
Abstract
Purpose: Patients with acute hip fractures who are on maintenance warfarin for anticoagulation present a significant challenge and their management remains controversial. The purpose of this study was to assess thromboembolic and systemic complications associated with pharmacological reversal of warfarin-associated coagulopathy in a population of geriatric patients with hip fractures. Methods: This retrospective cohort study identified patients with operative hip fractures on oral warfarin therapy who had an international normalized ratio (INR) >1.50 on admission (N = 93) approximately over a 13-year span. The control group consisted of patients whose warfarin was held upon admission without further intervention preoperatively (n = 23). The treatment group consisted of patients who underwent pharmacologic reversal of elevated INR with vitamin K and/or fresh frozen plasma (FFP) in addition to holding warfarin (n = 70). Primary outcomes included thromboembolic and other complications as well as mortality within 3 months of presentation. Time to surgery was a secondary outcome. Results: The 3-month mortality rate was 4% in the pharmacological intervention group and 17% in the watch-and-wait group; this difference trended toward statistical significance (P = .06). There were no significant differences in the likelihoods of other thromboembolic or nonthromboembolic complications between groups. While the difference in mean time to surgery was not significantly different overall between groups, this difference was significant in a subgroup of patients with higher baseline INRs (n = 46, INR >2.17), with a mean difference of 4.0 fewer days until surgery in the pharmacological intervention group (P < .01). Conclusions: Pharmacological reversal of warfarin-associated coagulopathy with a combination of vitamin K and FFP appears to be a safe way to optimize patients for operative fixation of hip fractures and is associated with a shorter delay to surgery in patients with more elevated INRs preoperatively. Level of evidence: retrospective cohort study (level III).
Introduction
Warfarin is the most frequently prescribed anticoagulant in the United States, and patients may take warfarin for a variety of reasons including atrial fibrillation, history of deep venous thrombosis (DVT) or pulmonary embolism (PE), history of valve replacement, and various hypercoagulable states, among other reasons. Recent estimates reveal that approximately 1% to 1.5% of the general population take chronic warfarin therapy as a prophylaxis against thrombosis, 1 which is likely an even higher percentage in the elderly population of patients sustaining hip fractures given the association of atrial fibrillation with age. In fact, patients with hip fractures using warfarin therapy for anticoagulation present a significant challenge to the orthopedic surgeon. While studies have shown improved results and less perioperative morbidity with rapid surgical intervention for hip fractures, surgery in this subset of patients is often delayed until reversal of anticoagulation in order to safely perform regional anesthesia and/or to avoid excessive bleeding during surgery. Published recommendations state that unless there is a very high risk of thromboembolism, anticoagulation should be temporarily discontinued in preparation for surgery. 2 Patients with elevated international normalized ratio (INR) are considered at higher risk during surgery because of increased bleeding complications. 3–7 Furthermore, there is a risk of epidural hematoma in patients receiving spinal or epidural anesthesia with elevated INRs, often necessitating either reversal of warfarin-associated coagulopathy in patients receiving regional anesthesia or abandoning regional anesthesia altogether and its associated advantages over general anesthesia. 8,9 An alternative to waiting for the INR to decrease with time is to administer pharmacological reversal with a combination of vitamin K or fresh frozen plasma (FFP). 10–12 There is some evidence, however, that overly aggressive pharmacologic reversal of supratherapeutic INR may further increase the risk of thromboembolic complications such as DVT or PE in this patient population which is already at elevated risk of such complications. 13–17
This retrospective study assessed a well-defined cohort of geriatric patients on warfarin presenting acutely to our institution over approximately a 13-year period for operative intervention of a hip fracture. The hypothesis was that patients on warfarin anticoagulation therapy who present with acute hip fractures would not have a higher rate of thromboembolic complications nor a higher 3-month mortality rate when receiving pharmacological reversal of their anticoagulation versus patients who simply have their warfarin held as a means of reversing elevated INR prior to surgery in this high-risk patient cohort. Our secondary hypothesis was that patients treated with pharmacological reversal would have a shorter time to surgery.
Patients and Methods
Patients
This was a retrospective cohort study of patients who were admitted with a primary diagnosis of a hip fracture. Inclusion criteria for this study included (1) patients who underwent surgical intervention of an acute hip fracture at Columbia Presbyterian Medical Center (CPMC) from January 1, 1997 through March 30, 2010, who were concurrently taking oral warfarin therapy at the time of admission and (2) patients having an INR value preoperatively greater than 1.50. This cutoff value of INR was chosen given the American Society for Regional Anesthesia and Pain Medicine (ARSA) recommendations that INR be less than 1.50 in surgical patients being managed with regional anesthesia because of the risk of epidural hematoma 9 ; this guideline is followed at the study institution, as attempts are typically made to perform spinal anesthesia in patients with hip fracture, given the demonstrated benefits of perioperative pulmonary function, decreased intraoperative blood loss, and blunting of the surgical stress response overall. 18,19 Fractures were defined by Current Procedural Terminology (CPT) codes, and these corresponded to OTA types 31-A, -B, and -C. 18 Exclusion criteria included (1) patients who were admitted with a hip fracture but who underwent nonoperative management or (2) patients who had a total hip arthroplasty for arthritis rather than for a femoral neck fracture.
Among 1634 patients presenting to CPMC from 1997 to 2010, who underwent operative intervention of a hip fracture, 93 patients (5.7%) were identified as having a preoperative INR >1.50 and were on warfarin on admission. Two study groups comprised the study population. The control (watch-and-wait) group consisted of patients whose warfarin was held upon admission without any further preoperative intervention (n = 23). The treatment (pharmacological intervention) group consisted of patients who underwent pharmacologic reversal of elevated INR (with vitamin K and/or FFP) in addition to their warfarin being held (n = 70). The 2 groups did not significantly differ in their demographics or in their preoperative American Society of Anesthesiologists (ASA) scores (Table 1 ), a factor that has been closely linked to the risk of postoperative mortality in the population with hip fracture. 20
Demographic Variables by Group a

Abbreviations: INR, international normalized ratio; SD, standard deviation.
a Data reported as mean (SD) or count (percentage).
Outcomes Measurements
Data were collected on first INR value at admission and INR just prior to surgery. Data were also collected on methods of pharmacological reversal of coagulopathy when performed, including dose and route of vitamin K (oral, subcutaneous, intravenous [IV], and/or intramuscular) and dose of FFP. Primary outcomes of interest included relevant thromboembolic complications, including DVT (as assessed by lower extremity venous Doppler or computerized tomogram angiography) and PE (as assessed by computerized tomogram angiography, VQ scan, transthoracic echocardiogram, or a clinical diagnosis by a cardiologist, internist, or hematologist) within 3 months of presentation/fracture occurrence. Nonthromboembolic complications were also collected, including myocardial infarction ([MI] as assessed by cardiac enzymes and echocardiogram), stroke (as assessed by computerized tomography of the head or magnetic resonance imaging of the brain), postoperative anemia requiring blood transfusion, hematoma and other wound complications, any condition requiring postoperative transfer to intensive care unit (such as pulmonary edema from volume overload), mortality, any complication requiring reoperation, and any complications overall within 3 months of presentation. These complications were assessed as part of the standard of clinical care, and screening tests were not performed in asymptomatic individuals. A secondary outcome of interest was time to surgery. All of the data analyzed in this study were previously collected as standard of clinical care. No novel prospective data were collected.
This research protocol was reviewed by the Institutional Review Board of CPMC, and a Health Insurance Portability and Accountability Act (HIPAA) Waiver of Consent was approved for this retrospective protocol.
Statistical Analysis
To compare postoperative thromboembolic events and complications (eg, DVT, PE, MI, stroke, mortality, postoperative intensive care unit (ICU) transfer, reoperation, hematoma, or other wound complication) that occurred with scarcity (defined by at least once cell count of less than five) between groups, Fisher exact test was employed. For events that were not rare (eg, for postoperative anemia requiring transfusion and any complication), chi-square test was utilized. Additionally, multivariate logistic regression models were created for the outcomes of mortality and any complication overall, since the frequency of these 2 adverse events was sufficiently large to allow for multivariate regression modeling. International normalized ratio at admission was dichotomized such that the values of INR at admission above the median value (INR = 2.17) were classified as “high INR” and those less than or equal to the median value were classified as “low INR.” The Wilcoxon rank sum test was used to compare the time to surgery between groups for each of the subgroups with low and high INR.
The analyses were conducted using SAS version 9.2. All P values were 2-sided and a P value of ≤.05 was considered statistically significant.
Results
Baseline Characteristics
All 93 patients identified by the inclusion and exclusion criteria were available for study by review of existing medical records. Patients were on average 81.4 years of age (standard deviation [SD] = 9.3, range = 54-100). The majority of patients sustained femoral neck or intertrochanteric femur fractures (Table 1). The watch-and-wait group had a mean INR of 1.9 (SD = 0.7) on admission, and the pharmacological intervention group had a mean INR of 2.6 (SD = 1.1), a difference which was statistically different (P < .01; Table 1). There was, however, no difference in the mean INR just prior to surgery (P = .91).
Among the 70 patients receiving pharmacological intervention, 46 received vitamin K alone, 11 received FFP alone, and 13 received both vitamin K and FFP. Among the patients receiving any form of vitamin K, the average total preoperative dose per patient was 4.2 mg of oral vitamin K (SD = 4.37), 1.4 mg of subcutaneous vitamin K (SD = 4.2), 1.1 mg of IV vitamin K (SD = 2.4), and 3.0 mg of intramuscular vitamin K (SD = 6.4). Among those receiving FFP, the average total preoperative dose per patient was 4.6 units IV (SD = 2.4). The percentage change in INR from admission value to value just prior to surgery was 42.9% overall, with 26.9% and 48.2% INR reduction for the watch-and-wait and pharmacological intervention groups, respectively, down to a preoperative value of 1.3 for both groups.
Postoperative Complications
Overall, thromboembolic events were rare. The causes of the 7 mortalities included 3 acute cardiopulmonary arrests, 2 MIs, and 2 deaths due to sepsis and severe end-organ failure. Overall, there were numerous complications of any kind, with 15 in the watch-and-wait group and 52 in the pharmacological intervention group (Table 2 ). While there were several MIs and strokes, none of these were conclusively proven to be related to thrombosis, as these events can also be related to ischemia.
Postoperative Events by Group a
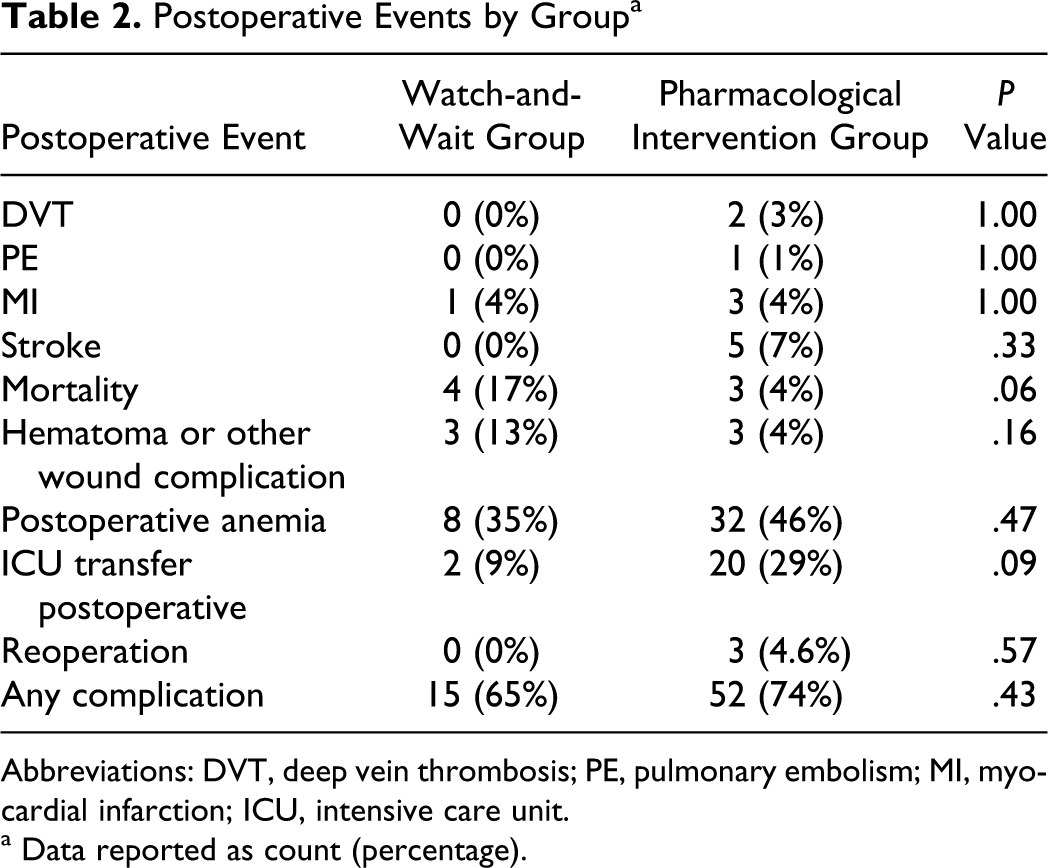
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism; MI, myocardial infarction; ICU, intensive care unit.
a Data reported as count (percentage).
Fisher exact test showed no significant association as a function of treatment group for the rare outcomes of DVT (P = 1.00), PE (P = 1.00), MI (P = 1.00), stroke (P = .33), hematoma or other wound complication (P = .16), postoperative ICU transfer (P = .09), or complication requiring reoperation (P = .57). A trend toward decreased mortality was seen in the pharmacological intervention group compared to the watch-and-wait group, as there was a 17% mortality rate in the watch-and-wait group versus 4% in the pharmacological intervention group (P = .06). Chi-square test showed no significant association as a function of treatment group for the outcomes of postoperative anemia requiring transfusion (P = .47) or any complication (P = .43).
Controlling for INR at admission, multivariate logistic regression analysis showed no significant difference between groups for any complication (P = .49) and for mortality (P = .60).
Time to Surgery
Overall, a nonparametric test of time to surgery in days showed no significant difference in time between the control and treatment groups (P = .89). International normalized ratio at admission was then dichotomized such that the values of INR at admission above the median value of 2.17 were classified as high INR and those less than or equal to the median value were classified as low INR (Table 3 ). Wilcoxon rank sum test revealed a highly significant increased time to surgery in those with a high INR (P < .01) but not for those with a low INR (P = .26); among those with a high INR, patients in the watch-and-wait group had a mean time to surgery of 6.8 days (SD = 1.9) and those in the treatment group had a mean time to surgery of 2.8 days (SD = 1.3).
Delay to Surgery by Group and Preoperative INR a
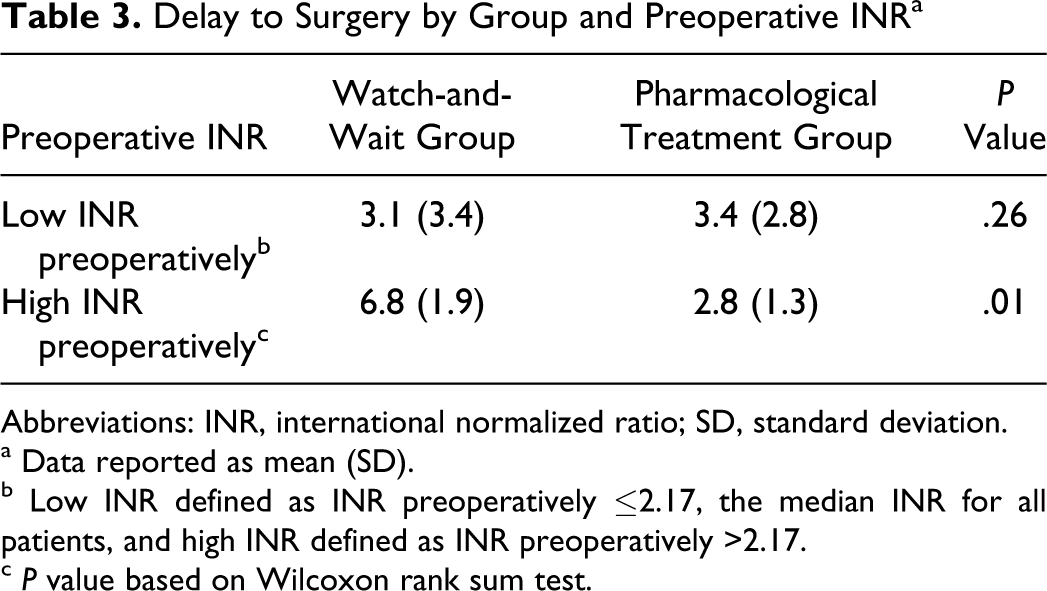
Abbreviations: INR, international normalized ratio; SD, standard deviation.
a Data reported as mean (SD).
b Low INR defined as INR preoperatively ≤2.17, the median INR for all patients, and high INR defined as INR preoperatively >2.17.
c P value based on Wilcoxon rank sum test.
Discussion
Warfarin-associated coagulopathy is a condition which presents a unique challenge to surgeons treating patients requiring urgent surgery, as highlighted by a recent review published by the American Academy of Orthopaedic Surgeons. 12 One option in preparing patients for surgery—holding warfarin administration until the INR values are deemed acceptably low—results in a slow reversal of INR, although largely maintaining an exponential decline. 21–23 Waiting several days for INR to decrease, however, may compromise the benefits of early operative fixation of patients with hip fractures.
An alternative option to holding warfarin for several days in preparing such patients for surgery is pharmacological reversal of warfarin-associated coagulopathy with vitamin K, FFP, or prothrombin complex concentrates (PCCs). Since the 1950s, vitamin K in its various forms has proven to be an effective INR reversal agent in the presence of warfarin-associated coagulopathy. 22 While oral, subcutaneous, or IV vitamin K may be administered to correct elevated INRs, the efficacy and associated complications vary for each route. Studies have revealed that oral and IV vitamin K are more effective in their ability to achieve target INR than subcutaneous vitamin K. 24–26,46 Furthermore, IV vitamin K provides the most rapid correction of INR, although this route of administration is more frequently associated with overcorrection of INR and is also rarely associated with fatal anaphylaxis. 27–29 Riegert-Johnson and Volcheck estimated the incidence of anaphylaxis to IV phytonadione to be 3 per 10 000 doses, which is comparable or slightly less than other drugs known to cause anaphylaxis. 29
Fresh frozen plasma is an alternative to vitamin K for correcting coagulopathy, which may be administered to reverse the effects of warfarin. 30–35 Fresh frozen plasma is a human donor plasma that contains many plasma proteins, including all the coagulation factors, and has been the most widely utilized form of coagulation factor replacement. 36 However, because of the variable content of the vitamin K-dependent coagulation factors in FFP, especially factor IX, large volumes of fluid required, and the increased infection risks, the use of FFP for the emergency reversal of warfarin coagulopathy has been questioned. 30–32 Recently published evidence-based practice guidelines for FFP transfusion fail to recommend for or against transfusion to reverse warfarin coagulopathy in patients without intracranial hemorrhage, as the quality of evidence on both sides is very low. 33
Some evidence exists to suggest that overly aggressive pharmacologic reversal of supratherapeutic INRs may promote thromboembolic events and other complications. García-Noblejas et al reported a case of a PE in a patient with congenital factor V deficiency during treatment with FFP, despite coadministration of prophylactic low-molecular-weight heparin. 14 Other case reports have described patients receiving plasma exchange with FFP and developing venous thromboembolism. 15,16 Ratnaweera et al reported a case of multiple PE in a patient receiving vitamin K, FFP, and PCCs for warfarin coagulopathy in the presence of an intracranial hemorrhage. 13 Additional in vivo and in vitro data support the hypothesis that PCCs may predispose patients to thromboembolic events. 17,37 Despite published guidelines on the use of vitamin K, FFP, and PCCs, including their simultaneous use, it remains unclear how to best manage the warfarin-anticoagulated patient requiring urgent surgery and there continues to be a dearth of literature quantifying the effects of pharmacological reversal of supratherapeutic INR. 2,38–42 Guidelines set forth by Ansell and colleagues have specified a role for vitamin K and FFP used simultaneously, as was the case for many patients in the current study, in the presence of active bleeding and a supratherapeutic INR or if the bleeding risk is high with an INR greater than 9.0. 38 Given that the effect of FFP is short-lived, as the half-lives of the clotting factors are short, the coadministration of vitamin K is essential to sustaining a lower INR. Thakur and colleagues have recently advocated the simultaneous use of vitamin K and FFP in preparing patients on warfarin for urgent orthopedic surgery including patients with intertrochanteric fractures or femoral neck fractures, as vitamin K promotes new factor production while the effect of FFP is diminishing. 12
The current data in this study do in fact suggest that vitamin K and FFP administration appear to be safe pharmacological methods for reversal of warfarin-associated coagulopathy in a geriatric population of patients with operative hip fractures. Despite case reports of thromboembolic complications associated with vitamin K and FFP use, there was no greater occurrence of thromboembolic events or other postoperative complications in patients receiving pharmacological reversal with vitamin K and/or FFP versus those patients in whom warfarin was simply held until INR declined sufficiently in this population. In fact, there was a nearly significantly lower mortality rate in patients treated with pharmacological intervention compared to those treated with warfarin cessation alone, further supporting the safety profile of vitamin K and FFP, although this statistical trend must be interpreted with caution as it may be subject to beta error. Nonetheless, this trend was consistent with other reports that have supported early fracture fixation and mobilization in order to decrease perioperative morbidity in patients with hip fractures. 10,11 In an ideal system at a geriatric fracture center as discussed by Friedman et al, in which patients are rapidly assessed and optimized by geriatricians and orthopedic surgeons and undergo surgery early on, the time to surgery, overall complication rate, and length of stay are all diminished, compared with the usual care patients. 43 Furthermore, by actively reversing the INR with vitamin K and/or FFP, a greater percentage correction of the INR was achieved preoperatively and the time to surgery was nearly a day shorter overall. While this trend toward greater delay to surgery in patients in the watch-and-wait group was not significantly different among all patients, the mean difference of 4 days greater delay in surgery in the watch-and-wait group compared to those in the pharmacological intervention group was significantly greater in the subset of patients with high INR at admission (INR greater than the median value of 2.17).
Our results in a primarily geriatric hip fracture population are in concordance with the few previous studies in the literature that have compared series of patients treated with and without some type of pharmacological reversal of warfarin-induced coagulopathy. The most relevant study was performed by Tharmarajah and colleagues and was a combination of retrospective and prospective cohort study of 40 patients on warfarin with operative orthopedic trauma. 44 In all, 19 patients solely had their warfarin held and 21 patients were also given IV vitamin K. The authors found that vitamin K administration significantly reduced the time to surgery by almost half and reduced the INR to less than 2.0 in 74% of patients. There was no increased risk of complications associated with vitamin K administration, and there were no hemorrhagic or thromboembolic complications at 3-month follow-up. Similarly, Shields et al reported an approximately 2% adverse reaction rate to IV vitamin K for reversal of warfarin coagulopathy, including dyspnea and chest tightness, but none of the patients had associated thromboembolism after surgery. 45
There are several limitations to the present study. First as a retrospective cohort study, this is an effort to explore the already existing data, and the current investigation has a relatively small sample size to detect complications which may be rare, including DVT and PE. It is our intent that the hypotheses generated from this study will be further investigated in a larger scaled, randomized trial. Another limitation was that the doses of FFP and vitamin K as well as routes of administration varied among patients, and individual subgroup analysis among patients receiving only FFP or vitamin K was not possible, given the small number of patients in each category. This may, however, represent a practical situation as recommendations support the concurrent use of both vitamin K and FFP in urgent or emergent clinical settings, such as the scenario studied in the present investigation. 2,12,31,38 A further limitation was that there was a higher INR at the time of admission in those in the pharmacological treatment group, and these patients therefore may have had a difference at baseline, predisposing those in the treatment group to a different likelihood of complications than those in the control group; however, there were no significant differences in the INR just prior to surgery, likely minimizing this effect, and INR at admission was controlled for in the multivariate regression analysis. A further limitation was that the decision of which method of INR reversal individual patients received was often made by the patient’s surgeon who likely considered many patient factors, introducing a degree of selection bias. However, there were no differences in the mean ASA scores, which correlate highly with the risk of mortality in the hip fracture population, 20 nor the percentage of diabetic patients between groups. Closer inspection of patient charts may have also enabled detection of clinically significant yet not ICU level complications related to volume overload (such as pulmonary edema). Documentation of such complications is limited, however, due to the limited medical intervention needed to treat them, resulting in underestimation of the overall transfusion-related complication rate.
Despite these limitations, the current data suggest that reversal of warfarin-associated coagulopathy with vitamin K and/or FFP is not associated with a greater rate of postoperative complications in the high-risk geriatric population of patients with hip fractures and appears to be a safe alternative to warfarin cessation alone, which may result in increased delay to surgery. We urge cautious interpretation of these data, and we hope that this retrospective cohort study will serve as an initial step to better elucidate this poorly characterized clinical scenario in guiding future well-designed prospective, randomized investigations in a comprehensive system of care.
Footnotes
No author has a financial relationship with the provider of the grant. The authors have full control of all primary data and allow the journal to review our data if requested.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was supplied by the Orthopaedic Scientific Research Grant, New York, NY. 2009.