
Abstract
Introduction
Geriatric hip fracture patients are characterized by frailty due to multiple comorbidities, such as cardiovascular disease, in which the use of antithrombotics is frequent. The aim of this study is to assess the effect of antithrombotics on perioperative care and patient outcomes after hip hemiarthroplasty following current guidelines.
Materials and Methods
This observational cohort study included all consecutively admitted patients with a femoral neck fracture requiring hip hemiarthroplasty between January 1st 2010, and May 16th 2016, in two level II trauma teaching hospitals. Patients with multiple trauma injuries were excluded.
Results
In total, n = 907 patients (68% female (n = 615), median age 84 years) were included of which n = 142 used a vitamin K antagonist (VKA) and n = 213 used antiplatelet (AP) therapy. Both were associated with more packed cell supplementation (.4 ± 1.1 units and .3 ± .8 units vs .2 ± .6 units, P < .001 and P = .03, respectively). VKA was associated with more hematomas compared no antithrombotics (23% vs 11%, P = .001). VKA had a longer time to surgery compared to no antithrombotics and AP (24 hours vs 19 and 20 hours, P < .001 and P < .001, respectively) and longer admission duration (9 days vs 7 days P < .001. There were no differences in 30 day mortality nor in 1-year mortality rates.
Discussion
All modifiable causes for deep SSI, such as hematomas, should be prevented in acute hip fracture surgery. Since antithrombotics are associated with hematomas, an optimal handling in perioperative setting is necessary.
Conclusion
VKA was associated with longer time to surgery, more hematomas, and longer admission duration. VKA and AP were associated with more packed cell supplementation.
Introduction
Characteristic for frail hip fracture patients is the presence of multiple comorbidities. Amongst these comorbidities, cardiovascular disease has a high prevalence. 1 As a consequence of this, 40% of the patients with a hip fracture use antithrombotics, such as vitamin K antagonists (VKA) or antiplatelet therapy (AP) such as carbasalate calcium (CC) and acetylsalicylic acid (AA). 2 The use of these antithrombotics causes a conflict between optimal treatment of cardiovascular diseases and current guidelines for hip fracture surgery. 3 These guidelines advise to perform hip fracture surgery within 24 to 48 hours after admission, minimizing postoperative complications and mortality risk and establishing a higher percentage of patients returning to independent living.1,4-7
With a natural half-life over 24 hours, the use of VKA is challenging in daily practice when aiming for early surgery as is advised by current guidelines. 3 The use of VKA is associated with a higher amount of blood loss during surgery. 8 Reversal therapy of VKA with either vitamin K or prothrombin complex concentrate (PCC) is therefore embedded in the standard of care for patients with a hip fracture. 3 With reversal therapy, physicians aim for an International Normalized Ratio (INR) <1.5 to be able to administrate spinal anesthesia and to prevent bleeding complications.1,8-10 Current guidelines however see no harm in continuing AP such as CC and AA during the perioperative period. 3 Previously published studies however showed mixed results for bleeding complications and mortality for patients using AP.11-14
Despite treating patients conform current guidelines, major complications such as deep surgical site infections (SSIs) still occur in daily practice. The development of a SSI is influenced by the occurrence of a postoperative hematoma. 15 Since antithrombotic use is associated with postoperative hematoma, optimal handling of widely implemented antithrombotic in perioperative setting is necessary. 1 Question is whether current guidelines are optimal for this cause and are therefore optimal to prevent bleeding complications. 3 The aim of this study is therefore to investigate the influence of antithrombotics on clinical outcomes as postoperative hematomas and SSI after hip hemiarthroplasty when patients are treated according to current guidelines.
Materials and Methods
Patient Selection
For this observational cohort study, all consecutively admitted patients between January 1, 2010, and May 16, 2016, in two level II trauma teaching hospitals located in Rotterdam, the Netherlands, were screened for eligibility. Patients were enrolled in case of a femoral neck fracture for which a hip hemiarthroplasty was placed. Also, accurate information regarding antithrombotic use (ie, an up-to-date medication lists or information provided by pharmacy or general practitioner) had to be available. All other proximal femur fractures, that is, intertrochanteric fractures and subtrochanteric fractures, were excluded.
Perioperative Variables
Baseline characteristics including age, gender, preoperative hemoglobin (Hb) level in mmol/L, preoperative glomerular filtration rate (GFR) in mL/min/1.73 m2, and body mass index (BMI) in kg/m2 were extracted from patients’ medical charts. The American Society of Anesthesiologist (ASA) score was used to provide insight into the extent of comorbidities of a patient. Frailty was assessed using the Nottingham Hip Fracture Score (NHFS). 5 The NHFS is based on age, gender, serum hemoglobin at admission, cognitive dysfunction, number of comorbidities, institutionalization prior to admission, and presence of a malignancy in medical history and estimates the risk of 30-day mortality after a proximal femur fracture. 5 Time to surgery was measured in hours between admission and start of surgery. Surgical perioperative conditions were standardized according to local hospital protocol. An INR ≤1.5 was requested to administrate spinal anesthesia. Ten milligrams of vitamin K were administered to patients with an INR >1.5. This was repeated after 6 hours if INR was still >1.5. If patients responded insufficient to vitamin K, PCC was administered. No tranexamic acid or antiplatelet transfusion was used. All operating theaters had laminar airflow and all patients received standard antibiotic prophylaxis prior to surgery (1–3 g cefazolin, Kefzol). A cemented (Palamed G, gentamicin impregnated cement; Heraeus, Hanau, Germany) unipolar prosthesis (Mathys CCA; Mathys Ltd. Bettlach, Switzerland) was used in all surgeries. Surgeries were performed by senior trauma surgeons or directly supervised by senior trauma surgeons. The desired surgical approach, which was either an (minimally invasive) anterolateral approach or a straight lateral approach, was determined by the performing or supervising senior trauma surgeon. Besides the estimated blood loss (in mL) noted in patients’ charts, Δ hemoglobin was used as a proxy of perioperative blood loss. Δ hemoglobin was defined as the difference between the preoperative hemoglobin level and the lowest hemoglobin level postoperative (in mmol/L). The visual analogue scale (VAS) was used to rate the pain on the first postoperative day. Postoperative hematomas were diagnosed by physical examination, when a blue/purple discoloration and swelling of the skin surrounding the incision was used as a clinical definition. Postoperative wound infections were also diagnosed by physical examination, based on the classification system of the United States Centers for Disease Control and Prevention (CDC criteria). 16 Admission duration was defined as days from admission till discharge. Follow-up was done at the outpatient clinic with a minimum follow-up duration of 1 year.
Statistical Analysis
Data was analyzed using Stata version 14.0 (StataCorp, College Station, Texas). Categorical variables are presented as frequencies and percentages, and continuous variables are presented as means with a standard deviation (SD) in case of a normal distribution, or as median with an interquartile range (IQR) in case of a skewed distribution. All statistical tests were 2-sided with a significance level of 5%, P ≤ .05. As a consequence of the observational design of this study, no adjustments for confounders were made and missing data were not completed using imputation. Baseline characteristics, perioperative variables, and outcome variables are presented for 3 groups: patients without antithrombotics, patients using VKA, and patients using AP (CC and AA). A multivariable logistic regression analysis was performed for factors associated with hematoma accumulation. 17 Variables associated with hematoma accumulation were identified using previous literature and were included in multivariable analysis. In order to avoid multicollinearity, factors directly correlated were combined as a single variable in multivariable analysis.
Results
In total, n = 2491 patients were screened for eligibility of which n = 907 patients were enrolled in the study (Figure 1). Of these patients, n = 492 used no antithrombotics, n = 142 used VKA, and n = 213 used AP. Baseline characteristics are presented in Table 1. The median age was 84 years (78–88), n = 615 were female (68%), and 56% of the patients had an ASA score of ≥3. Patients using VKA were compared to AP (CC and AA) as well as to patients who did not use antithrombotics. Patients using AP were significantly older than patients without antithrombotics (84 years (79–88) vs 83 years (76–88), P = .03). No differences in age were present when VKA was compared to AP or to no antithrombotics. Patients using AP were less frequently female compared to no antithrombotics (62% vs 72%, P = .007). No differences in gender were present when VKA was compared to AP or to no antithrombotics. Patients using AP had a higher NHFS compared to patients without antithrombotics. No differences in NHFS were present when VKA was compared to AP or to no antithrombotics. Higher ASA score of 3–4 was more frequently present in patients using VKA compared to either no antithrombotics or AP (75% vs 46%, P < .001, and 75% vs 61%, P = .005, respectively). Patients using AP had more frequently higher ASA scores of 3–4 when compared to no antithrombotics (61% vs 46%, P <.001). Preoperative hemoglobin showed no differences between the 3 groups. GFR was significantly lower in patients using VKA compared to no antithrombotics (58 (52–77) mL/min/1.73 m2 vs 73 (56–90) mL/min/1.73 m2, P <.001) as well as compared to AP (58 (52–77) mL/min/1.73 m2 vs 69 (46–89) mL/min/1.73 m2, P = .01). Patients using AP had significantly lower GFR compared to no antithrombotics (69 (46–89) mL/min/1.73 m2 vs 73 (56–90) mL/min/1.73 m2, P = .04). No differences in BMI were present between groups. Flowchart of patient inclusion. Baseline Characteristics of Patients Using No Antithrombotic Drugs, Vitamin K Antagonists, and Antiplatelet Therapy. Abbreviations: ASA, American Society of Anesthesiology; BMI, body mass index in kg/m2; GFR, glomerular filtration rate in ml/min/1.73 m2; Hb, hemoglobin in mmol/L; IQR, interquartile range; NHFS, Nottingham Hip Fracture Score; SD, standard deviation. Group 1: no antithrombotic drugs. Group 2: vitamin K antagonists. Group 3: antiplatelet (carbasalate calcium and acetylsalicylic acid) therapy. aPearson’s chi-squared test. ₸ Student’s t-test, ¥ Wilcoxon rank-sum test.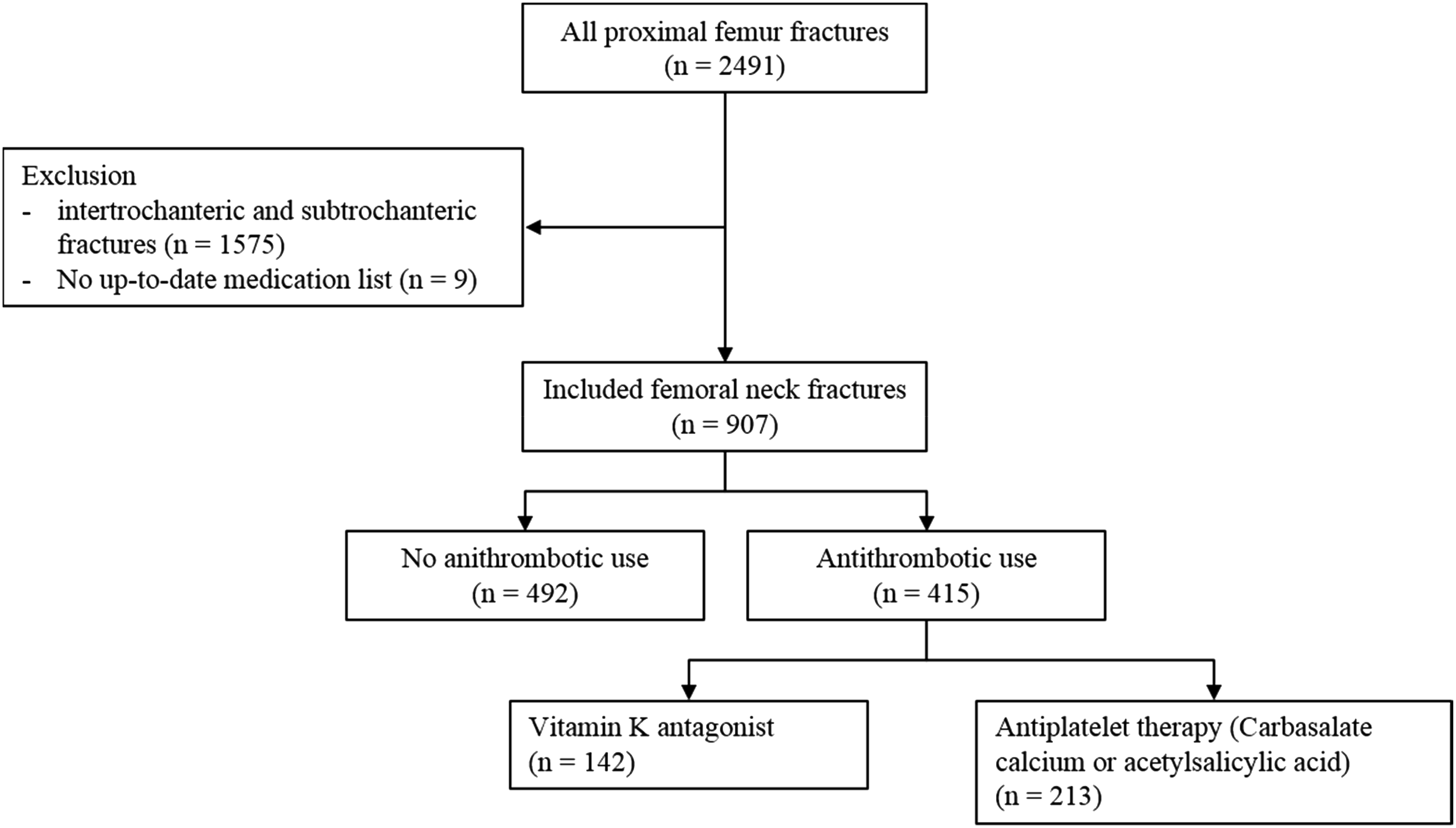

At admission, mean INR for patients using VKA was 3.2 ± 1.7. The mean preoperative INR for these patients was 1.5 ± .3 after correction. Correction was performed using vitamin K in 55% (n = 78) of the patients, and in 9% (n = 13) of the patients, additional PCC was needed besides vitamin K. In 8% (n = 11) of the patients who had correction of the INR, only PCC was used. Of the patients using VKA, 22% (n = 30) received no correction. Of these patients, 12 had an INR ≤1.5 (1.2 ± .2) at admission and 18 patients had an INR >1.5 (mean 2.1 ± .4). No complications occurred in the last group. Two patients with an INR >1.5 who did not receive correction had general anesthesia during surgery.
Perioperative Variables of Patients Using No Antithrombotic Drugs vs Vitamin K Antagonists and Antiplatelet Therapy.

Abbreviations: ASA, American Society of Anesthesiology; BMI, body mass index in kg/m2; GFR, glomerular filtration rate in ml/min/1.73 m2; Hb, hemoglobin in mmol/L; IQR, interquartile range; NHFS, Nottingham Hip Fracture Score; SD, standard deviation.
Group 1: no antithrombotic drugs. Group 2: vitamin K antagonists. Group 3: antiplatelet (carbasalate calcium and acetylsalicylic acid) therapy.
aPearson’s chi-squared test.
bKruskal–Wallis.
¥ Wilcoxon rank-sum test.
Clinical Outcomes of Patients Using No Antithrombotic Drugs vs Vitamin K Antagonists and Antiplatelet Therapy.

Abbreviations: ASA, American Society of Anesthesiology; BMI, body mass index in kg/m2; GFR, glomerular filtration rate in ml/min/1.73 m2; Hb, hemoglobin in mmol/L; IQR, interquartile range; NHFS, Nottingham Hip Fracture Score; SD, standard deviation.
Group 1: no antithrombotic drugs. Group 2: vitamin K antagonists. Group 3: antiplatelet (carbasalate calcium and acetylsalicylic acid) therapy.
aPearson’s chi-squared test.
bKruskal–Wallis.
Multivariable Analysis Hematoma.

Discussion
To prevent potential devastating complications after hip hemiarthroplasties such as deep SSIs, all preventable causes for deep SSI should be reduced. 15 Previous studies showed that hematomas are a cause of deep SSI. 15 Antithrombotic use is associated with hematoma accumulation, and therefore, optimal handling of widely implemented antithrombotic in perioperative setting is necessary. 8 Question is whether current guidelines are optimal for this cause since deep SSIs still occur in 5% of the geriatric hip fracture patients after hip hemiarthroplasty and hematomas occur in 15% of these patients. 15 This current study describes the effect of traditional antithrombotics on clinical outcome of geriatric patients with a femoral neck fracture for which a hip hemiarthroplasty was placed when patients are treated according to current guidelines.6,7
The finding with the most extensive clinical impact was a prolonged time to surgery in patients using VKA compared to both patients using AP and no antithrombotics (24 (19–37) hours vs 19 (13–25) hours, P < .001, and 24 (19–37) hours vs 20 (13–25) hours, P < .001, respectively). Prolonged time to surgery is associated with higher 30-day mortality rates, higher percentage of patients being discharged to an institution, and more frequently occurrence of postoperative complications as pneumonia, myocardial infarction, or pulmonary embolism.1,4,18,19 Conform current guidelines patients should be operated within 48 hours after admission.6,7 The median time to surgery in the study population was 20 (15–27) hours. However, a significant delay in time to surgery was found for patients using VKA despite aggressive correction of INR with either vitamin K or PCC. To quickly correct VKA, vitamin K was used in 55% of the patients using a VKA.1,3 Correction of INR is desirable for the use of spinal anesthesia and hemostasis during surgery. 20 Prolonged time to surgery for patients using VKA was previously found in studies by Lawrence et al and Tran et al. These studies describe that after controlling for baseline variables, VKA was associated with increased time to surgery.1,8,21 In these studies, the delay was not due to failure of INR reversal but due to the hospital’s capacity issues regarding availability of the surgical theater to perform hip repair surgery. Another explanation for the delay in surgery for patients using VKA is the indication for which patients use VKA.21,22 The most common indications for VKA are atrial fibrillation, thromboembolic disease, and mechanical heart valves.21,22 These conditions may delay surgery since more time is needed to appropriately investigate and optimize patients with these conditions before administration of anesthesia. 21
Hematomas occurred more frequently if patients used VKA compared to no antithrombotics (23% vs 11%, P = .001). No differences in occurrence of hematoma were present when VKA was compared to no antithrombotics or when AP was compared to no antithrombotics. One explanation of the increased risk for hematoma is the short half-life of vitamin K as reversal therapy for VKA. Combining the half-life of vitamin K (ie, 25 hours in elderly patients) with the time to surgery (ie, 24 hours (19–37) for patients using VKA), a rebound effect within the postoperative period can occur. 9 Since hematomas show significant association with deep SSIs, precautions should be taken to prevent these hematomas from developing. 15 Adequate correction and prolonged monitoring of INR with bridging therapy to prevent new cardiovascular events is one of those precautions. To assess the role of VKA in hematoma accumulation more specifically, a multivariable logistic regression was performed. Multicollinearity was found between VKA, Δ hemoglobin, and packed cell supplementation. These variables were therefore combined into a new variable and assessed in multivariable logistic regression analysis, which showed significant association with hematoma accumulation (OR 2.12, P = .001).
Admission duration was longer when VKA was compared to AP and to no antithrombotics (9 (7–12) days vs 7 (5–11) days, P < .001, and 9 (7–12) days vs 7 (5–9) days, P < .001, respectively). No differences in admission duration were found when AP was compared to no antithrombotics. No differences were found in the use of wound drains and the days until a drain was removed, which could therefore not be the explanation for the prolonged time to be ready for discharge. One variable that could be an explanation is that more packed cells were supplemented postoperative in patients using VKA, which could have prolonged hospital stay. 23 Patients using VKA received more packed cell supplementation than patients without use of antithrombotics (.4 ± 1.1 units vs .2 ± .6 units, P < .001). Patients using AP also received more packed cell supplementation compared to no antithrombotics (.3 ± .8 units vs .2 ± .6 units, P = .03). No differences in packed cell supplementation were present when VKA was compared to AP. The increased packed cell supplementation found in VKA and AP could be explained if increased perioperative blood loss was found. In this study however, no increase in perioperative blood loss or in Δ hemoglobin was found between groups. Previous studies showed that AP was not associated with more packed cell supplementation even though antithrombotic drugs are generally associated with more perioperative blood loss.24,25 Elderly patients however are particularly vulnerable to perioperative blood loss and postoperative anemia due to presence of comorbidities and limited physiological reserve. 26 Therefore, the threshold to supplement packed cells is lower in frail geriatric hip fracture patients than in healthy patients. 26 This combined with the borderline normal hemoglobin (overall 8.0 ± 1.0 mmol/L) could explain the increased packed cell supplementation found for patients with VKA and AP use.
Strengths and Limitations
The aim of this study was not to assess potential causality between antithrombotic use and undesirable clinical outcomes after hip fracture surgery but to evaluate daily practice of hip fracture surgery regarding antithrombotics. This study therefore has an observational character and no interventions were done. This was also the reason to choose not to impute missing data. We excluded patients who were unable to provide accurate information regarding antithrombotic use. This could however have induced selection bias since patients who cannot provide this information are potentially also patients with insufficient general practitioner contact and could therefore be the more frail patients presented in this study population. We believe this bias to be reduced to a minimum since in the Netherlands, the most frail patients frequently are institutionalized and accurate medication information can be provided by these institutions. There is also a risk of confounding by indication. Patients using AP may be more comorbid than patients using VKA since AP most frequently is prescribed for patients with a prior myocardial infarction for which a stent is placed or cerebrovascular event. VKA on the other hand is prescribed for patients with atrial fibrillation, thromboembolic disease, and mechanical heart valves. Despite differences in indication for the groups of antithrombotics in this study, no differences in 30-day mortality rates or 1-year mortality rates were found. We believe that the results of this study present an accurate image of the effects of antithrombotics in daily practice since very limited exclusion criteria were applied on the study population.
Conclusion
When geriatric hip fracture patients are treated according to current guidelines regarding anticoagulation use, differences in clinical outcomes between types of antithrombotics still occur. Patients using VKA or AP received more frequently packed cell supplementation postoperative compared to patients without antithrombotics. Also, patients using VKA developed hematomas more frequently. Collinearity was found between VKA use, Δ hemoglobin, and packed cell supplementation. These 3 variables combined showed significant association with more frequently occurring postoperative hematoma. Also, admission duration was longer for VKA compared to AP and to patients without antithrombotics. Despite higher ASA score of 3 and 4 in patients with VKA and AP, no differences in 30-day mortality or 1-year mortality were found. Also, despite quick and aggressive correction of INR, patients still had prolonged time to surgery. Quick and aggressive correction of INR should nevertheless remain one of the primary points of interest in optimizing preoperative care of frail geriatric hip fracture patients to prevent prolonged time to surgery, as well as the development of postoperative hematomas.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The local Medical Research Ethics Committee (METC) (Maasstad Hospital, Rotterdam, the Netherlands) has approved the study (reference number 2011/19). All protocols were in compliance with the declaration of Helsinki. Due to high incidence of cognitive dysfunction and no changes were made to the standard practice of care for the study population, the local METC has decided that patients’ consent to review their medical charts was not required.