsurgery and annually thereafter.
Operative Procedure
All patients were operated by either A. G. or M. Y. using the anterolateral approach with the patient in the lateral position.
All patients were given broad-spectrum antibiotics at least 1 hour prior to surgery and for 24 hours thereafter. All patients received prophylactic anticoagulants via once-daily administration of 40 mg enoxaparin. Patients who were treated prior to injury with anticoagulants were treated with 80 mg enoxaparin for 24 hours, and later, their prior treatment was reinstated.
Constrained total hip was performed via an anterolateral approach with the patient placed side-lying. Operative times averaged 75 ± 8 minutes. The femoral component used was the CORAIL Hip System (DePuy Synthes, Warsaw, Indiana; n = 85) or a cemented stem (C-STEM; DePuy Synthes; n = 2). The retentive cup used was TREGOR MEDIAL CUP (Aston Medical Orthopaedic Implants, Saint-Étienne, France) consisting of an unconstrained cemented metallic cup, articulating with a dual mobility polyethylene (PE) insert, which is clipped on the stem head. Essentially, 2 joints are thus formed, a major one between the metal cup and the outer polymer surface and a lesser one between the inner polymer surface and the hip stem component. The cemented cup is made of stainless steel, and its innovative design feature lies in its nonuniform thickness (from an average of 5-6 mm along the equator to 1.7 mm average at the pole) resulting in the medialization of the center of rotation, known to increase stability. This effect is further enhanced by the mobility of the insert with extreme movement protected by a cylindrical extension of the inner surface of the cup. A peripheral rim and bidirectional grooves ensure pressurization of the cement and the stability of the implant in the cement under load, respectively. The inner surface of the cup is solid (no holes) and polished in order to best protect the mobile PE from wear and creep (http://www.aston-medical.com/EN/medias/pdf/tregor/DOC2580_DocMedialCup_EN_saufUSA.pdf). The PE liner has also an unusual design feature—as it is able to move within the cup, providing a significant increase in the range of motion without dislocation by taking over the movement of the head while in an extreme position. It is retentive on the femoral head due to its internal volume far exceeding the size of an hemisphere (Figure 1). The acetabular component could be connected to a femoral component that has a polished neck without asperities and a head design that covers the entire Morse taper to avoid premature polymer wear when the neck is in contact with the edge of the insert during maximum amplitude of the lesser joint.

A, The center of rotation of a normal hip joint can be approximated to the point termed original center of rotation (OCR). B, Due to its specific architectural design, the implant has a medialized center of rotation defined as implant center of rotation (ICR). C, The acetabular component has a cemented shell with a smooth internal surface in which a polyethylene component is inserted. The construct is locked on a prosthetic head that coverts entirely the neck morse taper. D, X-ray demonstrates the prosthesis in situ (both components were cemented).
Anesthetic regimen had to be adapted for the specific patient disease. For patients with Parkinson disease, we used general anesthesia to control the muscular rigidity and tremor. After hip exposure, the operation could be finished successfully with the routine surgical steps.
Blood replacement trigger was defined as hemoglobin of <9 mg/dL. Complete blood counts were taken every day for the first 72 hours after surgery.
Rehabilitation Regimen
Patients were guided to do bed exercises, such as quadriceps femoris isometric contraction, immediately after the operation and try to get out of bed with the help of a crutch or walker from the first postoperative day to 1 week postoperatively. Weight bearing was not restricted.
Patients were transferred to a rehabilitation hospital from 5 to 10 days after surgery. The average hospital stay was 5 ± 2 days. Clinical and radiologic assessment was done before surgery, at 3 months, 6 months, and 1 year after surgery, and then annually. Clinical assessment of pain, function, deformities, and range of motion was based on the evaluation system developed by Harris (8) that assesses all of these parameters and allows scoring of the disability grade. A Harris hip score of ≤70 points was considered as a poor outcome, 70 to 79 points as fair outcome, 80 to 89 points as good, and ≥90 points was considered as an excellent outcome. Radiologic assessment included a standing anteroposterior radiograph of the pelvis with the radiograph centered at the pubic symphysis and a lateral radiograph of the operated hip joint.
Results
Of the 354 patients, 87 fulfilled the inclusion criteria (Table 1). Average age was 78 ± 10 years with a female predominance (73%). Fifteen patients had prior hemiparesis, 19 patients had Parkinson disease, 35 patients had generalized sarcopenia, 4 patients had prior poliomyelitis affecting the gluteal musculature, 2 patients had myasthenia gravis, 2 patients had amyotrophic lateral sclerosis, 1 patient had prior lumbar surgery and gluteus paralysis (15 lesion), and the rest had relatively mild dementia.
Eighty-five patients had an uneventful recovery, with an average Hip Disability and Osteoarthritis Outcome Score (HOOS) of 76 ± 7 at 2 years (Table 2). No patients were lost to follow-up. Eighty-seven patients were available for the 24-month follow-up, though the numbers declined later (see Table 2). Of the 87 patients, 84 reported significant pain relief at 24 months.
Patient HOOS and Survival.

Abbreviation: HOOS, Hip Disability and Osteoarthritis Outcome Score.
At the final available follow-up evaluation, 3 (8.3%) of the 87 hips had Brooker I heterotopic ossification. Of the 87 prostheses, 86 were fixed in place, and no instances of frank loosening were noted. No patients were found to have continuous radiolucent lines. There was no evidence of migration of any acetabular or femoral component.
Complications
This is a high-risk patient group and naturally had multiple preexisting diseases and different medical complications. Thus, a distinction is made between implant-related complications and nonimplant-related ones. Table 3 lists the nonimplant-related medical complications encountered during hospitalization.
Medical Complications.
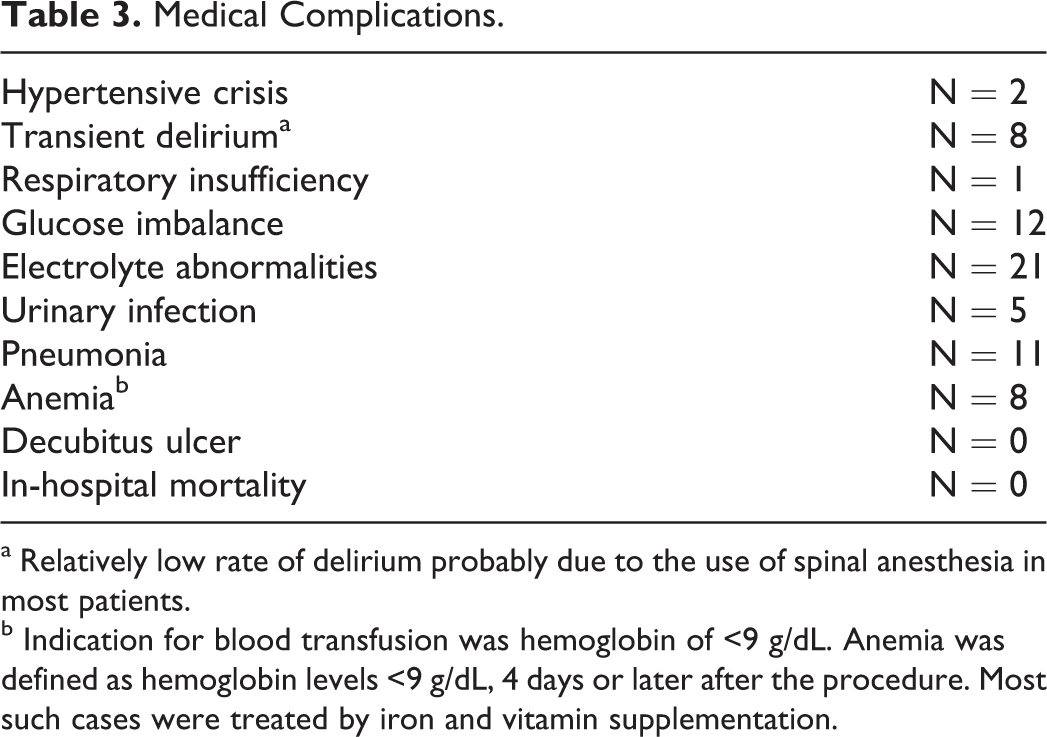
a Relatively low rate of delirium probably due to the use of spinal anesthesia in most patients.
b Indication for blood transfusion was hemoglobin of <9 g/dL. Anemia was defined as hemoglobin levels <9 g/dL, 4 days or later after the procedure. Most such cases were treated by iron and vitamin supplementation.
Implantation-related complications were as follows: 2 patients had clinically evident deep vein thrombosis requiring long-term anticoagulation.
Hemoglobin dropped to 2.5 ± 1 g/dL on average. Seventy-two patients received blood transfusions (averaging 1.2 ± 1 pints). Maximal blood transfusion requirement was 5 pints (a pint equals 450 mL).
In 2 patients, the prostheses dislocated. In both cases, the dislocation was due to ring displacement and the inner head dislocated. One case was infected, and the patient was treated by a Girdlestone procedure. In the other case, the prosthetic head was revised. The patient remained asymptomatic and at 4-year follow-up had an HOOS of 85.
Discussion
Appropriate treatment for the patient group described in the current study is debatable. One option to reduce the dislocation rate in elderly patients with poor muscle function might be a large head, 9 either as part of a total hip system or a hemiarthroplasty. According to the Appropriate Use Criteria for the Treatment of Hip Fractures in the Elderly by the American Academy of Orthopaedic Surgeons (AAOS; 2015, http://www.aaos.org/uploadedFiles/PreProduction/Quality/AUCs_and_Performance_Measures/appropriate_use/Hip%20Fx%20Tx%20AUC.pdf), a displaced subcapital fracture should be treated by hemiarthroplasty/total hip arthroplasty in a high-demand patient without prior arthritis, whereas in a low-demand patient, total hip arthroplasty is considered as possibly indicated. The population reported here is somewhat different than that described by the guidelines, as it is composed of relatively sick patients with a fairly high function despite their disease causing a limitation of muscular control. It appears, from this series, that constrained prosthesis is a suitable treatment for patients with poor muscular control having subcapital fractures with relatively good overall functional status. The functional results appear to be superior to those of bipolar arthroplasty and similar to the results of primary total hip reported in the literature, 10,11 while the dislocation risk is <3%. These results concur with the AAOS guidelines that conclude that moderate evidence supports a benefit to total hip arthroplasty in properly selected patients with unstable (displaced) femoral neck fractures (http://www.orthoguidelines.org/guideline-detail?id=1239). In general, cemented stems appear to be preferred to cementless ones due to a risk of shaft fracture in the latter (http://www.orthoguidelines.org/guideline-detail?id=1274). Both approaches yielded acceptable functional results with low complication rates. The results of the current study indeed show that the results of cementless stems are not inferior to cemented stems, and the risk of dislocation appears to be mitigated by the usage of the retentive cup arthroplasty technique. One of the possible causes of the relatively good results achieved is related to the scheduling of the operations during morning sessions making available the most experienced teams of surgeons, anesthesiologists, and supportive personnel.
A dislocation remains a catastrophic event that might lead to severe patient debilitation. 12 A somewhat worrisome finding appears to be the tendency of the ring to dislodge, as in the 2 dislocations that occurred in this series. This might indicate that an engineering design change is required to make the ring less deformable, as with other designs, the dislocation rate without ring disruption appears to be very low. 13
This study is the largest in the literature reporting the results of constrained arthroplasty in high-risk patients with subcapital fracture. As patients were selected to have a minimal FIM mobility score of at least 4, the results cannot be generalized to more severely affected patients who might have less muscular function. However, it is somewhat debatable whether nonambulatory patients require operative treatment of subcapital fractures. The failure rate of constrained prostheses is up to 42%. 13 In the current series, the failure rate (at short-term follow-up) appears to be much lower. This observation might be due to the low patient demand in this selective patient group. Cost is a significant consideration nowadays. However, at least in our country, the cost of this system compares favorably with that of a bipolar arthroplasty, though this might well be a market-dependent pricing that varies elsewhere (Another regional specific issue is the use of cementless stems as compared to cemented stems. The C-Stem was taken of the market locally in 2010, for commercial reasons, the Corail stem was very competitively priced relative to other cemented or cementless stems).
In conclusion, constrained THR using a retentive cup appears to be a viable alternative for mobile patients with poor neuromuscular control. This patient group does not appear to have a particularly high loosening rate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.