
Abstract
Introduction:
Hip fractures are common injuries with high morbidity and mortality rates. These patients often become anemic and require allogenic blood transfusion. Transfusions are costly with potential complications. This study examines the effect of intravenous (IV) iron on patients with hip fractures, undergoing surgery within 48 hours, and being treated with a highly restrictive transfusion protocol.
Materials and Methods:
A retrospective chart review performed on patients admitted to a level 1 tertiary care center with fractures of the proximal femur from December 2015 to December 2017 included 239 patients. Patients who received 300 mg of IV iron when their hemoglobin fell below 11 g/dL were compared to a control group of patients who never received IV iron with respect to transfusion rate, 30-day readmission rate, nosocomial infections, length of stay, and hospital costs.
Results:
There were no significant differences in transfusion rates (P = .118). There was a trend toward decreased length of stay (P = .063) and 30-day readmission rates (P = .051) with a 59% reduction in the odds of 30-day readmission when a patient received IV iron. There were no differences in nosocomial infection rates or cost of hospitalization.
Discussion:
This study presents a compelling argument for further research regarding the use of IV iron in elderly patients undergoing surgery for a hip fracture. Length of stay and transfusion rates are increased in patients with intertrochanteric fractures and undergoing intramedullary nailing. A higher number of these patients in the IV iron group may have falsely increased these rates. A prospective, randomized, controlled trial is needed to assess the true effects of perioperative IV iron.
Conclusions:
This study showed no significant benefit to IV iron use in elderly patients undergoing surgical treatment of hip fracture. The decrease in 30-day readmission rate should be further examined with a prospective randomized controlled trial.
Introduction
Hip fractures are a common injury in the United States with greater than 320 000 related admissions yearly in patients older than 65 years. 1 With an increase in life expectancy and an aging population, it is estimated that the rate of hip fractures worldwide will increase from 1.66 million per year in 1990 to 6.36 million per year in 2050. 2 The fracture itself combined with surgical treatment result in significant blood loss as well as anemia, a common problem following these injuries; more than 80% of these patients have a hemoglobin concentration of <11 g/dL during their hospital course. 3 This anemia, and its symptoms, is often addressed with allogenic blood transfusion. Up to 74% of these patients require perioperative transfusion. 4 While major adverse events associated with allogenic blood transfusions are relatively rare, they are not without risks including infection, hemolytic reaction, transfusion-related acute lung injury, transfusion-associated circulatory overload, minor febrile reactions, and increased length of hospital stay. 3 There is also significant monetary cost associated with transfusions. 5,6 For these reasons, efforts have been made to reduce the rate of transfusion among these patients while still addressing their anemia.
One proposed method of decreasing the transfusion rates in hip fracture patients is to administer intravenous (IV) iron. The use of IV iron therapy, alone or in addition to erythropoietin (EPO) administration, has been studied in other surgical specialties. 7 In more recent years, research has been done to address the use of IV iron on orthopedic patients undergoing total knee arthroplasty, total hip arthroplasty, or surgical treatment of a hip fracture. To date, the results have been varied with a limited number of prospective studies. 4,7 - 12 Several studies addressing the use of IV iron have been performed in institutes whose transfusion protocol dictates the administration of blood products for hemoglobin of less than 8 g/dL or 10 g/dL. 4,7 -9 Recent literature has demonstrated safety of highly restrictive transfusion protocols. 13 -15 Additionally, studies examining IV iron use in hip fractures have used protocols wherein the patients do not undergo surgery until 72 hours after admission. 4,8,9,12 More recently, it has been recommended that patients undergo surgical intervention for hip fracture within 48 hours, if they are medically optimized, to improve patient outcomes. 13,16 -18
Due to the varied results and recent alterations in management of hip fractures, further studies are needed to assess the efficacy of IV iron in patients undergoing surgery for hip fractures; particularly, IV iron use in an institute utilizing a restrictive transfusion protocol for patients undergoing surgery within 48 hours should be examined as this has become the standard of care. This study aims to examine the effect of IV iron administration on transfusion rates, in-hospital mortality, and 30-day readmission rates while also assessing its effect on nosocomial infections rates and hospital admission costs.
Materials and Methods
This was a retrospective chart review study conducted with approval from the institutional review board. A search was conducted to find all patients admitted to Cleveland Clinic Akron General Medical Center with the diagnosis of a fracture of the proximal end of the femur between December 2015 and December 2017. Inclusion criteria consisted of all patients aged greater than 60 years who underwent hemiarthroplasty, intramedullary nailing, sliding hip screw fixation, or closed reduction percutaneous pinning of a proximal femur fracture, and whose hemoglobin fell below 11 g/dL on that admission. Patients were excluded if they were transfused on admission, did not have a hemoglobin below 11 g/dL throughout their hospital course, had dialysis-dependent chronic kidney disease, were in liver failure, had a known malabsorption disorder, had a known blood dyscrasia, had an active infection at the time of admission, or were less than 60 years of age.
Of the 414 charts reviewed, 239 patients met inclusion criteria (Table 1). Certain data that may have affected their transfusion requirements, such as age, gender, preoperative anticoagulant use, and admission hemoglobin level were collected. Injury and treatment-specific data were also collected including fracture type, surgery performed, postoperative hemoglobin levels, postoperative anticoagulation, length of stay, and direct hospital costs associated with admission. Lastly, data pertaining to postoperative complications were collected such as postoperative red blood cell transfusion data, presence and type of nosocomial infection, 30-day readmissions, and in-hospital mortality.
Patients Excluded From the Study at Initial Time of Chart Collection.
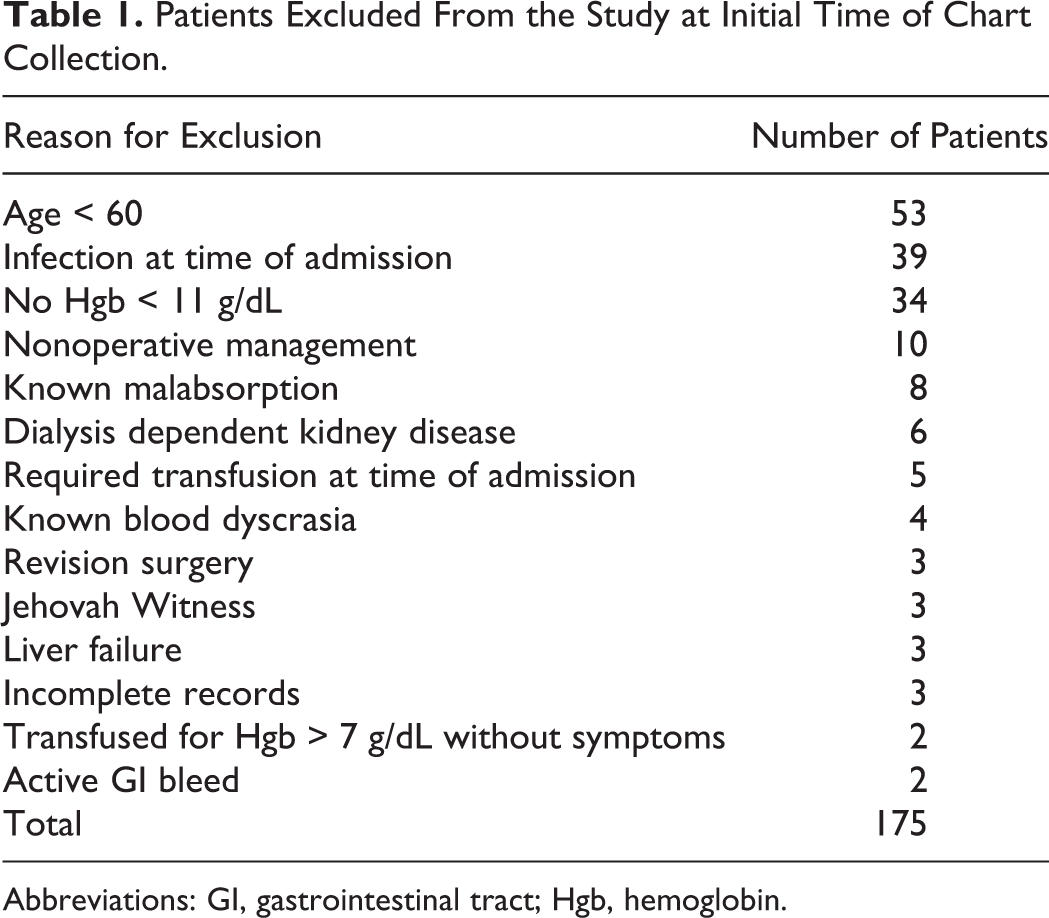
Abbreviations: GI, gastrointestinal tract; Hgb, hemoglobin.
Patients were divided into 2 groups for comparison, IV iron and control. The IV iron group consisted of patients who received 300 mg of Venofer (Vifor France Company, Levallois-Perret, France) as a single dose at the time that their hemoglobin fell below 11 g/dL. Venofer was chosen as the IV iron formulation to be used as iron sucrose has been found to have the lowest number of adverse events when compared to sodium ferric gluconate and iron dextran. 19,20 The control group included patients who did not receive IV iron when their hemoglobin level fell below 11 g/dL. Intravenous iron was used in patients at the discretion of the attending surgeon or resident physician.
There were otherwise no differences in patient management between the 2 groups. The same transfusion protocol was applied to all patients; both pre and postoperatively, patients were transfused if their hemoglobin fell below 7 g/dL or if they developed symptoms of anemia, such as tachycardia, acute kidney failure, shortness of breath, or dizziness, among others. All patients had a complete blood count drawn on admission and postoperatively for a maximum of 3 postoperative days unless clinically indicated. Patients were discharged upon medical stability or extended care facility placement and insurance approval. Discharge disposition was determined by a collaboration between the primary surgeon and the physical therapy department.
Data were compared between the IV iron and control groups. Specifically, categorical data were compared with Pearson χ2 tests with Fisher exact testing as appropriate. Continuous data were tested for normality with Shapiro-Wilk tests; non-normally distributed data were then compared to Mann-Whitney U tests. A significance threshold of .05 was chosen for all statistical analyses.
Results
A total of 414 charts were reviewed. Once exclusion criteria were applied, 239 patients were included in the study, 119 in the IV iron group and 120 in the control group. There were no significant differences between groups with respect to patient age, gender, medical comorbidities (ie, diabetes and congestive heart failure), preoperative anticoagulant use, or aspirin use (P > .126, Table 2). There was a significantly higher proportion of patients who sustained peritrochanteric, that is, intertrochanteric and subtrochanteric, hip fractures, compared to femoral neck fractures, in the IV iron group (P = .002). There was also a significantly higher rate of intramedullary nailing performed in the IV iron group, and a significantly higher number of patients treated with hemiarthroplasty in the control group (P = .035, Table 3).
Demographic Data for the Control Group and IV Iron Group.
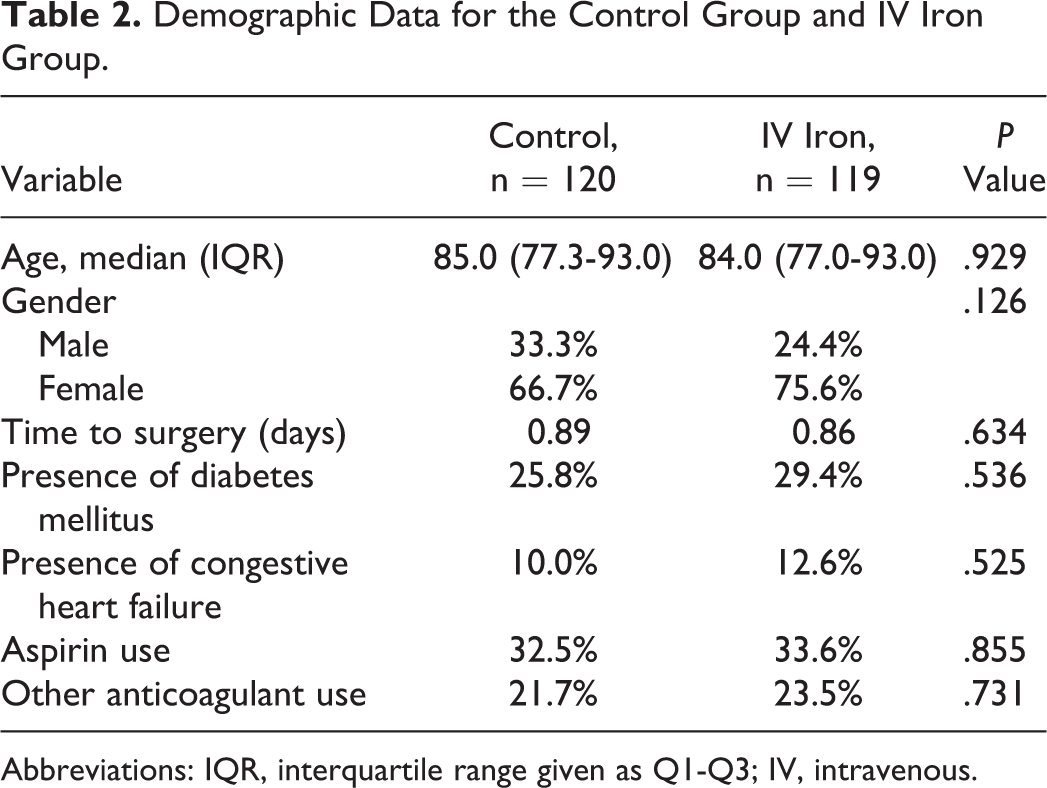
Abbreviations: IQR, interquartile range given as Q1-Q3; IV, intravenous.
Data Demonstrating the Distribution of Fracture Types and Surgeries.
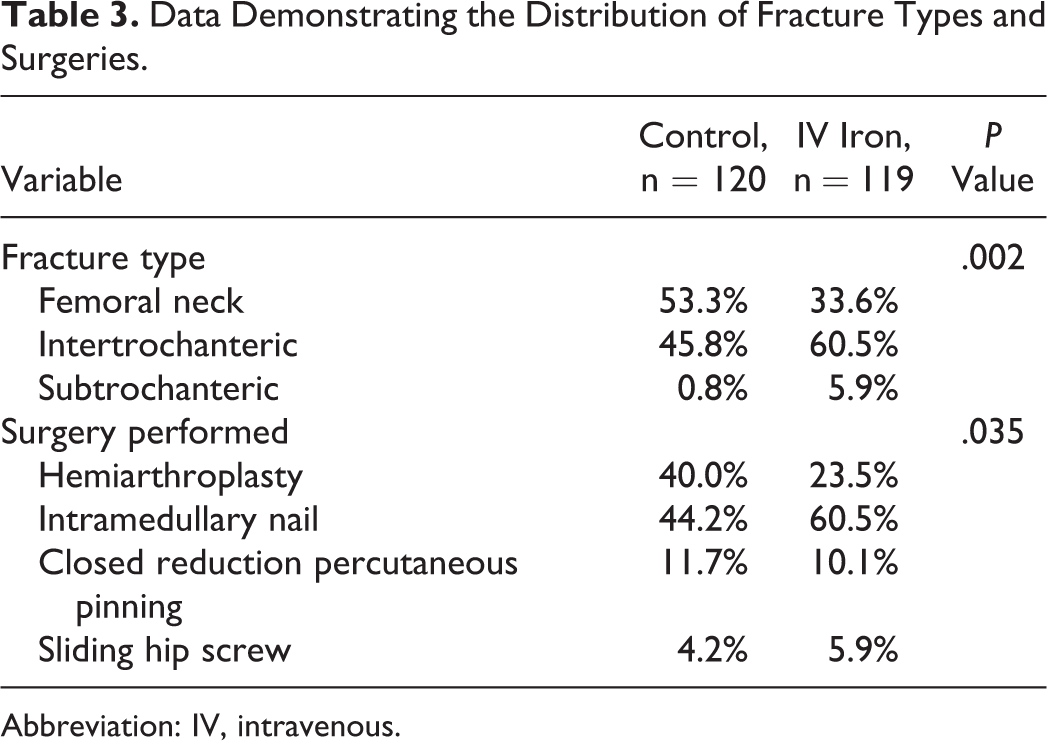
Abbreviation: IV, intravenous.
Twenty-three (19.2%) patients in the control group required allogenic blood transfusion, whereas 33 (27.7%) patients required it in the IV iron group (P = .118; Table 4). There was a higher number of patients requiring allogenic blood transfusion with peritrochanteric fractures when compared to femoral neck fractures (P = .011). Patients who underwent intramedullary nailing had a greater likelihood of receiving allogenic blood transfusion, while patients who underwent closed reduction with percutaneous pinning were the least likely to require transfusion (P = .007). Because of the large number of primary surgeons in this study (9), surgeon-specific data were analyzed, and it was found that no one surgeon had a higher rate of transfusion than the others.
Transfusion Data as Associated With IV Iron Use, Fracture Type, and Surgery Type.
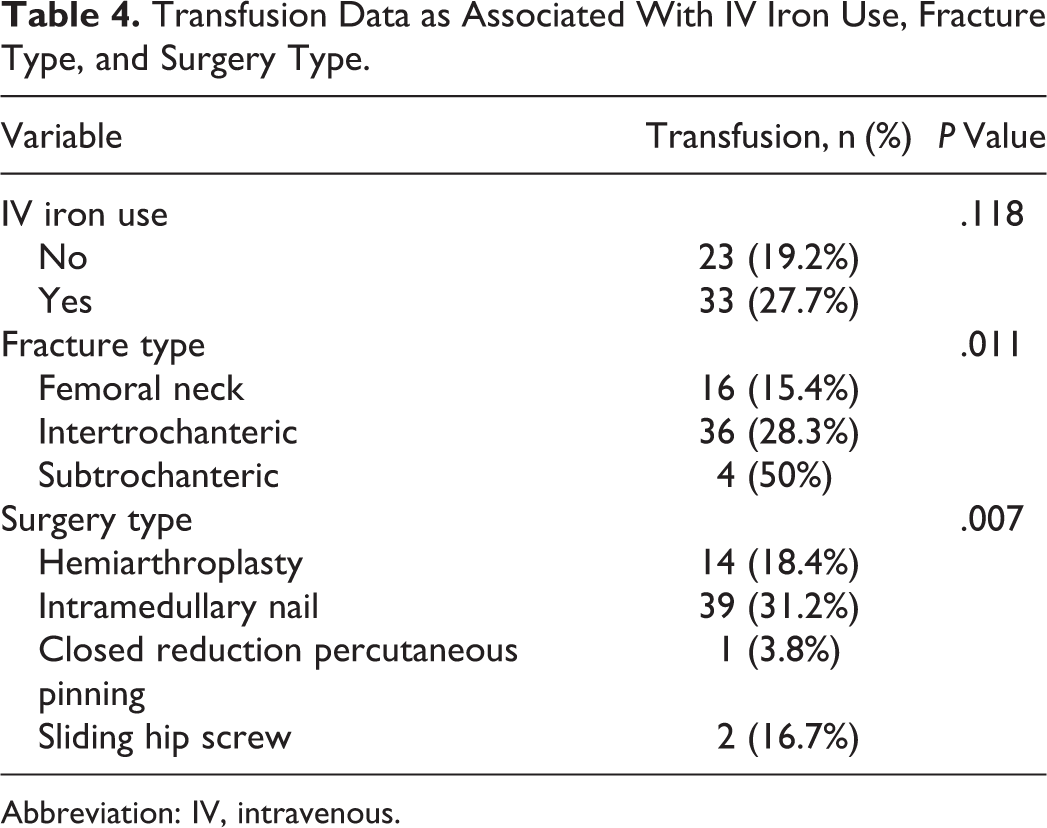
Abbreviation: IV, intravenous.
Secondary outcome results are reported in Table 5. Specifically, there was a trend toward lower 30-day readmission rates and shorter length of hospital stay for patients in the IV iron group, however, neither of these variables reached statistical significance (P = .051 and P = .063, respectively). Despite not achieving statistical significance, when a patient was given IV iron, the odds of having a 30-day readmission were reduced by 59% compared to patients who received no intervention when their hemoglobin fell below 11 g/dL. Of note, there were zero incidences of in-hospital mortality in either group. Direct cost data, such as procedures, imaging, and laboratories, were collected, while excluding administrative fees. There were 12 patients for whom cost data could not be collected due to a change in electronic medical records system and cost model during the study time period. There was no significant difference in direct hospital costs between the 2 groups with a median (interquartile rage) cost of US$ 7891 (US$ 6834-US$ 9798) in the control group and US$ 7891 (US$ 6706-US$ 9152) in the IV iron group (P = .469, Table 5).
Summary of Secondary Outcome Results.

Abbreviations: IQR, interquartile range given as Q1-Q3; IV, intravenous.
Discussion
Hip fractures are a common injury with high rates of morbidity and mortality. The expectation is that the incidence of these injuries will increase considerably with the aging population. Due to the nature of these fractures, the surgeries used to treat them, and the patient population typically affected, a large majority of these patients develop anemia, with hemoglobin dropping below 11 g/dL in more than 80%. 3 To date, the mainstay of treatment of this anemia has been allogenic blood transfusion. However, due to associated costs and complications related to these transfusions, efforts have been made at reducing transfusion rates.
This study aimed to examine the effect of IV iron administration in a restrictive transfusion model on transfusion rates, in-hospital mortality, and 30-day readmission rates while also assessing its effect on nosocomial infections rates and hospital admission costs. No differences were found in transfusion rate, nosocomial infection rate, in-hospital mortality, or direct hospital costs. These results are in concordance with those found by Cuenca et al who found a 20% reduction rate in transfusions in patients with intertrochanteric hip fractures and a reduction of 59.2% in femoral neck fractures, neither of which were statistically significant. In addition, Cuenca et al found a 31.1% reduction in transfusion rates in patients treated with IV iron, which again was not statistically significant. In fact, a study by García Erce et al was the only one to date showing a statistically significant reduction in transfusion rate, and they gave patients EPO in addition to IV iron. The study presented here actually demonstrated an 8% increase in transfusion rates in patients receiving IV iron.
The presented study had a higher proportion of intertrochanteric and subtrochanteric femur fractures undergoing intramedullary nailing in the IV iron group. Peritrochanteric femur fractures and intramedullary nailing are reported in the literature as an independent risk factor for transfusion when compared to femoral neck fractures and closed reduction percutaneous pinning and that is supported by the results of this study. 21 -23 Because peritrochanteric fractures have higher transfusion rates, and there was a higher proportion of them in the IV iron group, it is possible that the transfusion rates were falsely elevated in that group.
The results of this study demonstrated a trend toward reduced 30-day readmission rates in patients receiving IV iron with the odds of a 30-day readmission reduced by 59% when a patient was treated with IV iron. The reduction in 30-day readmission is in agreement with a previous paper by Erce et al, which showed similar results when giving EPO in addition to IV iron. Reducing 30-day readmissions is a crucial factor for a multitude of reasons. Firstly, hip fractures have a high mortality rate within the first year postinjury, and this risk is increased when a patient requires a readmission into the hospital within 30 days of treatment. It has been shown that almost 20% of patients readmitted die during that admission, and the 1-year mortality rate for patients readmitted within 30 days is more than double that of those who are not readmitted. 24 In addition to improvements in the overall health and outcomes of patients, there is a push to reduce 30-day readmission rates from a monetary standpoint. Recently, insurance companies have been enacting stricter ramifications when a patient is readmitted to the hospital within 30-days of previous discharge. For both of these reasons, among others, it is important to utilize all reasonable resources to avoid 30-day readmissions and the consequences that arise from them.
This study also found a trend toward shorter hospital stay in patients receiving IV iron. Reducing length of hospital stay following hip fractures would not only reduce cost to the patient and burden on the health-care system but it would also reduce possible exposure time of frail patients to hospital acquired infections and likely improve patient comfort.
There are limitations to this study. The most notable being that it was conducted as a retrospective chart review rather than a prospective randomized controlled trial. Due to our hospital implementation of a highly restrictive transfusion protocol, the transfusion rate found in this study was lower than those reported in the literature. 2,21 -23 As a result, the study was underpowered to detect a difference in transfusion rates between those receiving IV iron and those receiving no supplementation. The study would have required more than 600 patients per group to achieve at least 80% power, which could not be achieved in the time frame within which medical records can be accessed at this institute. Lastly, we did have a higher proportion of peritrochanteric fractures in the IV iron group. Because peritrochanteric hip fractures are a risk factor for transfusion, and these patients had higher rates of transfusion in this study, it is possible that this could mask differences in transfusion rates between the 2 groups. Future studies could be designed to control for fracture type.
With the continued goal of reducing the necessity of transfusions and readmissions in patients undergoing surgery for treatment of a hip fracture, IV iron remains a plausible treatment option. Varying results in studies to date, as well as changes to the standard of care in treating these patients, mandates further investigation of IV iron. Ideally, a large-scale, prospective, randomized controlled trial isolating IV iron administration as a single variable should be conducted to accurately assess the efficacy of perioperative IV iron use in these patients.
Conclusion
This study demonstrates no statistically significant benefit to administration of IV iron to patients undergoing operative treatment of a hip fracture. It does show a trend toward reduction in 30-day readmission rate which may be clinically significant and should be studied further.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.