
Abstract
Introduction:
To analyze the perioperative hidden blood loss (HBL) and its influencing factors in elderly cervical spondylosis patients treated with anterior cervical discectomy fusion (ACDF).
Materials and Methods:
From January 2017 to December 2018, 128 elderly cervical spondylosis patients (age > 65 y) treated with ACDF were selected. The patients’ height, weight, duration of symptoms, previous medical history and other basic information were routinely recorded. The hemoglobin (Hb), hematocrit (Hct) and blood coagulation function preoperative and the next day postoperative were recorded. The operation time, surgical bleeding, ASA classification, fixation method, total drainage and the time for extraction of drainage tube were recorded. The total blood loss (TBL) was calculated according to the Gross’s formula, and HBL was calculated based on TBL, total drainage and surgical bleeding. The statistical analysis of HBL was performed, and then influential factors were further analyzed by multivariate linear regression analysis and t test.
Results:
The mean surgical bleeding was 102.70 ± 46.78 mL and HBL was 487.98 ± 255.96 mL. HBL accounted for 67.61 ± 5.20% of TBL. According to the multiple linear regression analysis, the gender (P = 0.047), operation time (P = 0.000), fixation method (P = 0.014) and international normalized ratio (INR) (P = 0.003) influenced the amount of HBL. Body mass index (BMI) (P = 0.624), hypertension (P = 0.977), diabetes (P = 0.528), blood type (P = 0.577), ASA classification (P = 0.711), duration of symptoms (P = 0.661), preoperative cobb angle (P = 0.152), number of surgical level (P = 0.709), intramedullary hyperintensity (P = 0.967), drainage time (P = 0.294), postoperative drainage volume (P = 0.599), prothrombin time (PT) (P = 0.674), activated partial thromboplastin time (APTT) (P = 0.544) and thrombin time (TT) (P = 0.680) had no correlation with the amount of HBL.
Conclusions:
There was obvious HBL during the perioperative period of ACDF in elderly cervical spondylosis patients. The male patients, longer operation time, fusion with titanium plate and cage and high INR were independent risk factors for HBL.
Keywords
Introduction
During the development of society, aging of the population and increased use of computer, the number of people with cervical spondylosis is increasing. 1 Cervical disc degeneration is the most common cause of cervical spondylotic radiculopathy and cervical spondylotic myelopathy. 2 The main symptoms are pain, numbness and weakness of both upper limbs which seriously affect quality of life and bring huge social and economic burden. 3 The consequence is more serious if the elderly patient has such disease. The occurrence of numbness and weakness in the lower limbs and other symptoms are prone to fall and lead to fracture, brain injury, and even life-threatening in elderly patients. Anterior cervical discectomy fusion (ACDF) has become the first choice for the treatment of cervical spondylosis if conservative treatment fails. However, the majority of elderly patients are accompanied with poor physical condition, multiple chronic diseases, and poor tolerance of blood loss. Long-term bed rest can also easily cause pneumonia, bedsores, thrombosis and other serious complications. It is often believed that blood loss during the intraoperative and postoperative of ACDF is limited but the patients’ postoperative hemoglobin showed marked decrease. 4 Postoperative anemia will result in slower functional recovery, longer wound healing time, increased risk of infection, longer hospital stays and increased financial burden. 5
Current studies found that there is a large amount of hidden blood loss (HBL) in spine surgery, 6,7 and the same situation also exists in minimally invasive surgery such as percutaneous kyphoplasty (PKP) surgery. 8,9 However, there are few studies focus on perioperative HBL in elderly ACDF patients. 4,10 Most spine surgeons also ignore HBL during the perioperative period because of the small incision of ACDF. However, we suspected that there are also high levels of HBL during the perioperative period of ACDF based on the results of previous studies.
In this study, we retrospectively analyzed the perioperative HBL in elderly ACDF patients and identified its influencing factors.
Materials and Methods
Patient Selection
The study protocol was reviewed and approved by the Ethics Committee of Clinical Medical College of XX University and all patients signed informed consent. A total of 128 elderly cervical spondylosis patients (78 males and 50 females) treated with ACDF under general anesthesia from January 2017 to December 2018 were retrospectively reviewed. All patients’ normal data including gender, weight, height, hypertension, diabetes, duration of symptoms, ASA classification, fixation method, operation time, surgical bleeding, hematocrit (Hct), hemoglobin (Hb), prothrombin time (PT), activated partial thromboplastin time (APTT), international normalized ratio (INR) and thrombin time (TT) preoperative and postoperative, total drainage and time for extraction of drainage tube were recorded. In addition, imaging data including the presence of intramedullary hyperintensity assessed by MRI and preoperative cobb angle measured by X-ray were also recorded.
Inclusion Criteria and Exclusion Criteria
Inclusion criteria: (1) diagnosis of cervical spondylotic radiculopathy or cervical spondylotic myelopathy; (2) no significant improvement after conservative treatment for 3 months; (3) follow-up more than 6 months; (4) without cervical surgery history; (5) the preoperative surgical plan is formulated and implemented by the same term; (6) age over 65 years.
Exclusion criteria: (1) cervical surgery history; (2) combined motor neuron disease; (3) cervical vertebra malformation, fracture, tumor or infection; (4) abnormal coagulation function; (5) blood loss for various reasons during and after operation >1.5 L; (6) severe complications occurred during perioperative period; (7) use of anticoagulant drugs before and after surgery; (8) incomplete case data.
Methods
Calculation of HBL
According to the records of patients’ gender, height, weight and other data, the patient s’ blood volume was calculated using the method reported by Nadler et al. 11 The formula was as following: Blood volume = k1 × height (m) 3 + k2 × weight (kg) + k3. For male patients: k1 = 0.3669, k2 = 0.03219, k3 = 0.6041; For female patients: k1 = 0.3561, k2 = 0.03308, k3 = 0.1833. The total blood loss (TBL) was calculated according to the formula reported by Gross. 12 HBL was calculated by TBL and the formula was as follow: TBL = blood volume × (preoperative Hct − postoperative Hct)/average (preoperative Hct + postoperative Hct). The formula used to estimate HBL: HBL = TBL + blood infused − surgical bleeding − volume of drainage.
Statistical Analysis
All data analysis was performed using the SPSS 21.0 software package (SPSS, Chicago, IL) and the statistical significance level was set at P < 0.05. All variables may be related to HBL were screened by single factor correlation analysis, including 12 quantitative variables (BMI, duration of symptoms, preoperative cobb angle, number of operation segments, surgical bleeding, operation time, postoperative drainage, PT, APTT, INR and TT) and 8 qualitative variables (gender, hypertension, diabetes, ASA classification, blood type, intramedullary hyperintensity, fixation method and drainage time). Then multiple linear regression analysis was used to select the variables with high correlation and determine the independent factors related to HBL.
Results
A total of 116 patients were followed up completely at least 1 year after surgery, and the complete follow-up rate was 90.6%. The other patients who were not followed up completely were followed up for more than 6 months. As shown in Table 1, the average height was 1.69 ± 0.09 m, weight was 70.09 ± 12.09 Kg, BMI was 24.50 ± 3.78, duration of symptom was 132.16 ± 249.33 d, and preoperative cobb angle was 27.36 ± 9.85°. The patient’s postoperative drainage volume was 74.94 ± 27.13 mL, postoperative drainage time was 2.09 ± 0.34 d, surgical bleeding loss was 102.70 ± 46.78 mL, operation time was 119.45 ± 37.32 min, preoperative PT was 12.51 ± 1.16 s, preoperative APTT was 33.17 ± 4.91 s, preoperative INR was 1.09 ± 0.18, preoperative TT was 17.80 ± 2.46 s, perioperative Hct loss rate was 7.61 ± 4.27% and Hb loss rate was 7.94 ± 5.80%.
Patient Demographics Information.
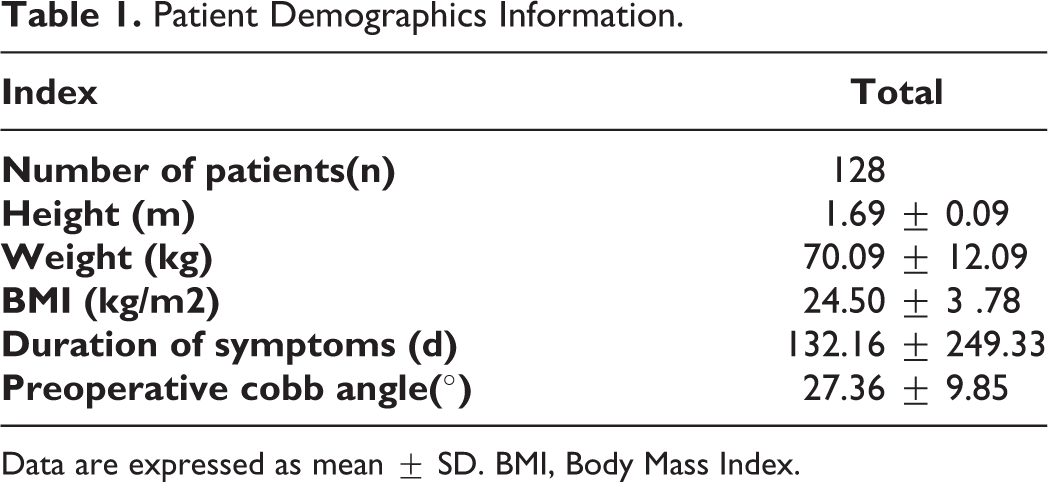
Data are expressed as mean ± SD. BMI, Body Mass Index.
As shown in Table 2, perioperative HBL was 487.98 ± 255.95 mL, and the proportion of HBL in TBL was 67.61 ± 5.19%. The gender (P = 0.014), fixation method (P = 0.000), operation time (P = 0.000), surgical bleeding (P = 0.037) and INR (P = 0.000) were significantly correlated with HBL through univariate correlation analysis. However, BMI (P = 0.913), surgical bleeding (P = 0.715) and number of surgical level (P = 0.709) were not significantly associated with HBL as shown in Table 3.
Clinical Data of Patients.

Data are expressed as mean ± SD. PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; TT, thrombin time; Hb, hemoglobin; Hct, hematocrit; HBL, hidden blood loss.
Single Factor Correlation Analysis of HBL.

Data are expressed as mean ± SD. HBL, hidden blood loss; BMI, body mass index; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; TT, thrombin time.
As shown in Table 4, there was significant positive correlation between gender (male), longer operation time, fusion with titanium plate and cage fixation, higher INR and increased HBL through multiple linear regression analysis. However, there was no significant correlation between surgical bleeding and HBL.
Results of Multiple Line Regression Analysis for HBL Coefficients.

Data are expressed as mean ± SD. HBL: Hidden Blood Loss; INR, international normalized ratio.
Discussion
In 2000, Sehat et al found that the visible blood loss and the amount of blood loss calculated according to the results of the auxiliary examination before and after surgery were significantly different during total knee arthroplasty (TKA). 13 Thus, they defined blood loss due to diffusion into the tissue, residual in the dead space or loss by hemolysis as HBL. In recent years, the study of perioperative HBL in spine surgery has attracted increasing attention. 14,15 HBL accounts for a larger proportion of TBL in transforaminal lumbar interbody fusion (TLIF) surgery. 16,17 In addition, further studies also found some spine surgeries such as PKP which previously been believed accompanied with small amount of blood loss also had significant HBL during perioperative period. 8,9
In the past, surgeons paid little attention to HBL in minimally invasive surgery, thus the risk of blood loss related complications is greatly increased especially in elderly patients who already have anemia. High levels of HBL may lead to significant organ hypoperfusion and increased incidence of cardiovascular and cerebrovascular complications. At the same time, higher HBL may increase the risk of surgical incision infection and reduce rehabilitation level, resulting in longer hospital stay time and higher costs.
Elderly patients are generally in poor physical condition, more obviously response to surgical trauma, and less tolerance for blood loss. Even a small amount of blood loss may also cause imbalance of body homeostasis, resulting in serious postoperative complications. HBL secondary to the initial ACDF procedure and the potential adverse effects of anemia may increase post-operative mortality and morbidity especially in elderly patients. Therefore, HBL should be valued carefully and monitored closely especially in elderly patients. Therefore, it is particularly important to study the risk factors.
ACDF, as a common small incision operation in spinal surgery, has also been found to be accompanied with HBL. Existing studies found that gender, ASA classification, intraoperative hemorrhage and total drainage are related to perioperative HBL of ACDF. 4,10 The present study also found that male patients have more HBL which is consistent with previous studies. 4,10,18,19 The reason why male patients have more HBL may be related to the greater height and weight and higher blood volume. These factors together with higher Hb content led to more serious blood loss when male patients lose the same volume of blood. At the same time, the muscle content of male patients is often higher than that of female patients. Therefore, greater muscle and soft tissue damage caused during ACDF operation may also result in more blood loss.
In addition, this study found that longer operation time is one of the important factors to increased HBL, which is similar to the results of previous studies. 4,10 Longer operation time will lead to greater surgical damage, which will lead to increased blood loss remaining in the dead space after surgery. At the same time, longer operation time will result in more serious body inflammatory reaction after surgery and increased hemolysis. 20 The above factors together lead to increased HBL. The present study also found that patients with higher INR had a higher amount of HBL. The reason may be that INR reflects the coagulation function to a certain extent. The increased INR indicates that blood clotting ability is poor and it is difficult to reduce bleeding. 21 In addition, high-pressure background will be slower if blood cannot be coagulated in time in the dead space and thus lead to increased HBL. 22,23
Finally, this study found that use of Zero-Profile system as an internal fixation method resulted in less HBL than “cage and plate.” The size of Zero-Profile system implant is smaller than that of “cage and plate,” thus resulting in less surgical trauma and less tissue damage. 24 In addition, Zero-Profile system does not need to adjust the length of plate after intraoperative fluoroscopy as the “cage and plate” does, thus further saving operation time and reducing surgical trauma. 25 These above factors together made Zero-Profile system fixation method have less HBL.
At the same time, all patients received oral or limited intravenous injections for pain relief and related treatments. To reduce the bias caused by infusion during the perioperative period, all patients received a similar volume of fluid. Therefore, the dilution effect of intravenous infusion cannot affect the results of the study as the intravenous infusion volume was almost the same in all patients. In addition, all patients underwent post-operative blood tests in which the amount of blood collected was minimal and had no significant impact on HBL.
However, the results of the present study are different from those of TKA and total hip arthroplasty (THA). For example, gender has an important effect on perioperative HBL in TKA. 26 The patients with lighter weight had larger HBL in THA. 27 In addition, advanced surgical methods, unstable fractures, combined medical diseases, longer postoperative injury delay time and prophylactic anticoagulation treatment increased HBL in the treatment of femoral intertrochanteric fractures. 28,29 The reason of the different results may be attributed to less surgical trauma and shorter operation time in ACDF compared with other surgery which accompanied by huge trauma and longer operation time.
This study suggested that surgeons should pay more attention to the presence of HBL in elderly patients with ACDF during perioperative period. In the future, we need to specify some strategies to reduce HBL after identifying the above factors which lead to increased HBL. We should put drainage as the risk of airway obstruction caused by hematoma is high and the consequences are catastrophic in ours experience. In addition, more delicate hemostatic procedures can be performed during surgery, such as bone wax smearing, appropriate use of thrombin and tranexamic acid.
This study also has several limitations. First, we conducted a retrospective study and the enrolled number of patients was small, future large-scale prospective studies should be conducted to verify the results. Second, the routine blood tests were performed before and at the second day after surgery to obtain Hct and Hb values, there was no long-term follow-up of postoperative anemia.
Conclusion
In conclusion, there is obvious HBL in elderly cervical spondylosis patients treated with ACDF. Male, longer operation time and higher INR increase HBL, but the application of Zero-Profile system can reduce HBL. More attention should be paid to the existence of HBL to ensure the safety of the elderly patients with risk factors.
Supplemental Material
Supplemental Material, sj-doc-1-gos-10.1177_21514593211002164 - Perioperative Hidden Blood Loss in Elderly Cervical Spondylosis Patients With Anterior Cervical Discectomy Fusion and Influencing Factors
Supplemental Material, sj-doc-1-gos-10.1177_21514593211002164 for Perioperative Hidden Blood Loss in Elderly Cervical Spondylosis Patients With Anterior Cervical Discectomy Fusion and Influencing Factors by Tongchuan Cai, Dong Chen, Shuguang Wang, Pengzhi Shi, Junwu Wang, Pingchuan Wang, Xinmin Feng, Wenjie Zhang and Liang Zhang in Geriatric Orthopaedic Surgery & Rehabilitation
Supplemental Material
Supplemental Material, sj-jpg-1-gos-10.1177_21514593211002164 - Perioperative Hidden Blood Loss in Elderly Cervical Spondylosis Patients With Anterior Cervical Discectomy Fusion and Influencing Factors
Supplemental Material, sj-jpg-1-gos-10.1177_21514593211002164 for Perioperative Hidden Blood Loss in Elderly Cervical Spondylosis Patients With Anterior Cervical Discectomy Fusion and Influencing Factors by Tongchuan Cai, Dong Chen, Shuguang Wang, Pengzhi Shi, Junwu Wang, Pingchuan Wang, Xinmin Feng, Wenjie Zhang and Liang Zhang in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by: Key Funding Project of Maternal and Child Health Research of Jiangsu Province (F201801); Guangxi Natural Science Foundation General Project (2018JJA14775). High-level Health Pro- fessionals “Six projects” Top-notch Talent Research Program of Jiangsu Province (LGY2019035).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.