
Abstract
Introduction:
With respect to care setting, there are mixed results in the literature with respect to the role of trauma centers in management of isolated geriatric hip fractures. During a transition from a Level 3 to a Level 1 trauma center, significant protocol changes were implemented that sought to standardize and improve the care of hip fracture patients. The objective of this study was to determine the effects of this transition on the management, efficiency, morbidity, mortality, and discharge of geriatric hip fracture patients.
Methods:
A retrospective chart review of geriatric hip fractures treated operatively was conducted. Two cohorts were compared: hip fractures in the year prior to (2015) and year following (2017) Level 1 Trauma designation. Primary outcome measures were length of stay (LOS), transfusion rate, complication rate, and mortality rate. Secondary outcome measures were time from emergency department (ED) arrival to medical optimization, time from medical optimization to surgery, time from ED arrival to surgery, and discharge destination.
Results:
There were no differences in LOS, transfusion rate, or complication rate between the two cohorts. There was a nonsignificant trend toward lower in-hospital mortality after the transition (2.24% vs 0.83%). There were no differences in time from ED arrival to medical optimization, time from medical optimization to surgery, time from ED arrival to surgery, and percentage of patients discharged home between the cohorts.
Discussion:
Management of operative geriatric hip fractures at our institution has remained consistent following transition to a Level 1 trauma center. There was a trend toward lower mortality after transition, but this difference was not statistically significant. We attribute the variety of findings in the literature with respect to trauma center management of hip fractures to individualized institutional trauma protocols as well as the diverse patient populations these centers serve.
Introduction
The American population sustains a significant amount of hip fractures every year, and the number is only rising as the elderly population continues to grow. Hip fractures are estimated to affect 18% of women and 6% of men. 1 The global incidence of hip fractures is expected to increase from 1.26 million in 1990 to approximately 4.5 million by 2050. 1 In 2015, 5.7 of every 1000 Medicare enrollees were hospitalized with a hip fracture in the United States, and hip fracture incidence in women older than 65 years exceeded projections by almost 4000. 2,3 The rising number of annual hip fractures is costly as well; hip fracture care in the United States costs US$17 billion in 2002. 1 Medical comorbidities have increased in these patients over time, as those aged 65 years and older comprise the most common cohort for hip fractures. Taken together, these factors make management of these injuries complicated as hip fractures have been found to carry a 4.0% to 5.4% 30-day mortality, and an 18.8% to 21.9% 1-year mortality. 4 -6
One method to decrease the morbidity and mortality of hip fractures is the establishment of a geriatric comanagement service. 7 Another attempt to improve outcomes is trauma center management of hip fractures. The literature offers conflicting evidence, however, with respect to the benefits of trauma centers. It has been reported that older adults with isolated hip fractures had an increased length of stay (LOS), higher 30-day readmission rates, and higher rates of venous thromboembolism when treated at Level 1 trauma centers compared to nontrauma centers. 8 Establishment of a hip fracture service within a Level 1 trauma center, however, has been shown to decrease time to surgery, decrease LOS, and decrease costs. 9 Yet another study found that elderly individuals with hip fractures treated in high-level trauma centers did not experience significant differences in in-hospital mortality or discharge destination when compared to low-level trauma centers. 10
Our institution presented a unique opportunity to evaluate care setting with respect to geriatric hip fracture patients. On July 1, 2016, it transitioned from a Level 3 to a Level 1 trauma center. The objective of this study was to determine the effect of trauma protocols and new care paradigms, if any, on the management, efficiency, morbidity, mortality, and discharge of geriatric hip fracture patients.
Methods
Trauma Center Transition
The transition of our institution from a Level 3 to a Level 1 trauma center occurred on July 1, 2016. Prior to the transition, geriatric hip fracture patients were admitted to either the Orthopaedic Surgery service or the Internal Medicine service if management of multiple medical comorbidities was required. There was no established geriatric fracture care or protocol. Following the transition, protocol dictated that patients were admitted to the General Surgery Trauma service for management and coordination of care along with medical comanagement. Preoperative medical optimization was performed by the patient’s private primary care physician prior to Level 1 status. Following the transition, optimization was performed by a surgical hospitalist; this represented the primary role of these hospitalists. The surgical hospitalists were physicians trained in internal medicine who ensured that proper medical workups and interventions were carried out prior to operative fracture fixation. The venous thromboembolism prophylaxis, patient population, and orthopaedic surgeons remained unchanged throughout the transition.
Data Acquisition
After institutional review board approval was obtained, a retrospective chart review of geriatric hip fracture patients treated operatively at our institution was performed. Informed consent was not contained from the patients whose charts were reviewed. The calendar year prior to trauma center transition (January 1, 2015-December 31, 2015) comprised the pretrauma center (PrTC) cohort and the calendar year following trauma center transition (January 1, 2017-December 31, 2017) comprised the posttrauma center (PoTC) cohort. Patients younger than 50 years of age were excluded from the study. Only the hospital admission in which the hip fracture treatment occurred was reviewed.
Outcome Measures
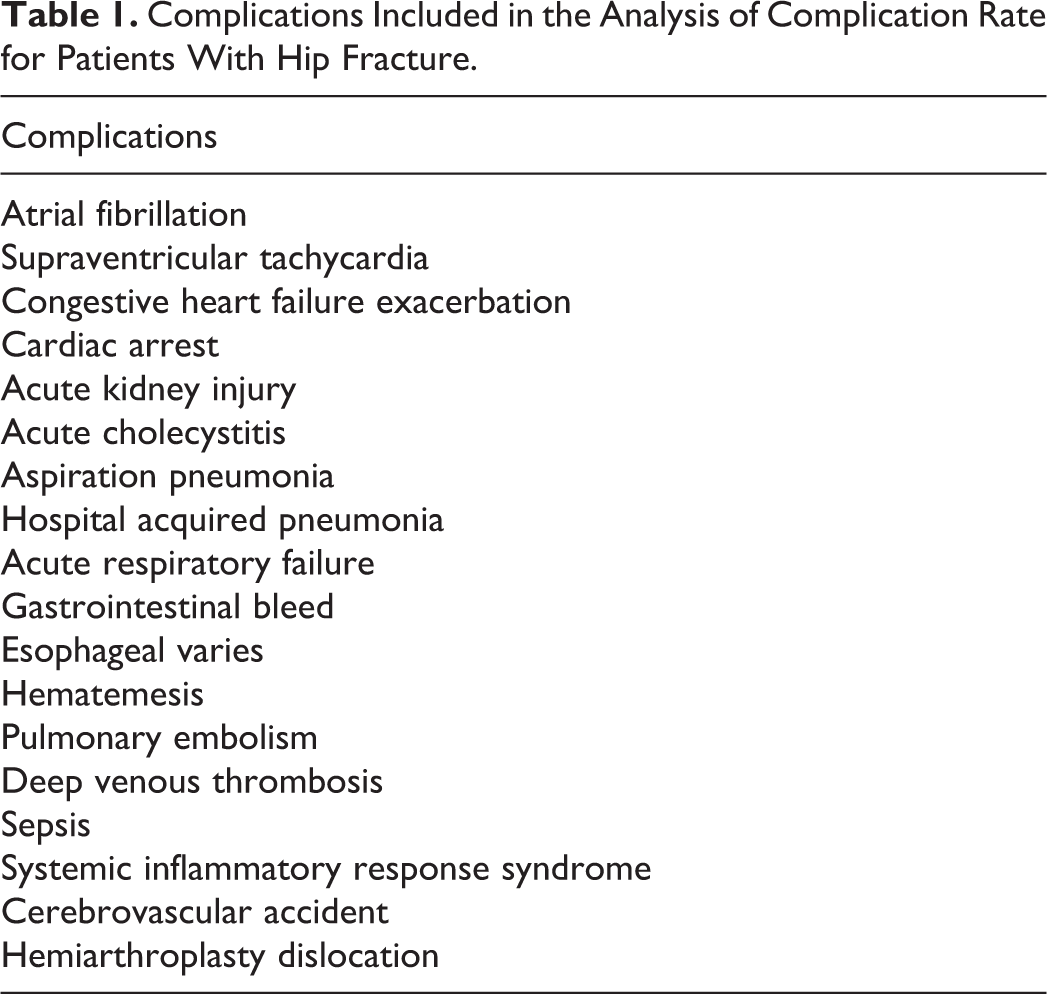
Primary outcome measures were LOS, transfusion rate, complication rate, and mortality rate. Secondary outcome measures were time from emergency department (ED) arrival to medical optimization, time from medical optimization to surgery, time from ED arrival to surgery, and discharge destination. Complications can be viewed in Table 1.
Complications Included in the Analysis of Complication Rate for Patients With Hip Fracture.
Data Analysis
Age between cohorts was compared using a t test. Sex, percentage of patients operated on within 48 hours, American Society for Anesthesiologists (ASA) classification, comorbidity prevalence, surgical procedure, and admitting service distributions were compared between cohorts using chi-square independence tests. Length of stay, time from ED arrival to medical optimization, time from medical optimization to surgery, and time from ED arrival to surgery were transformed using a natural log transformation and compared using linear regression. Estimates were then exponentiated to return them to their original scale. Transfusion rate, complication rate, and home discharge percentage were analyzed using logistic regression. Due to the small number of patients in each cohort who did not survive to discharge, mortality rate was compared using a Fisher exact test.
For all continuous primary and secondary outcomes, univariate linear regression was performed for medical comorbidities to determine any cofounders that existed. For all frequency outcomes, comorbidities were analyzed with logistic regression models. Comorbidities analyzed included diabetes mellitus, hyperlipidemia, chronic kidney disease, cardiac disease, respiratory disease, depression, dementia, and cancer. No relationships were found, and thus multivariate analysis was not performed. An α level of 0.05 was utilized as the cutoff point for significance for all data analysis.
Results
A total of 223 hip fractures were identified in 2015 to comprise the PrTC cohort and 240 in 2017 to comprise the PoTC cohort. Demographic information can be viewed in Table 2. Average ages and standard deviations of the PrTC and PoTC cohorts were 82.4 (10.0) and 83.2 (10.3), respectively (P = .3978); 53 (23.8%) of the PrTC patients were male compared to 70 (29.2%) of the PoTC patients (P = .2600). The median ASA classification of both cohorts was 3, and analysis of their respective ASA classification distributions showed that they were not significantly different (P = .4222). The prevalence of diabetes mellitus (P = .6881), hyperlipidemia (P = .4651), kidney disease (P = .3350), cardiac disease (P = .1555), respiratory disease (P = .0972), cancer P = .2659), dementia (P = .7576), and depression (P = .3265) was not different between the PrTC and PoTC cohorts.
Demographic Information for the PrTC and PoTC Cohorts.a

Abbreviations: ASA, American Society for Anesthesiologists; PrTC, pretrauma center; PoTC, posttrauma center.
a Mean and standard deviation are given for age. Number and percentage of males in each cohort are given for gender; P value for ASA classification reflects a chi-square test.
Procedures performed for hip fracture include hemiarthroplasty, total hip arthoplasty, long cephalomedullary nail, short cephalomedullary nail, cannulated screw fixation, and sliding hip screw. There was no difference in distribution of procedures performed between the 2 cohorts (Table 3; P = .3009).
Breakdown of Procedures Performed for the PrTC and PoTC Cohorts.a

Abbreviations: CS, cannulated screw fixation; HA, hemiarthroplasty; THA, total hip arthroplasty; PrTC, pretrauma center; PoTC, posttrauma center; SHS, sliding hip screw.
a A chi-square test comparing the distributions between the two cohorts yielded a P value of .3009.
The distribution of admitting service of the PrTC cohort was significantly different from that of the PoTC cohort (Table 4; P < .0001). Prior to transition, geriatric hip fracture patients were admitted to the Medicine or Orthopaedic Surgery services. Following the transition, most patients were admitted to the Trauma Surgery service.
Breakdown of Admitting Service for the PrTC and PoTC Cohorts.a

Abbreviations: PrTC, pretrauma center; PoTC, posttrauma center.
a A chi-square test comparing the distributions between the 2 cohorts yielded a P value <.0001.
None of the primary outcome measures were statistically significantly different between the PrTC and PoTC cohorts (Table 5). Average LOS (P = .8524), transfusion rate (P = .2874), and complication rate (P = .4698) were all statistically equivalent between the two cohorts. Mortality rate was almost three times as large in the PrTC cohort (2.24% vs 0.83%), but this difference did not reach statistical significance (P = .2704).
Comparison of the Primary Outcome Measures Between the PrTC and PoTC Cohorts.a
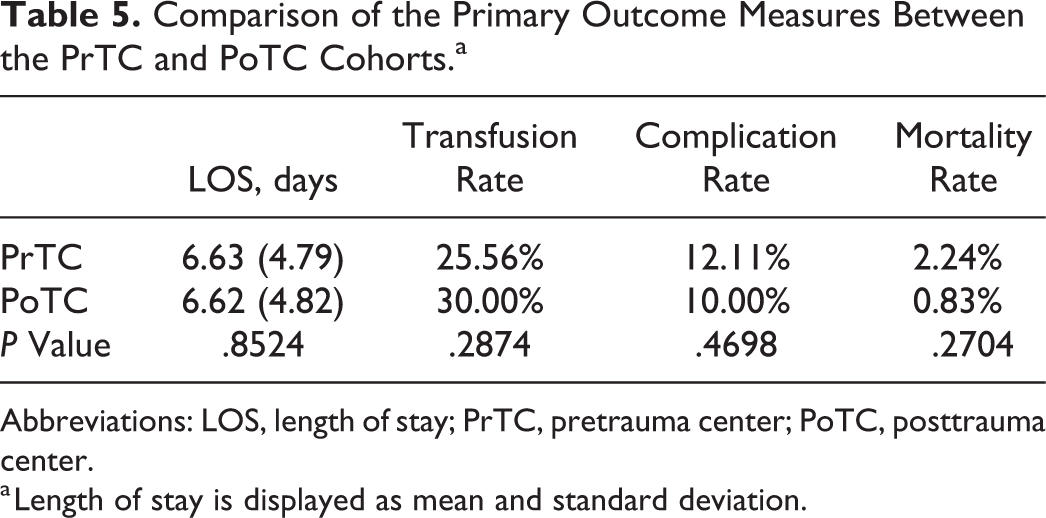
Abbreviations: LOS, length of stay; PrTC, pretrauma center; PoTC, posttrauma center.
a Length of stay is displayed as mean and standard deviation.
Likewise, none of the secondary outcome measures were statistically significantly different between the PrTC and PoTC cohorts (Table 6). There was no difference with regard to time from ED arrival to medical optimization (P = .5877), time from medical optimization to surgery (P = .9516), time from ED arrival to surgery (P = .6035), and home discharge percentage (P = .9110) between the two cohorts. Additionally, 71.3% (159) of patients in the PrTC cohort were operated on within 48 hours, compared to 70.4% (169) of patients in the PoTC cohort (P = .9101). Among the 64 patients in the PrTC cohort who were operated on after 48 hours, 3 (4.7%) did not survive to discharge. Among the 71 patients in the PoTC cohort who were operated on after 48 hours, 1 (1.4%) did not survive to discharge. This difference was not statistically significant (P = .3450). Furthermore, 15.6% (10) of these patients in the PrTC cohort experienced a complication, compared to 11.3% (8) in the PoTC cohort. This difference was also not statistically significant (P = .4571).
Comparison of the Secondary Outcome Measures Between the PrTC and PoTC Cohorts.a

Abbreviations: PrTC, pretrauma center; PoTC, posttrauma center.
a All values displayed are means and standard deviations.
Discussion
This study found that transition to a Level 1 trauma center did not affect the care of operative geriatric hip fracture patients at a large, tertiary care institution. Length of stay, transfusion rate, complication rate, mortality rate, time from ED arrival to medical optimization, time from medical optimization to surgery, time from ED arrival to surgery, and percentage of patients discharged home were all unchanged following the transition. Mortality rate trended toward being lower following the transition, however. Care provided to these patients following trauma center designation was not inferior to care provided beforehand. These findings are a departure from the current literature with respect to the effects of trauma center care of isolated hip fractures in elderly individuals.
It has been suggested that older adults (65+ years) with isolated hip fractures fare worse when treated at Level 1 trauma centers. In a retrospective cohort study, it was found that older adults had an increased LOS, higher 30-day readmission rates, and higher rates of venous thromboembolism when treated at a Level 1 trauma center compared to nontrauma centers. 8 Another study found that older patients with isolated hip fractures tended to have higher mortality and lower odds of being discharged home when treated at high-level trauma centers compared to low-level trauma centers, but these trends were not statistically significant. 10 In contrast, establishment of a “hip fracture service” has been shown to decrease time to surgery, increase the amount of patients discharged home, and decrease costs. 9 Establishment of a geriatric trauma center in another institution had no effect on time from presentation to surgery or discharge destination. Complication rate and LOS were both significantly lower following transition to geriatric trauma center. 11 Additionally, it has been found that there is reduced mortality and improved physical function at 1 year for patients with unstable pelvic and severe acetabular injuries when they are treated at a Level 1 trauma center. 12 Many extol the benefits of trauma centers for the management of hip fractures in the elderly individuals, with respect to efficiency, morbidity, and financial measures. 13
Average LOS for the patients in both cohorts of the present study was just over 6.6 days, which is similar to what has been reported in the literature for operative hip fractures. 6 It has been suggested that LOS for hip fracture patients may not affect short-term mortality, as 30-day risk of death remained unchanged over a 9-year period in which LOS significantly decreased. 14 In terms of mortality, our study demonstrated that the in-hospital mortality rate of hip fracture patients was 2.24% prior to trauma center transition and 0.83% following it. These numbers are consistent with those described in the literature, where in-hospital mortality has been reported at 1.8% to 5.0%. 15,16 Before the transition, 71.3% of patients were operated on within 48 hours, compared to 70.4% after. In an Australian hospital, 67% of patients had surgery within 48 hours after a hip fracture service was established, compared to 52% before. 9 In a review of hip fracture patients in Southern Ontario, 90% of patients underwent surgery within 48 hours of admission in community hospitals. 16 This number dropped to 71% in academic hospitals. A database study with over 500, 000 hip fractures from 2012 to 2013 reported a 75.2% rate of surgery within 48 hours. 15 In the present study, 7.83% of hip fracture patients were discharged home prior to trauma center transition, compared to 8.09% following the transition. This is slightly lower than the 10.0% to 13.3% that has been reported for isolated geriatric hip fractures. 16,17
This study is not without limitations. It is a retrospective chart review, and only the hospital admission in which surgery occurred was reviewed. Complications or deaths that occurred following hospital discharge are thus unaccounted for. Additionally, while our sample size for each cohort was appreciable, this study was underpowered to detect significant differences in some of the outcome measures examined, such as mortality rate. Lastly, the data analyzed in this study were derived from a single institution. It is unlikely that this single institution is representative of all centers that treat geriatric hip fractures. Thus, the findings reported here may not be generalizable to all hospitals.
Here, we report that transition to a Level 1 trauma center did not affect care of operative geriatric hip fracture patients at our large tertiary care hospital. Effectively, Level 1 care of the patient population studied was not inferior to care prior to trauma center designation. Trauma center care may potentially be better in this population, as a significant difference in mortality rate may emerge as we get further away from the transition date. The variety of conflicting results reported in the literature with respect to trauma center management of hip fractures is likely due to individualized institutional protocols and the diverse patient populations served by different centers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.