
Abstract
Background
No evaluation has been done on the relationship of the acromion–greater tuberosity impingement index (ATI) with retear after arthroscopic rotator cuff repair (ARCR). Our purpose was to evaluate whether a higher ATI is associated with retear after ARCR.
Methods
132 patients received ARCR and underwent MRI scan at a one year follow-up to assess tendon healing, and the findings were graded no retear (NR), partial-thickness retear (PR) or full-thickness retear (FR). The ATI, the critical shoulder angle (CSA), acromion index (AI) and lateral acromial angle (LAA) were measured with postoperative radiographs. Functional scores were obtained preoperatively and at a one year follow-up.
Results
Postoperative Constant scores and ASES scores were significantly different between groups with inferior outcomes in the FR group (p < 0.05 for all). The UCLA score was significantly better in the NR group compared with the PR and FR groups (p < 0.05), and in the PR group compared with the FR group (p < 0.05). For ATI and CSA, the values of the PR and FR groups were larger than the NR group (p < 0.05 for all), but there were no significant differences between the PR and FR groups (p > 0.05 for all). No significant differences were observed with regard to the AI and LAA (p > 0.05, respectively). The repair integrity was positively related to the ATI (0.304, p < 0.05) and CSA (0.252, p < 0.05), but not related to the AI or LAA (p > 0.05 for both). ATI was not related to any functional scores (p > 0.05 for all).
Conclusion
This study revealed that the ATI was positively related to rotator cuff retear. Patients with retears had significantly greater ATIs after ARCR. Level of Evidence: III, case–control study.
Keywords
Background
Rotator cuff tear (RCT) is one of the most common causes of shoulder joint pain and mobility dysfunction. The incidence of RCT increases with age, and RCT is usually treated surgically. 1 With advancements in arthroscopic techniques, arthroscopic rotator cuff repair (ARCR) has become the treatment of choice for RCT 2 ; however, RCT may recur postoperatively. 3 Several studies have reported that intrinsic and extrinsic factors may increase the risk of retear.4–6 Abnormal scapular morphology is an important extrinsic factor that increases the retear risk. 4
In the coronal plane, the acromion index (AI), lateral acromial angle (LAA) and critical shoulder angle (CSA), measured in the coronal plane, are potential radiological factors that affect retear risk.7–9 Many studies have reported that larger AIs and CSAs, and smaller LAAs, are associated with a full-thickness RCT.10,11 Because these indicators do not provide information about the greater tuberosity of the humerus, they do not reflect the kinematics of the glenohumeral joint or the distance from the lateral aspect of the acromion to the humeral head. 12
The acromion-greater tuberosity impingement index (ATI) has recently gained interest as an important risk factor for RCT. 12 The ATI is calculated by measuring the distance from the centre of rotation of the humeral head to the humeral greater tuberosity and dividing it by the distance from the centre of rotation of the humeral head to the undersurface of the acromion. This index combines the subacromial space width and acromion type into a single quantifiable parameter. Studies have reported that the ATI is strongly related to degenerative supraspinatus tendon tears and subacromial impingement syndrome. 12 However, to date, no study has evaluated the relationship between the ATI and retear after ARCR.
We evaluated the relationship between the ATI and rotator cuff retear in patients who underwent ARCR and were followed up for at least one year. We hypothesized that a higher ATI would be associated with an increased retear rate after ARCR.
Methods
Study population
We retrospectively analysed the medical records of 217 patients who underwent arthroscopic surgery for RCTs between June 2014 and October 2018. The study protocol was approved by the Institutional Review Board of Wenzhou Medical University, China. Written informed consent was obtained from the participants.
RCTs were diagnosed using preoperative magnetic resonance imaging (MRI) and were confirmed during the surgery. Patients diagnosed with unilateral, partial- or full-thickness tear of the supraspinatus and/or infraspinatus muscle who had persistent symptoms (>3 months) after adequate conservative treatment and regular postoperative follow-up were included in the study. Patients were excluded if they were followed up for less than 12 months or had a massive RCT (anteroposterior length >5 cm, according to the classification system by DeOrio and Cofield) of the supraspinatus and/or infraspinatus muscle, 13 had additional lesions (such as superior labrum anterior or posterior lesion, Bankart lesion or Hill–Sachs lesion requiring repair), acromioclavicular arthritis requiring distal clavicle resection, advanced degenerative arthritis or history of any other surgery for the affected shoulder. After excluding 85 patients, 132 were included in the final analysis: 98 in the no tear (NR), 21 in the partial-thickness retear (PR) and 13 in the full-thickness retear (FR) groups.
Operative procedure
All surgeries were performed by one of two experienced surgeons. During the surgery, patients were placed in a lateral position and received general anaesthesia. Diagnostic arthroscopy was performed, and any associated lesions were managed as appropriate, for example, biceps tendon lesions were treated by tenodesis or tenotomy and osteochondral lesions by chondroplasty. Subacromial bursectomy and decompression were performed to clear the surgical area, and acromioplasty was performed in cases with an anterior osteophyte of the acromion or prominent anterolateral acromial spur. The tear location, size and delamination were assessed. After adequate debridement of the tendon edges, the tear size was measured using a probe under direct arthroscopic visualization. For ARCR, the single- or double-row method was used. The tears were repaired using Healix Peek suture anchors (4.5 or 5.5 mm; DePuy Mitek, Raynham, MA, USA) with or without PushLock anchors (Arthrex, Naples, FL, USA).
Postoperative management
The shoulder was immobilized for the first 6 weeks postoperatively using a shoulder sling with an abduction pillow, which limited internal rotation of the arm to 30–40° and abduction to 20–30°. However, after surgery, hand and elbow movements, as well as shoulder pendulum movements for axillary hygiene, were encouraged immediately. Passive and active range of motion exercises were initiated 3–4 and 6–8 weeks postoperatively, respectively. Muscle strengthening exercises were started 12 weeks postoperatively; participation in sports was allowed at 6 months postoperatively.
Outcome assessment
All patients underwent postoperative MRI (3.0 T scanner) at the 1 year follow-up to assess tendon healing. Postoperative tendon integrity was categorized using the criteria established by Sugaya et al. 14 into types I–V: type I, sufficient thickness with a homogeneously low intensity; type II, sufficient thickness with a partial high-intensity area; type III, less than half the thickness compared with the normal cuff but without discontinuity; type IV, minor discontinuity in less than two slices on oblique coronal and sagittal images; and type V, major discontinuity in more than two slices on oblique coronal and sagittal images. Tendons with type III integrity had PR, while those with types IV or V integrity had FR. Fatty infiltration was evaluated according to the criteria proposed by Goutallier et al. 15 : stage 0, normal muscle without fatty streaks; stage 1, muscle with some fatty streaks; stage 2, presence of more muscle than fat; stage 3, presence of as much fat as muscle; and stage 4, presence of more fat than muscle.
The ATI, AI, LAA and CSA were measured on standard anteroposterior X-ray images (Figure 1). To measure the ATI, a circle was drawn on the image, which followed the contour of the articular surface of the humeral head. This circle marked the medial and upper cartilaginous surfaces to identify the centre. The ATI was calculated using the following equation: ATI = CT/CA, where CT is the distance from the centre of rotation of the humeral head to the humeral greater tuberosity, and CA is the distance from the centre of rotation of the humeral head to the undersurface of the acromion.
12
The AI was calculated using the following equation: AI = AG/HG, where AG is the distance from the acromion to the glenoid, and HG is the distance from the lateral part of the humeral greater tuberosity and the glenoid.
16
The LAA was defined as the angle between a line drawn parallel to the lateral glenoid surface and a line along the undersurface of the acromion.
17
The CSA formed at the intersection of a line connecting the superior and inferior glenoid bone margins and a line connecting the inferior glenoid bone margin and the most lateral acromial border.
18
Radiological outcomes were evaluated by two independent experienced radiologists. (a) ATI, (b) AI, (c) LAA, (d) CSA.
All patients were followed up for a minimum of one year postoperatively. We recorded patient characteristics, demographic data, and preoperative and final Constant scores, American Shoulder and Elbow Surgeons (ASES) scores and Shoulder Rating Scale of the University of California at Los Angeles (UCLA) scores. Data were independently collected and analysed by two orthopaedic surgeons.
Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) software (version 18.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as the mean ± standard deviation and were analysed by one-way analysis of variance followed by Tukey’s post hoc test. Categorical variables are presented as the frequency and percentage and were analysed using the chi-square or Fisher’s exact tests. The intraclass correlation coefficient was used to assess the agreement among individual measurements. Pearson’s correlation was used to evaluate correlations between the ATI and clinical outcomes (Constant score, ASES score and UCLA score). Spearman’s correlation was used to evaluate the correlations between repair integrity and radiological outcomes (ATI, CSA, AI and LAA). All tests were two-sided, and p-values < 0.05 were considered significant.
Results
Preoperative Patient Characteristics and Demographic data.

Notes: NT, no retear; PR, partial-thickness retear; FR, full-thickness retear; ASA, American Society of Anaesthesiologists.
aone-way analysis followed by Tukey’s post hoc test used for analysis.
bchi-square test used for analysis.
Perioperative surgical data.

Notes: NT, no retear; PR, partial-thickness retear; FR, full-thickness retear.
achi-square test used for analysis.
bone-way analysis followed by Tukey’s post hoc test used for analysis.
Pre- and postoperative clinical outcomes.
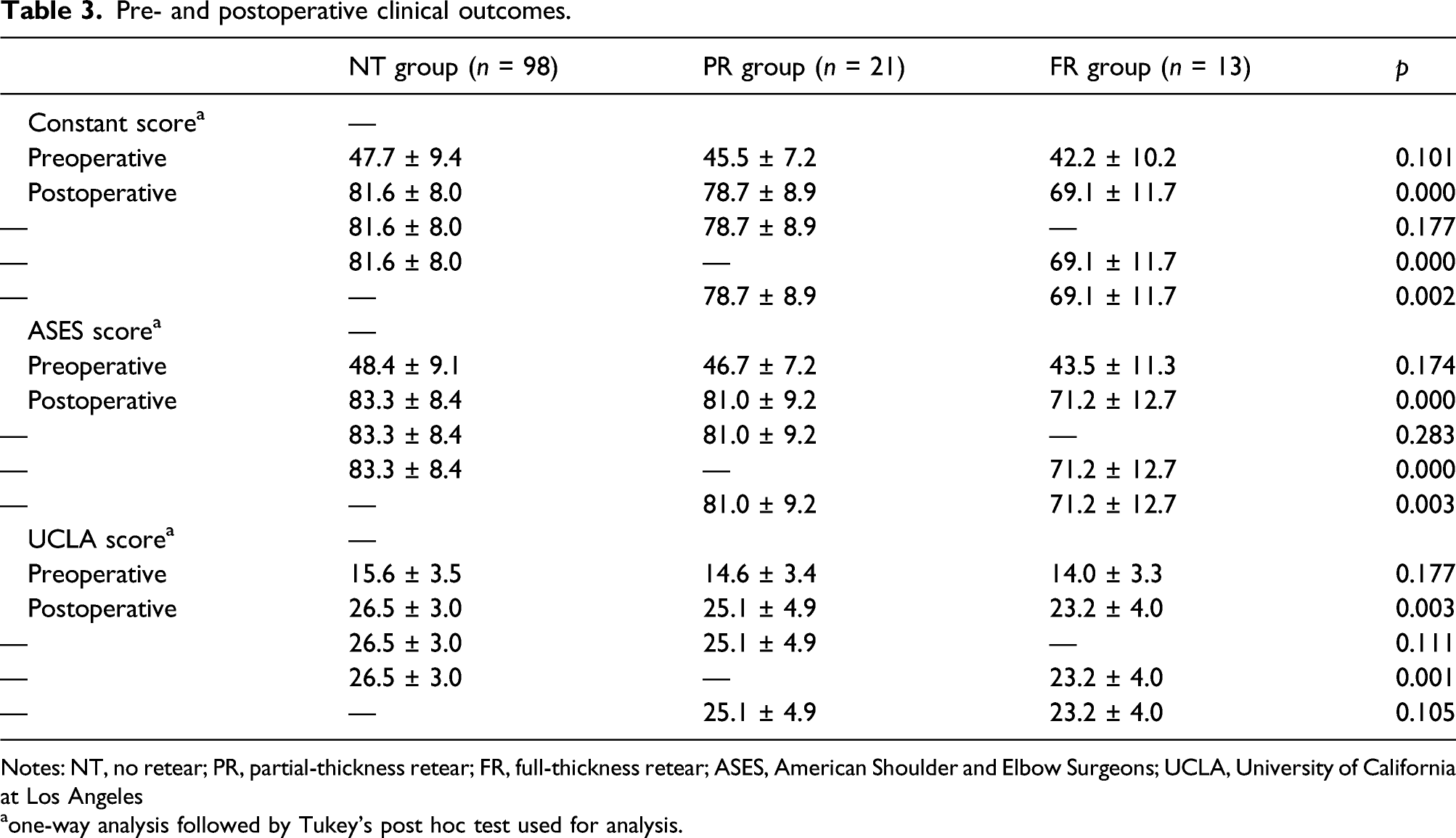
Notes: NT, no retear; PR, partial-thickness retear; FR, full-thickness retear; ASES, American Shoulder and Elbow Surgeons; UCLA, University of California at Los Angeles
aone-way analysis followed by Tukey’s post hoc test used for analysis.
Postoperative radiological measurements.

Notes: NT, no retear; PR, partial-thickness retear; FR, full-thickness retear; ATI, acromion–greater tuberosity impingement index; CSA, critical shoulder angle; AI, acromion index; LAA, lateral acromial angle.
aone-way analysis followed by Tukey’s post hoc test used for analysis.
The correlation between the repair integrity and the radiological indicators.

ATI, acromion–greater tuberosity impingement index; CSA, critical shoulder angle; AI, acromion index; LAA, lateral acromial angle.
aSpearman’s correlation used for analysis.
The correlation between ATI and the clinical outcomes.
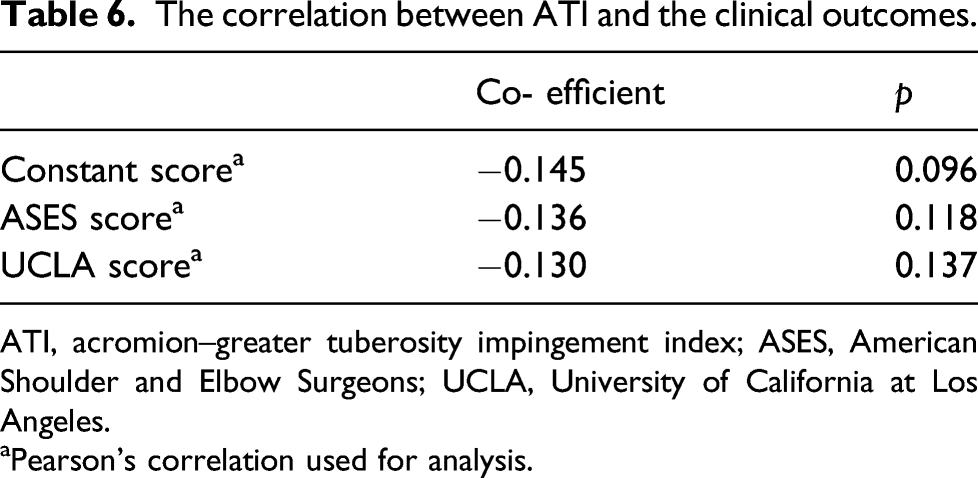
ATI, acromion–greater tuberosity impingement index; ASES, American Shoulder and Elbow Surgeons; UCLA, University of California at Los Angeles.
aPearson’s correlation used for analysis.
Discussion
We found that the ATI was associated with rotator cuff retear after ARCR. To the best of our knowledge, this is the first study to report a correlation between ATI and risk of rotator cuff retear.
Rotator cuff retear is a serious problem because revision surgery is more difficult, more time-consuming, and less effective compared with primary ARCR. 19 The overall retear rate was 26.0%, similar to the rates in previous studies of 10–48.4%. 20 The causes of rotator cuff retear are unclear. Several prognostic factors affect postoperative healing after ARCR, including the patient’s age, initial tear type and size, fatty infiltration of muscle, degree of tendon retraction, repair technique and rehabilitation.21,22 Importantly, these factors were not correlated with retear in the current study, thereby emphasizing the predictive value of radiological parameters. The patient groups were similar in terms of most characteristics, except surgical duration, because large-sized RCTs were included in the FR group.
Previous studies have reported conflicting results regarding the relationships between the retear rate and radiological parameters, such as the CSA, AI, and LAA.7,8,23 The CSA is a strong predictor of degenerative RCTs.4,7 Large CSAs are associated with overloading of the supraspinatus muscle and retear after ARCR due to the biomechanical properties of the rotator cuff. 24 This is supported by the findings of Scheiderer et al. and Garcia et al., who observed that larger CSAs were associated with increased retear rates.25,26 However, some studies have reported opposite results.4,27 In the present study, CSA values were significantly different between the groups with and without retear, with the maximum value in the FR group. This supports the concept that a wide lateral acromion is associated with postoperative tendon healing, as evidenced by the association of the CSA with failure of postoperative repair. 25 The AI and LAA were not associated with the retear rate, which is consistent with recent studies that reported poor specificity and sensitivity of the AI and LAA for rotator cuff diseases.28,29
The ATI is a dynamic radiological parameter that describes the relationship between the acromion and the humeral greater tuberosity, which reflects the width of the subacromial space and acromial type (i.e., causes of RCT). 16 The circle used to calculate the ATI connects the superior rim of the greater tuberosity and inferior tip of the acromion. This circle can be affected by lateral humeral extension (which alters joint biomechanics) and inferior bone spurs (which may cause impingement) on the supraspinatus outlet, which directly reflects the severity of subacromial impingement. Therefore, the ATI accounts for the acromial coverage and changes in the supraspinatus outlet during shoulder motion. In a previous study, we demonstrated that the ATI is a good predictor of degenerative supraspinatus tendon tears and subacromial impingement syndrome. 12 The preoperative ATI may be used to plan and implement the range of acromioplasty required to reduce the incidence of postoperative subacromial impingement. Additionally, we speculated that a reduced ATI could lower the risk of retear after ARCR. 12 In the current study, we found a significant difference in ATI values in the NR group compared with the PR and FR groups, which confirmed that a large ATI increased the risk of retear after surgery.
Significant controversy exists regarding the correlation between scapular anatomy and clinical outcome after ARCR. Garcia et al. 26 observed that an increased CSA was significantly correlated with worse postoperative outcomes at the 6-month follow-up. Zumstein et al. 30 reported that the AI was associated with worse clinical outcomes. Lee et al. investigated the influence of the CSA and AI on clinical outcomes after ARCR. At 6 months postoperatively, an increased CSA was correlated with worse postoperative clinical outcomes. However, no significant correlation was observed at the 24-month follow-up. 31 Li et al. and Scheiderer et al. reported that the CSA and AI did not predict the clinical outcomes after arthroscopic repair of full-thickness tears.7,25 In the present study, we found significantly worse clinical outcomes in the FR group compared with the NR and PR groups, indicating that a full-thickness rotator cuff repair was associated with a poor clinical outcome. This is consistent with the results of previous studies.5,32 Although the ATI was positively related to rotator cuff retear, it was not correlated with the clinical outcome. Importantly, this study included a homogeneous population and excluded patients with massive RCTs and severe glenohumeral osteoarthritis. Additionally, partial-thickness tears are not always associated with a poor clinical outcome; these tears are usually asymptomatic initially and may only be detected during follow-up. 33 Further research is required on this topic.
This study had some limitations. First, owing to the retrospective study design, we did not obtain standardized anteroposterior radiographs for all patients. However, all radiographs were obtained from the same institution, and the radiological parameters (ATI, AI, LAA and CSA) showed good intra- and inter-rater reliability. Second, although one-year follow-up may be sufficient to evaluate the retear rate, long-term outcomes may differ and should be evaluated in future studies. Third, the sample size of this study was small; therefore, this study was underpowered. Finally, two repair techniques (single and double row) were used. It is unclear if this influenced the outcomes. However, many previous studies reported no significant difference in clinical outcomes between the two techniques.34,35
Conclusions
The ATI was positively related to rotator cuff retear. Patients with retears had significantly greater ATIs after ARCR. A large ATI was associated with an increased risk of rotator cuff retear after ARCR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in the study were in accordance
with the ethical standards of the institutional research committee.
Informed consent
Informed consent was obtained from all individual participants included in the study.