
Abstract
Introduction
Previous clinical studies have reported associations between the acromion index, lateral acromion angle, and critical shoulder angle and the occurrence of rotator cuff tears. The objective of this study was to analyze the correlations of these different anatomic parameters in geriatric Chinese Population.
Methods
Healthy geriatric Chinese participants (n = 66) and geriatric Chinese patients with rotator cuff tears (n = 70) identified between January 2019 and October 2020 were included in this study. Standardized true anteroposterior radiographs were used to measure the acromion index, lateral acromion angle, and critical shoulder angle in each study participant.
Results
The mean acromion index was significantly larger, the mean lateral acromion angle was significantly smaller, and the mean critical shoulder angle was significantly larger in geriatric patients with full-thickness rotator cuff tears compared with geriatric healthy participants.
Conclusion
There were a negative linear relationship between the acromion index and lateral acromion angle and a positive linear relationship between the acromion index and critical shoulder angle in geriatric patients with rotator cuff tear and geriatric healthy participants; we termed this phenomenon “Hypothesis of Acromion Index.” The acromion index, lateral acromion angle, and critical shoulder angle are independent predictors of rotator cuff tears in a geriatric Chinese population.
Keywords
Introduction
The potential relationship between variations in acromion morphology and rotator cuff tears has been investigated in multiple studies. 1 –4 Many of these used anthropometric techniques to identify a number of relevant parameters, including the acromion index (AI), the lateral acromion angle (LAA), and critical shoulder angle (CSA). The causal relationship between the variation of lateral acromial extension and the risk of a full-thickness rotator cuff tear was first investigated by Nyffeler et al. 5 who originally defined the AI. They found that a larger lateral extension of the acromion provided a higher ascending force than a smaller lateral extension of the acromion during abduction of the shoulder and a high AI was associated with risk of full-thickness rotator cuff tear. Banas et al. 6 revealed that a significant correlation between the LAA and rotator cuff changes by MRI, the LAA may be useful for evaluating patients have or to be at risk for rotator cuff tear. They reported an association between the angle of lateral tilt of the acromion and the prevalence of subacromial tear. Moor et al. 7 developed a radiological parameter, the CSA, which took into account both the tilt of the glenoid in the frontal plane and the AI. They showed that the CSA was correlated with wear of the rotator cuff tendons and the articular cartilage of the glenohumeral joint but eliminated the influence of degenerative changes in the humerus. In a second study, Moor et al. 8 evaluated the predictive power of the AI, LAA, and CSA to determine the presence of degenerative rotator cuff tear. They concluded that the CSA was the most valuable measure to distinguish between patients with intact rotator cuff tendons and those with torn rotator cuff tendons. Interestingly, we noted that all these parameters use the surface of the glenoid cavity as the baseline for measurement. Therefore, we hypothesize that the relationship between the AI, LAA, and CSA is relevant in the diagnosis of rotator cuff tears.
In this study, we evaluated radiologic parameters of acromion morphology in two geriatric Chinese populations. The objective of the study was to identify correlations between the AI, LAA, and CSA in a healthy geriatric Chinese population and in geriatric Chinese patients who suffer from rotator cuff tears.
Methods
Ethics
The experimental protocol was established according to the ethical guidelines of the Helsinki Declaration, and ethical approval for this study was provided by Ethics Committee. Each survey participant provided written informed consent. All methods were performed in accordance with the relevant guidelines and regulations.
Study Subjects
Distribution of Groups According to Gender, Mean Age, Side.
RCTs, Rotator cuff tears.
Radiologic Parameters of Acromion Morphology
Standardized true anteroposterior radiographs were used to measure AI, LAA, and CSA in geriatric healthy participants and patients with rotator cuff tears (Figure 1). Individuals stood in front of an X-ray cassette with a neutral rotation of the forearm and the arm at the side of the body without any abduction. The coronal plane of the body was rotated until the glenoid plane was vertical to the X-ray cassette. The X-ray beam was directed horizontal to the glenoid plane. The measurements were recorded by two independent observers. Standardized true anteroposterior radiographs (A): The outline of the glenoid is a line (a), the middle part of the clavicle is overlapping (b), and the joint space is visible (c). Standardized anteroposterior radiographs (B): The outline of the glenoid is an oval (a), the middle of the clavicle is straight (b), and the outline of the glenoid and head of the humerus overlap (c).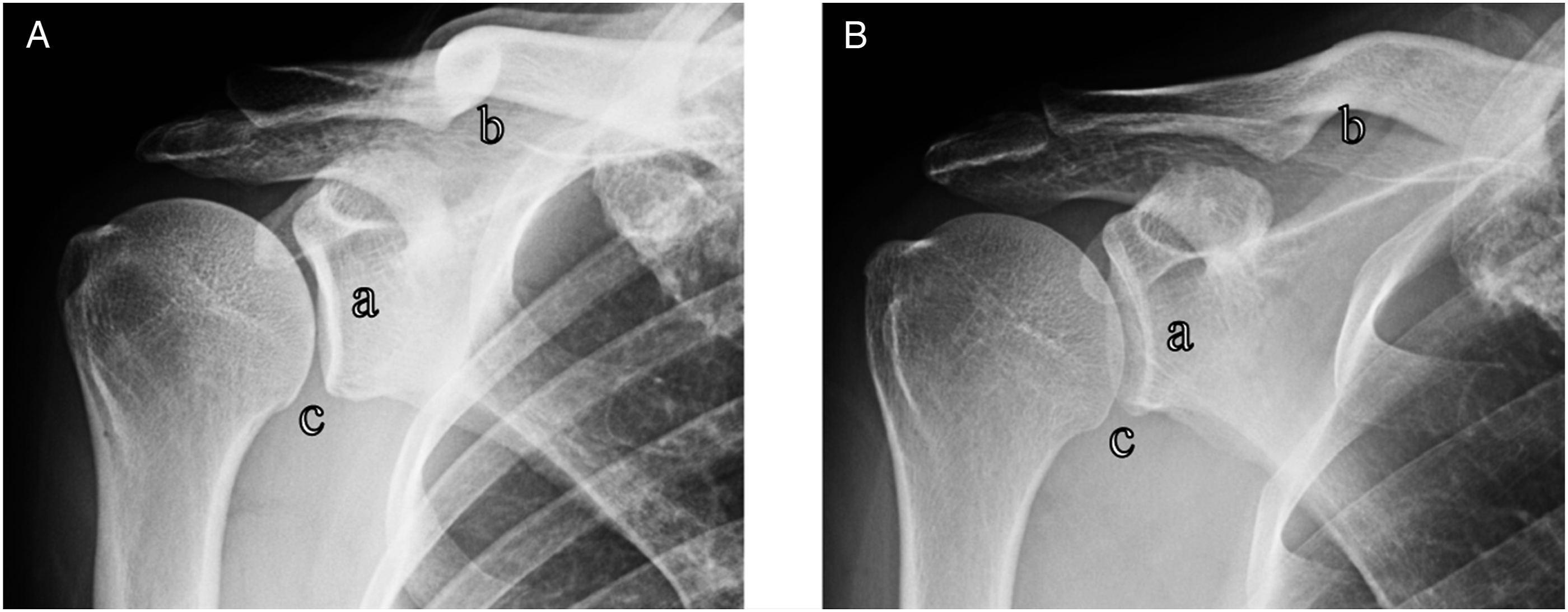
Acromion Index
As shown in Figure 2, line “a” represents the glenoid plane, connecting the superior and inferior borders of the cortical bone of the glenoid. Line “b” and line “c” are parallel to line “a” and at a tangent to the lateral border of the acromion and proximal humerus, respectively. The AI was defined as the ratio between the distance from line “a” to line “b” (GA) and the distance from line “a” to line “c” (GU).
5
The acromion index was calculated by dividing the distance from line “a” to line “b” (GA) by the distance from line “a” to line “c” (GH). The lateral acromion angle (lateral acromion angle, angle α) was assessed between line “a” and line “d.” The critical shoulder angle (critical shoulder angle, angle β) was assessed between line “a” and line “e”.
Lateral Acromion Angle
The LAA (angle α) is formed by the intersection of line “a” and line “d.” Line “d” (the proximal line) is parallel to the sclerotic line of the cortical undersurface of the acromion (Figure 2).
Critical Shoulder Angle
The CSA combines the measurements of inclination of the glenoid and the AI. The CSA is formed by line “a” and line “e.” Line “e” extends from the inferolateral point of the acromion to the inferior fossa margin of the glenoid (Figure 2).
Statistical Analyses
Statistical analyses were performed using SPSS statistical software (version 21.0). The post observed power analysis was done. According to the formula of sample size, the average AI was .6 in control group and .7 in rotator cuff tear group. The standard deviation (SD) of AI was .1 in two groups, the power was .9, the alpha was .05, and the result is needed at least 24 patients in each group. On the basis of observed correlations of −.813–.912, at α = 5% and power = 80%, a sample of ten cases was required. Since the sample size taken was quite high as compared to the required sample size, we can say that the power of our study is very high. Between-group comparisons were evaluated using Student’s t-test and chi-square test. Correlations between parameters were investigated with Pearson’s correlation test. Statistical significance was set at P < .05.
Results
Results of AI, LAA, CSA.

AI, acromion index; LAA, lateral acromion angle; CSA, critical shoulder angle; SD, standard deviation; RCTs, rotator cuff tears.
There was a negative linear relationship between the AI and LAA (rotator cuff tears: R2 = .5417, P< .001, r = −.759, P< .01; healthy participants: R2 = .6168, P< .001, r = −.813, P< .01) and a positive linear relationship between the AI and CSA (rotator cuff tears: R2 = .5611, P< .001, r = .854, P< .01; healthy participants: R2 = .5437, P< .001, r = .912, P< .01) in geriatric healthy participants and patients with rotator cuff tears (Figures 3 and 4). Patients with rotator cuff tears: There were a negative linear relationship between acromion index and lateral acromion angle and a positive linear relationship between acromion index and critical shoulder angle. Healthy participants: There were a negative linear relationship between acromion index and lateral acromion angle and a positive linear relationship between acromion index and critical shoulder angle.

Discussion
In contrast to other studies, we measured three radiologic parameters of acromial morphology in each geriatric healthy participant or geriatric patient using the same true standardized anteroposterior radiograph. In the geriatric Chinese patients (average AI and standard deviation was .71 ± .05), we found the consistent results with Nyffeler et al. that the lateral extension was positively correlated with the lateral extension of by Nyffeler et al. in the Swiss population (average AI and standard deviation was .73 ± .06), and the data on healthy geriatric Chinese population (average AI and standard deviation was .64 ± .06) also matched on healthy Swiss population (average AI and standard deviation was .64 ± .06). However, Nyffeler et al. 5 found that the average AI and standard deviation was .60 ± .08 in Swiss population with primary osteoarthritis; this phenomenon has not been proved in the geriatric Chinese population. One of the most important reasons was that the incidence was low in geriatric Chinese population with primary osteoarthritis of shoulder. Indeed, in our study, no patient with osteoarthritis of shoulder was found. In our study, the mean LAA (77.0°) of the patients with rotator cuff tears was significantly larger than the one reported by Banas et al (less than or equal to 70°). 6 The different measurement methods were the main reason for this phenomenon that we used DR, but Banas et al. used MRI to measure LAA. The measurement by DR was conducive to analyze the correlation between AI and LAA, and CSA comprehensively. The CSA was measured on standard true radiographs of three groups (asymptomatic, shoulder with RCT, shoulder with primary osteoarthritis) by Moor et al.;7,8 however, two groups (patients with RCT and healthy participant) were measured in our study. In this study, the same positive correlation between a large acromial cover with an upwardly tilted glenoid fossa and RCT was found as that reported by Moor et al.
In addition, we demonstrated two other phenomena. First, we found an inverse relationship between the AI and LAA; the lateral extension of the acromion increased as the inclination of acromion increased. Second, we found a positive relationship between the AI and CSA; the lateral extension of the acromion increased as the angle between the line connecting the lowest point of the glenoid plane and the inferolateral point of the acromion and a line delineating the glenoid plane increased. We call this phenomenon the “Hypothesis of Acromion Index.”
The Hypothesis of Acromion Index was needed to undergo a multi-center study; however, this study is just a correlational analysis and the limitations of conclusions have to be taken into account. There were several limitations associated with this study. First, we did not account for a possible association between the shape of the acromion and the presence of rotator cuff tear in our study participants. Second, we did not account for a possible association between the acromiohumeral interval and the presence of rotator cuff tear. Third, our study was performed in a geriatric Chinese population, and the findings may not be generalizable to populations in other regions. Fourth, the age difference between the patients with geriatric rotator cuff tears and healthy participants may have affected the results. Finally, this study does not take into account the intrinsic pathology of rotator cuff tear and the correlation between rotator cuff tear and factors such as diabetes, genetics, and smoking.
Conclusion
Our study revealed an interesting phenomenon and we named it the “Hypothesis of Acromion Index.” The implication of the “Hypothesis of Acromion Index” is a negative linear relationship between the acromion index and lateral acromion angle and a positive linear relationship between the acromion index and critical shoulder angle in patients with rotator cuff tear and healthy participants. These findings imply that the lateral extension of the acromion, the upward tilt of the glenoid fossa, and the downward tilt of the acromial cortex represent relevant risk factors for rotator cuff tear.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Startup Foundation for Doctors of Dalian University (Serial Number, 20152QL003), the funder was MY who conceived the research idea and participated in its design.
Ethics Approval and Consent to Participate
Ethics approval was obtained from the Ethical Research Committee of Affiliated Zhongshan Hospital of Dalian University. All participants provided written informed consent before the commencement of the study. Ethical Research Committee of Affiliated Zhongshan Hospital of Dalian University approved this study involving human participants.