
Abstract
Objective:
There continues to be controversy over whether operative delay is necessary for patients on antiplatelet therapy, particularly for elderly patients with hip fractures. This study sought to assess current clinical practices of orthopedic surgeons regarding perioperative management of these patients.
Methods:
A 12-question, Web-based survey was distributed to orthopedic surgeons via e-mail. Questions regarding timing of surgery assumed patients were on antiplatelet therapy and assessed attitudes toward emergent and nonemergent orthopedic cases as well as operative delay for specific closed fracture types. Responses were compared using unpaired, 2-tailed Student t tests for continuous variables and Pearson chi-square tests with odds ratios (ORs) and 95% confidence intervals (CIs) for categorical variables. Statistical significance was defined as a P value <.05.
Results:
Overall 67 orthopedic surgeons responded. Fifty-two percent (n = 35) of the respondents described their practice as academic. Thirty-nine percent (n = 25) of the surgeons indicated that no delay was acceptable for urgent but nonemergent surgery, and 78% (n = 50) reported no delay for emergent surgery was acceptable. Sixty-eight percent (n = 46) of respondents felt patients on antiplatelet therapy with closed hip fractures did not require operative delay. Surgeons who opted for surgical delay in hip fractures were more likely to delay surgery in other lower extremity fracture types (OR = 16.4, 95% CI 4.48-60.61, P < .001). Sixty-four percent (n = 41) of the surgeons indicated there was no protocol in place at their institution.
Conclusions:
There continues to be wide variability among orthopedic surgeons with regard to management of patients with fracture on antiplatelet therapy. Over a quarter of surgeons continue to opt for surgical delay in patients with hip fracture. This survey highlights the need to formulate and better disseminate practice management guidelines for patients with fracture on antiplatelet therapy, particularly given the aging population in the United States.
Keywords
Introduction
As the population ages, an increasing number of patients are prescribed antiplatelet therapy (clopidogrel, aspirin, cilostazol, ticlopidine, dipyridamole, etc) for a variety of indications including cardiovascular disease, prevention of thrombotic events after drug-eluting stent placement, peripheral arterial disease, and secondary prevention of cerebrovascular ischemic events. 1,2 The potential increase in risk of perioperative bleeding associated with antiplatelet therapy must be balanced with the associated morbidity of delaying a necessary surgery. 3 A single dose of clopidogrel, for example, will affect platelets for the remainder of their life span with normal platelet function returning in concert with turnover of the cells between 5 days and 9 days. 4 As patients with cardiac comorbidities requiring these drugs are often similarly at risk for osteoporosis and thus for fragility fractures, this population presents a unique dilemma for orthopedic surgeons who perform emergent, urgent, as well as elective operations on these patients. 5 Additionally, a nationwide cohort study published in 2012 by Jørgensen et al concluded clopidogrel taken by itself in the recommended dose range is associated with a risk of fractures, although the in vivo effects of antiplatelet drugs on bone metabolism are uncertain. 5
Given these facts, the lack of well-established guidelines regarding the perioperative management of patients undergoing surgical intervention for orthopedic injuries who are on antiplatelet therapy is particularly concerning. 6 The potential morbidity associated with patients being taken off antiplatelet therapy must be weighed in these decisions as well, adding complexity to the dilemma. These decisions are encountered most frequently in the geriatric population and are particularly difficult in elderly patients who have sustained a hip fracture, given the established advantages of early surgery for these patients. 7
Differing recommendations have been made in the literature regarding management of patients with fracture on antiplatelet and anticoagulant therapy. However, recent studies are supportive of the safety and benefit of early surgery for patients with hip fracture on antiplatelet therapy. 6,8 –10 Previous surveys of orthopedic surgeons in the United Kingdom and of orthopedic program directors in the United States have demonstrated wide variation in practice patterns for these scenarios, with the last evaluation of practice patterns in the United States completed in 2008, to our knowledge. 6,11,12
This study sought to assess the current practice pattern among a sample of orthopedic surgeons in the United States regarding operative delay in perioperative management of patients on antiplatelet therapy. We also sought to discern whether differences in current management of this patient population with respect to fracture type existed and to evaluate evolving practices relative to those reported in the past surveys.
Methods
This study was approved by our home institution Internal Review Board. A 12-question Web-based survey was created (Table 1) and distributed to orthopedic surgeons registered with the Orthopaedic Trauma Association (OTA) through their Web-based survey registry and members of the American Academy of Orthopaedic Surgeons (AAOS) present at local academic conferences. As of 2015, the OTA lists 601 “active” members with a subset of 319 “clinical members” of which 72 are international members, leaving 247 OTA members eligible for this study. Respondents were considered eligible if they were currently practicing orthopedic surgeons in the United States and clinical members of the OTA. Regarding respondents at local conferences, approximately 200 or so additional orthopedic surgeons were asked to participate. Additional orthopedic surgeons approached were required to be actively practicing in the United States and active members of the AAOS to participate. Respondents were ultimately selected for inclusion based on the completion of all survey questions and meeting the aforementioned criteria.
Individual Survey Questions.
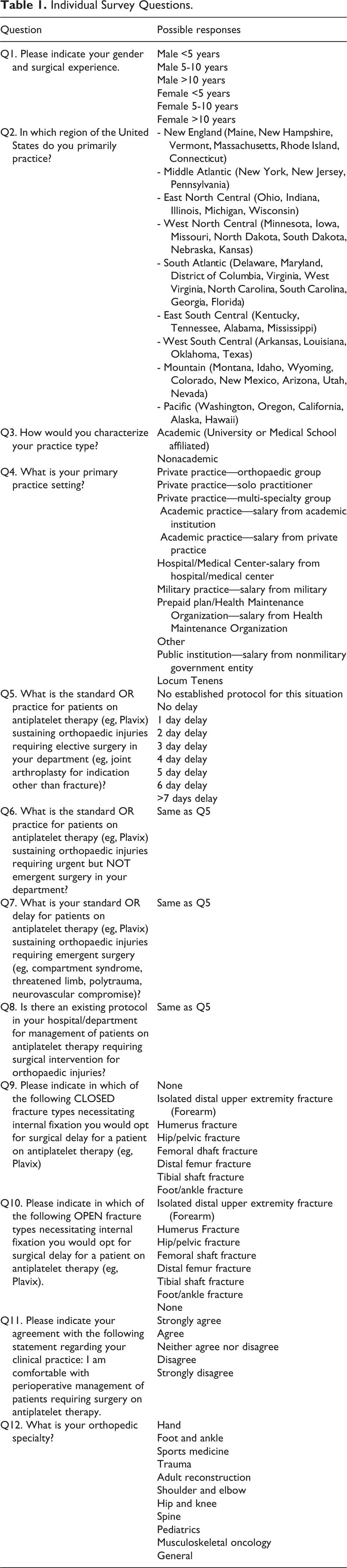
Questions regarding timing of surgery assessed management for patients on antiplatelet therapy in elective, urgent, and emergent fracture care situations. Survey items were selected based on questions in similar past surveys with additional questions specific to fracture location included so as to provide a temporal comparison with regard to management patterns. 6,11 Responses included various options for operative delay. Demographic information on physician gender, number of years of experience, primary practice setting, and regional location was collected. The question “Please indicate in which of the following closed fracture types necessitating internal fixation you would opt for surgical delay for a patient on antiplatelet therapy (eg, Plavix)” was included with the following answer choices: isolated distal upper extremity fracture, humerus fracture, hip fracture, femoral shaft fracture, distal femur fracture, tibial shaft fracture, foot/ankle fracture, and none. Responses were grouped dichotomously into upper extremity and lower extremity (without hip fractures included) for analysis.
Questions regarding practice patterns and protocols both from an individual practitioner and from an institutional perspective were included in the survey. It was recognized that the absence of an institutional protocol did not preclude an individual orthopedic surgeon having a decision-making process in place for these patients and also that, in the presence of a standardized protocol, practice patterns vary for an orthopedic surgeon on a case-by-case basis (Table 1, Questions 5-7).
Responses were compared using unpaired, 2-tailed Student t tests for continuous variables and Pearson chi-square tests with odds ratios (OR) and 95% confidence intervals (CI) for categorical variables. All statistical tests were carried out using SPSS software version 20.0 (SPSS Inc, Chicago, Illinois). P < .05 was considered significant for all analyses.
Results
A total of 67 of the approximate 500 orthopedic surgeons who were asked to participate were included in the analysis, of which 27% (n = 18) were fellowship-trained orthopedic traumatologists. Fifty-two percent (n = 35) of the respondents described their practice as academic. Regional variation in respondents was as follows: 75% Northeast, 10% West, 7.5% South, and 7.5% Midwest. Respondent demographics including specialty, specific practice type, and surgeon experience are listed in Table 2.
Survey Respondent Demographics.

Regarding management of any orthopedic injury requiring operative intervention, 39% (n = 25) of surgeons responded that no delay was acceptable for urgent but nonemergent surgery, and 78% (n = 50) of surgeons reported no delay for emergent surgery was acceptable. Of the surgeons who opted for delay in urgent surgery, 50% delayed surgery for 3 days or more (Figure 1). Sixty-eight percent (n = 46) of respondents felt closed hip fractures did not require operative delay. Surgeons who opted for surgical delay in hip fractures were more likely to delay surgery in other lower extremity fractures (OR = 16.4, 95% CI 4.48-60.61, P < .001; Figure 2) although not more likely to delay surgery in upper extremity fractures compared to their counterparts (P = .118). Positive responses to delay in hip fractures were compared separately from the lower extremity and upper extremity fracture categories. A positive response to delay in hip fractures was not considered a positive response to the “LE fractures” category, which was a compilation of individual questions for delay practices in various lower extremity fracture types. Sixty-four percent (n = 41) of surgeons indicated there was no protocol in place at their institution regarding the management of patients on antiplatelet therapy. The existence of a protocol policy at any individual respondent’s institution (Table 1, Question 8) had no impact on his or her likelihood to delay treatment of upper extremity (P = .68), lower extremity (P = .61), or isolated hip fractures (P = .53). There were no significant differences between traumatologists and nontraumatologists or between academic and nonacademic orthopedic surgeons with regard to practice patterns or protocol policies.

Distribution of survey responses to survey question: “What is the Standard OR practice for patients on antiplatelet therapy (eg, Plavix) sustaining orthopaedic injuries requiring urgent but NOT emergent surgery in your department?”

Orthopedic surgeons who delayed surgery in patients with closed hip fracture on antiplatelet therapy were more likely to delay surgery for other lower extremity (LE) fractures than those who opted for no surgical delay in patients with closed hip fracture (67% vs 11%, P < .001).
Discussion
Several surveys on this topic are available for comparison. Previous surveys of orthopedic clinicians in the United Kingdom and Scotland have shown wide variability in standards of practice regarding perioperative management of this patient population. 11 –13 A similar study conducted in 2008 surveying orthopedic residency program directors in the United States demonstrated a similar lack of consensus on this topic with 23% of orthopedic surgeons indicating no delay is necessary for nonemergent operative interventions for patients on Plavix, compared to 39% who responded in this manner for the current survey. 8 A comparable proportion of surgeons in this survey were in agreement regarding the acceptability of operating without delay on emergent orthopedic injuries (78% in this survey vs 89% previously).
A total of 31% of respondents indicated they would opt for surgical delay for hip fractures in patients on antiplatelet therapy. These survey responses were observed in the face of several recent clinical trials and cohort studies suggesting operating without delay on patients with hip fractures using clopidogrel is safe. 14 –17 A paucity of literature on the subject in regard to other fracture types and conflicting study results create significant barriers to establishing standard-of-care practices. This survey demonstrates wide variability in orthopedic surgeons’ preferences for surgical delay with regard to different fracture locations in patients on antiplatelet medications requiring operative intervention (Table 3). Opting for surgical delay in hip fractures appears to be correlated with doing so for other lower extremity fractures specifically. 18 –20 Academic and nonacademic surgeons in this survey did not have differing practice patterns, potentially reflective of the largely anecdotal and individualized nature in which orthopedic surgeons appear to devise management patterns in these patients. In addition, there were no differences in practice patterns by duration of practice.
Individual Fracture Type Operative Delay Responses: “Please indicate in which of the following closed fracture types necessitating internal fixation you would opt for surgical delay for a patient on antiplatelet therapy (eg, Plavix).”

This survey is limited by its relatively small sample size and its regional skew to the Northeast region. While this must be considered with regard to any generalizable conclusions about practice patterns, we felt that our respondents were reflective of the orthopedic community by and large, geography notwithstanding. We cannot speak to differences in management with respect to geographic location in the United States, since we did not attain enough responses from each region to draw meaningful conclusions.
The number of questions included in the survey was limited to allow ease of completion, which prevented collection of more in-depth information regarding surgeon practice in specific scenarios. For example, the use of pooled platelet transfusion was not addressed, despite recent recommendations in the literature that this should be a preoperative measure for consideration of patients on antiplatelet therapy requiring surgery for hip fractures. 21 This survey drew on community practitioners as well as academic orthopedic surgeons in contrast to previous surveys that targeted only academic practitioners or individuals answering on behalf of a hospital unit. This allowed for contrast between practice types and discernment of factors that may play a role in surgeon practices. The proportion of surgeons indicating no surgical delay is acceptable for emergent orthopedic injuries (78%) is similar to that reported in a previous survey. 6,12 Although the title of the survey referred to antiplatelet therapy, the questions within the survey made explicit references to “clopidogrel/Plavix.” In retrospect, this wording may have led to different interpretations of the patient population in question by respondents and influenced results of the survey. We believe that orthopedic surgeons interpreted these questions in a similar manner, and that our results are valid, though future surveys should unambiguously describe the precise patient population being investigated.
There have now been numerous studies suggesting delay is not necessary for patients receiving antiplatelet therapy undergoing hip fracture surgery as well as nonelective operative orthopedic procedures. 8,9,16,17,21,22 . Managibawala et al found no significant differences between patients with hip fracture on clopidogrel undergoing surgery versus patients with hip fracture not on clopidogrel undergoing surgery, although they were only able to identify 15 patients in their cohort on clopidogrel. 23
In an article by Gleason et al detailing the management of patients with hip fracture on antiplatelet therapy, no clear recommendations were made, given a lack of consensus on the topic. 4 Most recently, a systematic review, meta-analysis, and meta-regression by Doleman et al demonstrated no associated increase in overall mortality for patients with hip fracture on clopidogrel undergoing early surgery but also reported an associated increase in blood transfusion for these patients. This review also reported a decreased length of stay in early surgery versus delayed surgery patient groups, and concluded early surgery is safe for patients with hip fracture on clopidogrel. 24
Conclusion
This study is the first to explore the effect of fracture location on orthopedic surgeons’ decision-making patterns for patients on antiplatelet therapy. In addition, this study demonstrates that there continues to be divergent practice patterns and no consensus among orthopedic surgeons regarding management of patients with fracture on antiplatelet therapy since the last time a similar survey was conducted and published in 2008. Despite evidence in the literature suggesting that no surgical delay for patients with hip fracture on clopidogrel is acceptable and the benefits of early hip fracture surgery, over a quarter of surgeons continue to opt for surgical delay. 9,25 This propensity for surgical delay for patients with hip fracture appears to correlate with surgeons’ preferences for surgical delay in other lower extremity fracture types. A majority (63%) of surgeons in this survey endorsed having no protocol in place for these patients, highlighting the void that needs to be addressed for many practicing orthopedic surgeons. Controversy regarding this topic continues, and the need for large prospective studies on fracture patients treated with clopidogrel is readily apparent. 26 These findings should be used as evidence that establishment of guidelines for orthopedic surgeons managing these patients is critical, not only for patients with hip fracture but also for other patients with fracture on antiplatelet therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.