
Abstract
Introduction
Approximately 300 000 hip fractures occur annually in the USA in patients >65 years old. Early intervention is key in reducing morbidity and mortality. Our institution implemented a collaborative hip fracture protocol, streamlining existing processes to reduce time to OR (TTO) and hospital length of stay (LOS). Our aim was to determine if this protocol improved these outcomes.
Study Design
We conducted a retrospective cohort study using our level-1 trauma center’s trauma registry, comparing outcomes for patients >60 years old with isolated hip fractures pre-and post-hip protocol implementation in May 2018. Our primary outcomes were TTO and in-hospital mortality. Secondary outcomes included LOS and postoperative complications. Univariate analysis was done using chi-square and T-test.
Results
We identified 176 patients with isolated hip fractures: 69 post- and 107 pre-protocol. Comparing post- to pre-protocol, TTO decreased by 18hrs (39 vs 57h; P = .013) and patients had fewer postoperative complications (9 vs 23%; P = .016) despite post-protocol patients being more likely to have diabetes (42 vs 27%, P < .05), elevated BMI (22 vs 25; P < .001), and to be current smokers (9 vs 2%; P < .05). LOS and in-hospital mortality also decreased (11 vs 20d; P = .312, 4.3 vs 7.5%; P = .402). Post-protocol patients were more likely to go to the OR within 24hrs of presentation (39 vs 16%; P < .001) and to go straight from ED to OR (32 vs 4%; P < .001).
Conclusion
TTO, LOS, and postoperative complications for isolated hip fracture patients were lower post-protocol. Though not all statistically significant, this trend indicates that the protocol was helpful in improving hip fracture outcomes but may require further improvement and institution-wide education.
Keywords
Introduction
There are approximately 330000 hip fractures seen annually in emergency departments across the United States. While the mean age of patients with femoral or acetabular fractures is 77 years old, some estimates project that the incidence of hip fractures is increasing and could reach over a million a year by 2050 for individuals over 45 years old. 1
Early operation of hip fractures has been extensively studied as a means of improving patient morbidity and mortality.2-9 In a 2017 retrospective cohort analysis of 42230 adults undergoing hip fracture surgery, wait time of over 24 hours was found to be associated with a higher risk-adjusted likelihood of 30 day mortality, 4 a trend also shown in Morrissey’s 2016 study in Injury. 7 Early surgical treatment is associated with an improved ability to return to independent living, a reduced risk of developing pressure ulcers, and a shortened hospital stay. 10 In addition, treatment of hip fractures represents a significant cost to the healthcare system, with an annual economic burden of $5.96 billion. Early intervention may decrease the cost of treatment by $15,400 per patient. 11
Retrospective studies have clearly demonstrated that early surgical intervention of hip fractures leads to better outcomes and reduced costs. HIP ATTACK, a recent randomized controlled study, showed that accelerated surgery was associated with lower rates of delirium and length of hospital stay (LOS), although not 90-day mortality or major complications. 12 Team-based approaches to geriatric hip fractures have also been shown to improve outcomes. Bracey et al showed that patients with comanaged orthopedic-geriatric care had reduced inpatient LOS by 1.6 days. 13 Suhm et al 14 showed that both LOS and complication rate decreased with comanaged care. Lister Hospital’s orthopedic department in the United Kingdom (UK) implemented dedicated care teams for hip fracture patients, after which the hospitals reported a significant decrease in LOS and time to operation (TTO). 15 Recently, an urban safety-net hospital in the US implemented a hip fracture protocol which significantly increased the number of patients admitted to a surgery service in a monitored setting but failed to demonstrate decreased TTO or LOS. 16 Others have introduced a multidisciplinary approach that resulted in a 10% improvement in the percentage of patients having surgery within 24 hours. 17
As a level-1 trauma center that routinely manages hip fracture patients, we have implemented our own unique collaborative hip fracture protocol (Figure 1), streamlining existing processes to expedite surgical intervention for isolated hip fracture patients. The protocol’s purpose was to optimize the number of patients going to the operating room within 24 hours of their triage time and to maintain a hospital length of hospital stay of under 96 hours. Our study’s objective was to determine if this protocol had an effect on time from admission to surgery, length of hospital stay, postoperative complications, and mortality rates. Protocol. H&P= History and Physical, DVT ppx = STAT dose of heparin subcutaneous 5000 U regardless of time for surgery, continue every 8 hours, do not hold before OR, geriatric/palliative for patients >65 years old.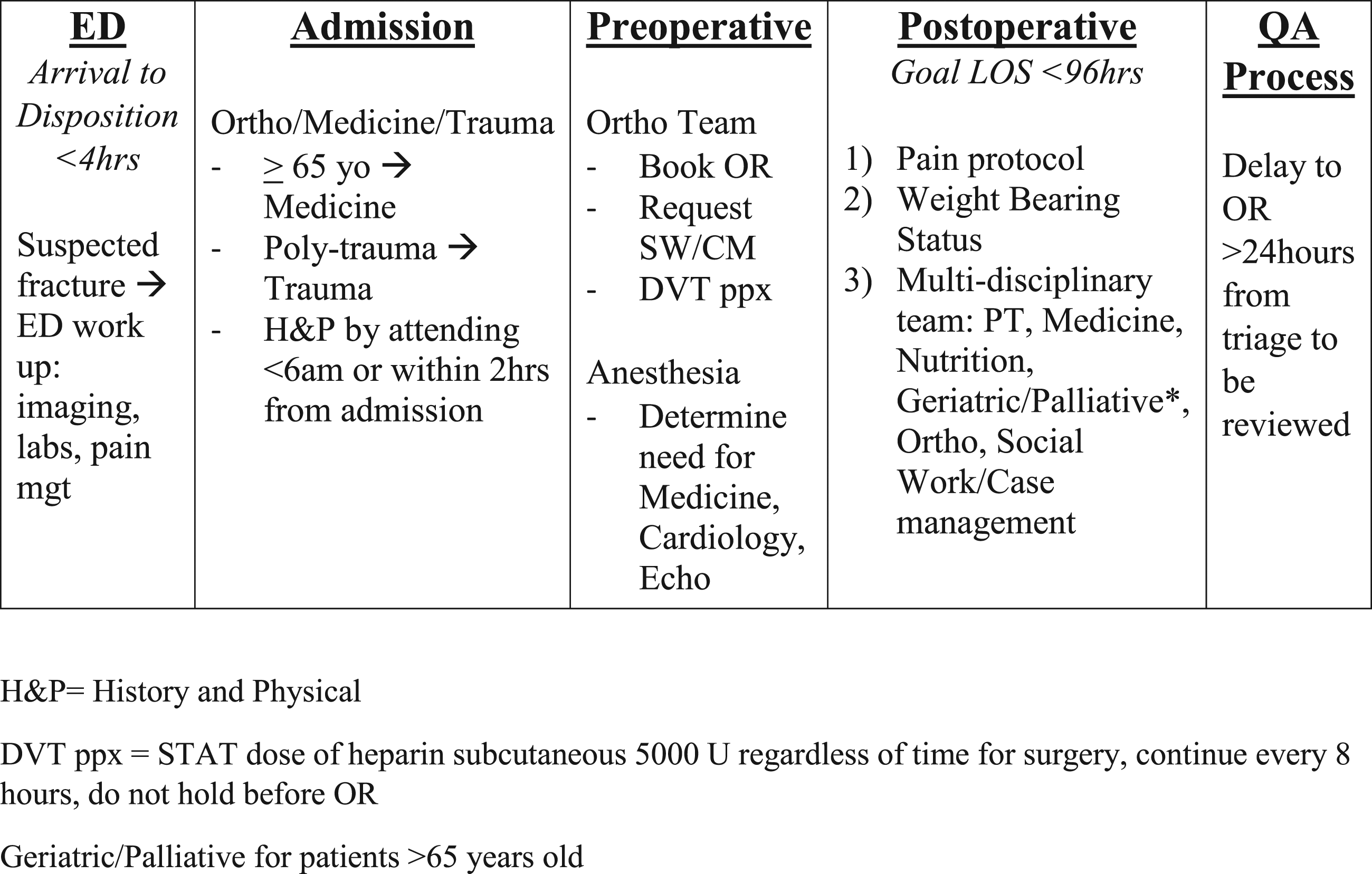
Methods
We conducted a retrospective cohort study using our institution’s trauma registry. Our institution is a Level-1 Trauma Center located in a large urban area. The center’s trauma registry contains retrospectively collected data of all trauma patients 18 years of age or older who come to our Level-1 Trauma Center. For each patient, information such as demographics, time spent in the emergency room, and resulting surgical operations are collected as well as postoperative complications, mortality, and discharge disposition. Appropriate approval by the institutional review board was obtained prior to initiation of any aspect of this study.
To effectively improve outcomes, our protocol defines the hospital stay into 4 discrete phases: Emergency Department (ED), Admission, Preoperative, and Postoperative with clearly defined roles for all personnel in each area. The ED phase focuses on diagnosing patients so that they may be admitted in under 4 hours. The Admission phase ensures that patients are accurately allocated to orthopedic, Medicine or Trauma teams and that History and Physicals are completed in a timely matter. The Preoperative phase details the roles of the orthopedics and anesthesia in expediently organizing the OR, giving DVT prophylaxis, and completing the necessary preoperative clearance, including consults to other services as an echocardiogram when necessary so that surgery is performed within 24 hours of admission. The Postoperative phase calls upon a multidisciplinary team including physical therapy, nutrition, social work and when appropriate geriatrics and palliative to optimize the patient to be discharged within 96 hours of surgery. The time frame of 96 hours was a steep goal, the collaborating teams decided on to strive for when creating the protocol. The protocol also enlists a Quality Assurance (QA) process so that delays in these phases will be reviewed by the Trauma Performance Improvement and Patient Safety program. The protocol is signed by heads of ED, Medicine, Anesthesia, Surgery, Cardiology, Rehab, Social Work, and Nursing. By distinctly defining responsibilities for all involved services, crucial patient care tasks may be undertaken simultaneously.
As our institution implemented a hip fracture protocol in May 2018, our goal was to compare hip fracture outcomes before and after the protocol was implemented. We included all methods of injury and then extracted all patients over 60 years old from our institution’s trauma registry with isolated traumatic hip fractures and then separated them into 2 groups: the pre-protocol group from January, 2016, to May, 2018, and the post-protocol group from May 2018 to September 2019. Changes to the hospital’s electronic medical in 2016 meant that data could not be collected prior to January 2016. We wanted include as much data as possible which is why we collected data through September 2019. Patients with isolated hip fractures were defined as patients with isolated intertrochanteric, subtrochanteric, acetabular, or femoral neck fractures. Patients with concomitant femoral shaft/distal femoral fractures or pathologic fractures were not included. All patients with other fractures, pelvic fractures, and hip dislocations were excluded. Patients with missing data or those who did not have surgery after their hip fracture were also excluded from the study (Figure 2). Flow chart depicting patient selection criteria.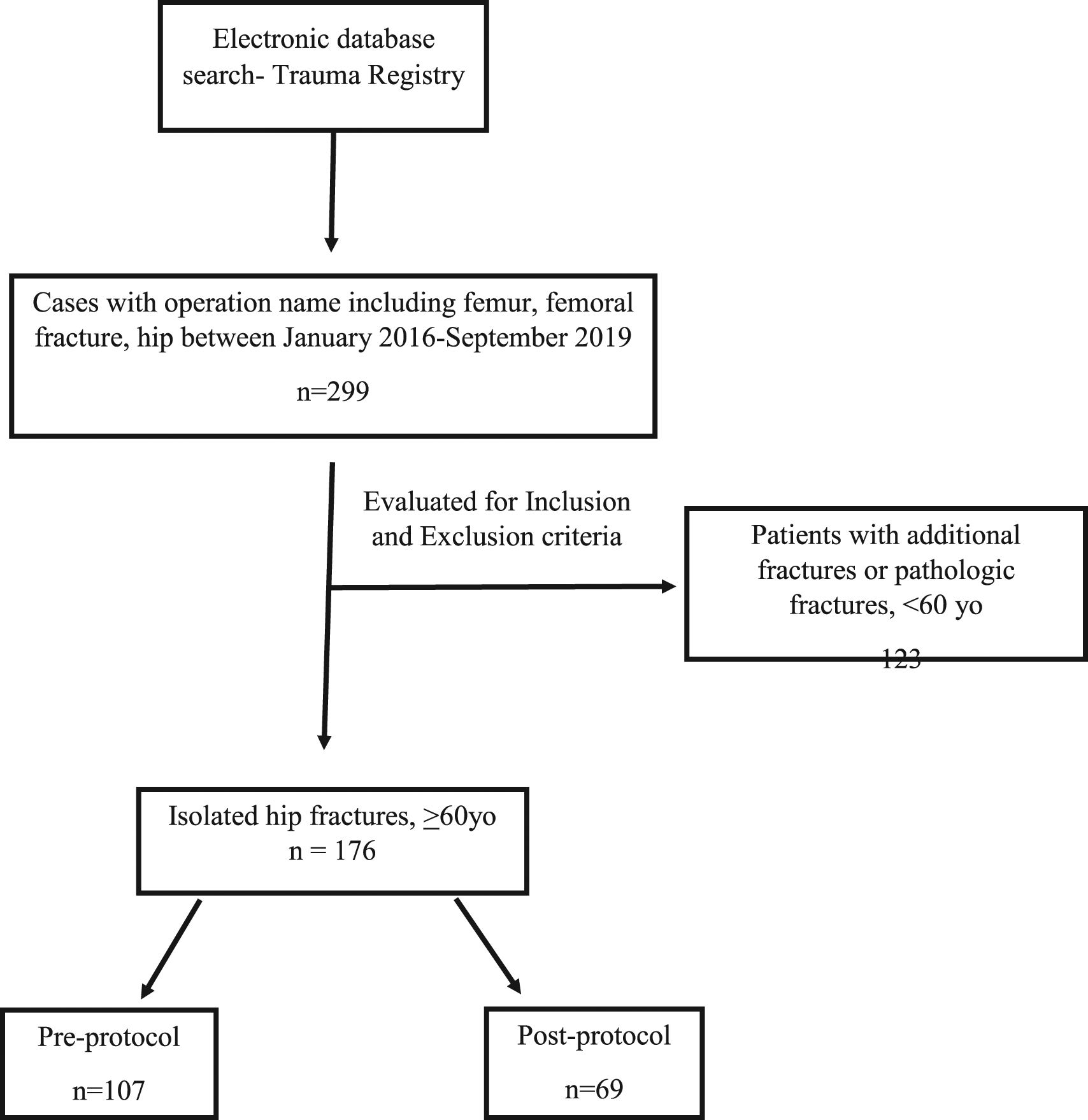
For all patients, we extracted demographics, comorbidities, emergency room variables such as vital signs, method of arrival, and method of injury, postoperative complications and disposition including mortality. Our primary outcomes were time to operating room (TTO) and in-hospital mortality. Secondary outcomes included length of stay (LOS) and postoperative complications. Postoperative complications included: arrhythmias, aspiration, cardiac arrest, decubitus ulcer, DVT, MI, PE, UTI, seizure, SBO, renal failure, liver failure, stroke, and alcohol withdrawal. Data from the pre- and post-protocol groups were compared using univariate analysis with chi-square analysis and T-test. Multivariate regression analysis was performed to identify whether protocol group, race, sex, diabetes, or smoker status were predictive factors for postoperative complications or for going to the operating room within 24 hours of arrival to the emergency room. All data analysis was performed using SPSS version 24.0 (IBM Corp, Armonk, New York, USA). The threshold for statistical significance was set at P < .05.
Results
Comparison of demographics between patients in the pre- and post-protocol groups.

Comparison of comorbidities between patients in the pre- and post-protocol groups.

Comparison of ED characteristics between pre- and post-protocol hip fracture patients.

Comparison of outcomes between pre- and post-protocol hip fracture patients.
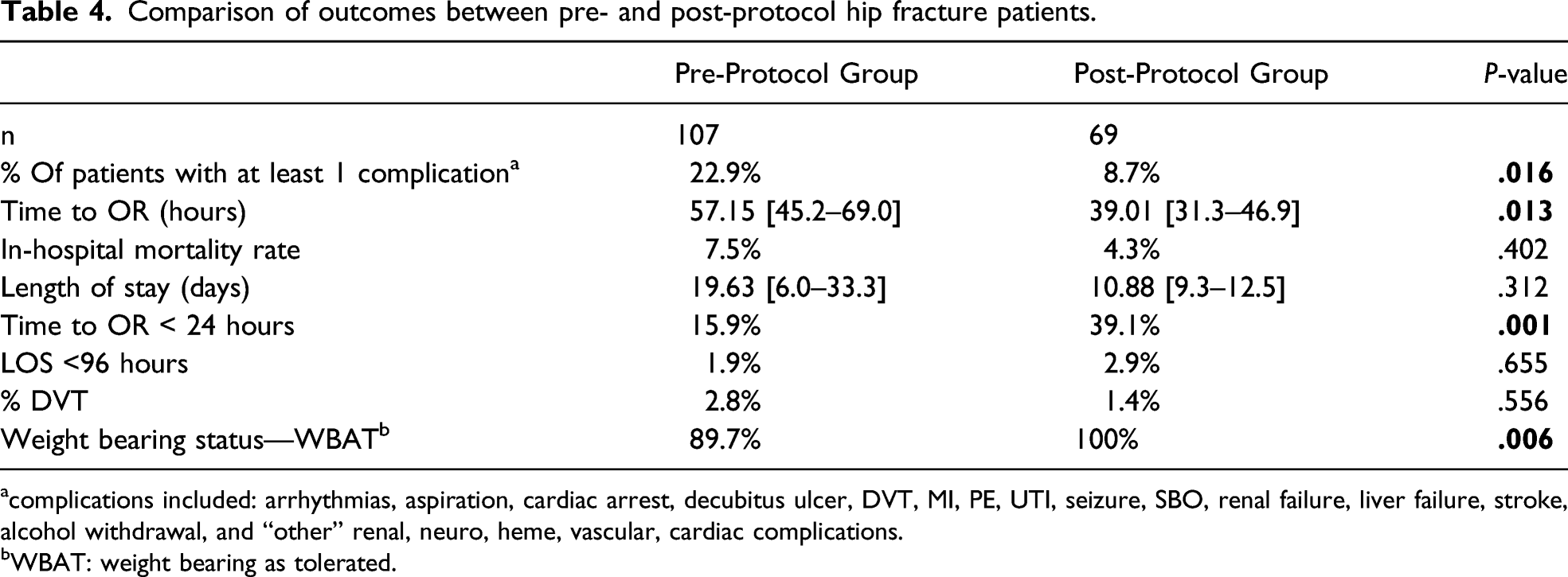
acomplications included: arrhythmias, aspiration, cardiac arrest, decubitus ulcer, DVT, MI, PE, UTI, seizure, SBO, renal failure, liver failure, stroke, alcohol withdrawal, and “other” renal, neuro, heme, vascular, cardiac complications.
bWBAT: weight bearing as tolerated.
Multivariable regression analysis showed that the pre-protocol group was associated with a higher risk of complications (OR=.26, 95% CI [.09-.74]; P = .011) and a lower chance of going to the OR in less than 24 hours (OR= 3.775, 95% CI [1.754–8.124]; P = .001). Race, sex, diabetes, and smoking were not associated with higher rates of complications or a decreased TTO.
Disposition of patients.

Discussion
With over 300000 traumatic hip fractures occurring each year in the United States, neither orthopedic nor trauma surgery teams are strangers to the management of these patients. Knowing that early intervention is key in reducing morbidity and mortality, the orthopedic and trauma surgery departments at our Level-1 Trauma Center created a protocol to streamline already existing processes in order to reduce time to OR and hospital length of stay. These processes included having distinct phases of treatment, specifying time intervals and expediting time to the OR. It included protocolization of the indication of preoperative echocardiogram, increasing availability of orthopedic operating room staff over the weekend, and involving social work and rehabilitation services early on in patient admission. A year and a half after the protocol was implemented, we sought to determine whether the protocol made a difference.
We found that TTO was significantly decreased after protocol implementation despite post-protocol patients having more comorbidities. In addition, post-protocol patients were more likely to go to the OR within 24 hours of presentation and to go straight to the OR from the ED. Further investigation into patients who had to go to the intensive care unit first is warranted as it is unclear if this was due to delay in surgery or the stability of the patient. LOS and in-hospital mortality were also decreased post-protocol. Although not statistically significant, the post-protocol LOS range was narrower. Overall, the trend from pre- to post-protocol improved.
This study included several limitations. Data was collected retrospectively; therefore, we did not have access to all the variables that we would have wanted, including long-term complications. In addition, granularity of data was frequently limited; for example, complications were inconsistently listed in the medical record, and thus in the extracted database, (ie, “other cardiac complication” in some instances, or “myocardial infarction” or “cardiac arrest”). Additionally, an important complication of delirium was not recorded for these patients. The data on patients after discharge is sparse as patients are often lost to follow up. While Table 5 is able to provide the limited data on disposition, further investigation on discharge location will be worthwhile. Cases with missing data had to be excluded which decreased the protocol pool which may have impacted the results. In addition, our hospital went through a change in the electronic medical record, which made gathering data before and after protocol implementation difficult as there was not always sufficient data recorded. There may also have been some degree of human error while entering data into the database. Finally, we had a limited number of patients. Future analyses could show greater improvements in our outcomes by including more patients, expanding the trauma registry to better report complications, improving follow-up, and allowing our healthcare providers to become more familiar with the protocol.
Many studies on this subject compare outcomes between trauma and non-trauma designated centers or look at hospitals before and after becoming trauma hospitals. Data suggests that outcomes are in fact similar or worse in trauma designated hospitals compared to non-trauma centers. In a study by Nelson-Williams et al, the authors found that there was no significant difference in mortality for geriatric hip fracture patients when brought to a level I or II vs a level II or undesignated trauma center. 18 Barr et al out of the UK, examined morbidity and mortality before and after the hospital became a major trauma center, showing that there was a significant increase in postoperative medical complications and TTO and that there was no change in mortality rate once the hospital became a major trauma center. 19 These studies attribute this discrepancy to resource allocation. A major trauma center attracts cases that require more hospital resources to battle the severity. These higher acuity cases then displace hip fracture cases which are considered lower acuity. 12
When we looked at our own trauma institution to determine how to improve outcomes, our findings shared similarities with other studies. Friedman et al, 20 Christiano et al, 16 and Burton et al 17 reported improved outcomes in geriatric patients with hip fracture after implementation of a protocol, which further highlights the importance of protocol-driven care. They showed that expedited surgical care improved time to surgery from 20.22 to 15.33 hours but did not show a difference in-hospital length of stay or mortality. The post-protocol group in the study by Christiano et al exhibited a decrease in complications (from 23–4%) and length of stay (13.2–12 days) compared to the pre-protocol group, but no significant decrease in time to surgery. 16 In contrast, we observed an increase in the number of patients who made it to the OR within 24 hours of arrival from 16 to 39% after protocol implementation. This discrepancy could be driven by differences in sample size as Christiano et al had an n = 633 while our study had an n = 176. Friedman et al’s study found that length of stay was significantly shortened (23.2–4.6 days). 20 While we did not observe any significant difference in length of stay, this discrepancy may be accounted for by their focus on incorporating geriatricians into patient care, which may have had a positive effect on length of stay. Overall, it shows that protocol-driven care improves results and that a multidisciplinary approach is most effective.
As the cost of hip fracture management keeps rising and is projected to increase by 50% between 2005 and 2025, 21 studies have examined whether a faster time from ED arrival to operation could reduce hospital costs. In a retrospective review by Judd and Christianson, 10 657 patients over age 65 were divided into an early intervention group of surgery in less than 6 hours after arrival and a late intervention group surgery after at least 6 hours after arrival. The authors found that the average cost of the early intervention group was significantly lower by $15,400 (P = .0086) per patient—$1.7 million for the entire cohort. 3 The total cost of stay for hip fracture patients ranges from $18,000 to $32,000 and 29% of hospital costs can be attributed to length of stay. 22 The cost of hip fractures does not stop after patients leave the hospital as patients not only require medical follow-up but also require help to complete their activities of daily living. Optimizing patient care could result in fewer healthcare dollars spent on such patients and significant savings for the healthcare system and hospitals. A protocol focusing on decreasing hospital LOS is therefore particularly important in decreasing overall costs.
Conclusion
As we are faced with an expanding elderly population, traumatic isolated hip fractures in patients over 60 years old will become more common. 1 Given the importance of surgical timing in reducing morbidity and mortality in these patients, efficiency in optimizing these patients to undergo surgery and discharging them from the hospital is critical. Implementing a collaborative hip fracture protocol helped achieve goals of decreasing overall mortality for patients with isolated hip fractures and revealed the utility of protocol in reducing length of hospital stay, time to OR, and postoperative complications. It is important to build on the progress that has already been made. The departments involved in the protocol (ED, orthopedic surgery, trauma surgery, anesthesia, cardiology, rehabilitation medicine) should all be aware of the goals for each patient and the specifics of the protocol. Geriatricians should be made an integral part in the postoperative care of these patients. Education on the protocol should be expanded to all healthcare personnel involved in the care of a patient with a hip fracture.
Future work will focus on expansion and improvement of the granularity of postoperative complication reporting in the trauma registry. Additionally, further efforts will be taken to improve follow-up reporting for these patients after discharge. As we believe that implementation of a hip fracture protocol could significantly reduce the financial impact of hip fractures, as it reduces the TTO, LOS and complication rates, we will continue to expand and re-evaluate our hip fracture protocol. We believe our findings should encourage other centers to adopt inter-disciplinary hip fracture protocols.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.