
Abstract

We read with great interest the article by Bugaevsky et al. and appreciate the authors’ efforts to examine the importance of ortho-geriatric units for older patients with hip fractures. 1 The study showed the advantages of the ortho-geriatric unit in treating frail, older adults. Patients with hip fractures often have problems specific to the geriatric population, such as dementia, malnutrition, urinary problems, pain, and depression, and if the surgery is successful geriatric care will be more important than orthopedic care. We agree with the importance of organizing the ortho-geriatric unit to provide high-quality care. However, additional discussion of some alternative approaches was considered necessary, and we would like to describe them here.
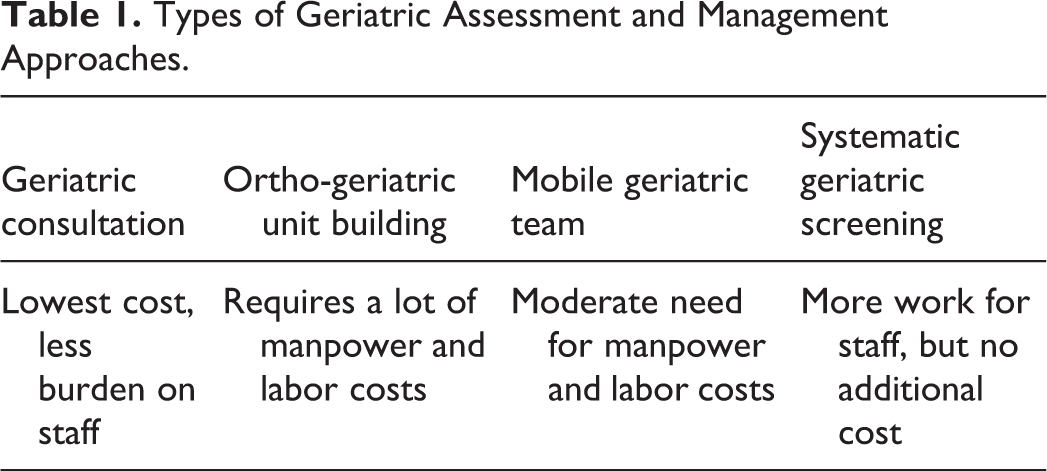
The building of an ortho-geriatric unit may indeed lead to the provision of high-quality geriatric care, but it requires more manpower and labor costs than geriatric consultation. There are also other possible intervention models (Table 1). For example, a possible approach is to introduce a mobile geriatric team to give geriatric advice. It has been reported that mobile geriatric teams could reduce the length of stay of elderly inpatients by half. 2 This team approach would probably be less costly and easier than building ortho-geriatric units. There is also a method of systematic geriatric screening of high-risk patients in the wards at the time of admission, and geriatric assessment and management of those who are found to be at risk.
Types of Geriatric Assessment and Management Approaches.
In Japan, the Ministry of Health, Labor, and Welfare reimburses and encourages the use of Comprehensive Geriatric Assessment (CGA) for hospitalized older patients. CGA helps to identify treatable health problems and appropriate goals, leading to improved outcomes for older patients. It has been reported from Japan that CGA screening shortens the length of stay in hospital for older stroke patients. 3 Such a team and screening approach may be easier than creating an ortho-geriatric unit, because it requires less manpower and money. To improve the level of hip fracture care, we should consider the characteristics and effect size of each method, along with local needs, before choosing which method to adopt.
Incidentally, there is a methodological concern with the paper by Bugaevsky et al.: the results show less renal impairment in the ortho-geriatric unit, but as the authors also state, the sample size of this study is small. The authors argue that there is an advantage to the ortho-geriatric unit in the treatment of older fracture patients, because despite the lower baseline functional ability in the ortho-geriatric unit, the improvement after rehabilitation was not significantly different between the 2 groups. However, no significant difference in mortality and functional recovery does not mean that the ortho-geriatric unit is more advantageous. It may be that the statistical power of this study was just insufficient, so sample-size calculation and statistical power need to be examined. Therefore, it would be a misinterpretation and a “spin” to argue for the superiority of the ortho-geriatric unit based on this result. 4