
Abstract
Introduction
The COVID-19 pandemic has profoundly impacted global healthcare systems, necessitating substantial shifts in patient care strategies. The pandemic’s onset led to drastic operational changes in hospitals, including reduced bed capacity and staffing levels, which could have further influenced the mortality outcomes for geriatric patients. The study aimed to assess the impact of the COVID-19 pandemic on 1-year mortality rates of surgically treated geriatric hip fractures.
Methods
This retrospective, single-center cohort study included 346 participants aged 65 and above who underwent surgical treatment for hip fractures. We compared mortality rates between the pre-COVID and COVID eras. Data included demographics, treatment, complications, and COVID-19 status. The independent samples t test and Chi-square tests (or Fisher’s exact test) were used for comparisons for era cohorts. Survival probabilities were assessed using Kaplan-Meier, while multivariate analysis identified mortality predictors.
Results
175 patients were included in the pre-COVID era, and 171 patients were included in the COVID era. During the COVID era, the 30-day mortality rate was 11.7% (compared to 13.7% in the pre-COVID era, p = 0.573), and the 1-year mortality rate was 43.9% (compared to 49.1% in the pre-COVID era, p = 0.325). The overall 1-year mortality rate was 46.5%. Patients who underwent surgery within 48 hours had a higher 1-year survival rate (60.5%) compared to those with delayed surgery (51.2%), p = 0.031. Additionally, patients not admitted to the ICU had a higher 1-year survival rate (74.7%) than those who were admitted (44.9%), p < 0.001. 70.1% of the total deaths occurred within the first 90 days.
Conclusion
Elderly patients with hip fractures experienced high mortality rates before and during the pandemic. This study demonstrates that the 1-year mortality rates of geriatric hip fractures were not significantly affected by the pandemic. The findings emphasize the importance of pandemic preparedness and prompt surgeries and attentive ICU care in reducing mortality rates.
Introduction
The novel coronavirus (COVID-19) pandemic has presented unprecedented challenges to global health systems, dramatically altering patient care protocols, especially for patients rendered more vulnerable due to age or comorbidities. Elderly individuals, especially those aged 65 and over, are part of this vulnerable group due to their frequent co-existing conditions and heightened risk for severe COVID-19 outcomes.1-4
Hip fractures, frequently seen in the elderly population, are associated with significant morbidity and mortality.5,6 In a meta-analysis, the prevalence of COVID-19 was found to be 13% and was associated with a crude mortality rate of 35%, which was a significantly increased risk compared to those patients without COVID-19. 7 In the period before COVID-19, the 1-year mortality rates for patients with hip fractures varied between 14% and 40%.8-10
The pandemic situation has necessitated a shift in healthcare priorities and resources, potentially influencing the standard care procedures for such conditions.11-15 The unprecedented burden that the pandemic has placed on healthcare systems worldwide may have disrupted these established protocols, led to a decrease in both emergency and elective operations in orthopedic surgery.16-20 Significant interruptions were observed particularly in the treatment processes of hip fracture patients, leading to increased morbidity and mortality rates. 21
During the early stages of the COVID-19 era in our hospital, all elective orthopedic surgeries were canceled, and the ward capacity was lowered from 29 beds to 21 beds, marking a reduction of approximately 27.6%. Each patient stayed in a single occupancy room. Attendants were not allowed to accompany patients unless absolutely necessary. Patient visits were prohibited. Rooms of COVID-positive patients were visited with special protective clothing. Some residents and nurses were assigned to COVID wards and services, resulting in a reduction of approximately 9%–18% in the number of residents, which was 11 before the pandemic. The number of employed nurses also decreased from 4 to 2-3, depending on the workload, leading to a reduction of up to 50% in staffing levels.
This study aims to examine the impact of the COVID-19 era on the mortality rate of patients aged 65 and over who have been treated for hip fractures. By comparing outcomes between the pre-COVID and COVID-19 eras, our objective is to uncover the effects of such global health crises on this critical aspect of elderly patient care.
Methods
This retrospective cohort study was conducted at Trakya University Hospital and focused on geriatric patients who underwent surgical treatment for hip fractures between January 2018 and December 2021. Ethical approval was granted by the ethics committee under protocol code: 2023/64, decision code: 03/09, 27/02/2023. The study was conducted in accordance with the principles of the Declaration of Helsinki. A written informed consent was obtained from each patient. The study included surgically treated patients aged 65 and above with proximal femur fractures, totaling 346 participants. Exclusion criteria encompassed pathological, periprosthetic, and non-specific undisplaced avulsion fractures of the greater trochanter.
Patients were divided into two cohorts: those treated in the pre-COVID era (n = 175), defined as January 1, 2018, to March 26, 2020, and those treated during the COVID era (n = 171), defined as March 27, 2020, to December 12, 2021. The onset of the COVID era was determined as March 27, 2020, marking the date of official regional and hospital operational changes. December 12, 2021, signifies the date when we officially resumed routine operations.
Data were extracted from the hospital’s electronic medical records system. Variables such as age, gender, activity level before fracture, trauma type, diagnosis, treatment type, ICU admission and duration, revision surgery, comorbidities, time to surgery, COVID-19 status, surgical duration, mortality within 1, 3, 6, and 12 months, causes of death, time until death (if occurred), and comorbidities were collected.
Statistical Analysis
Descriptive statistics were employed for all variables. The independent samples t test and Chi-square tests (or Fisher’s exact test) were used for comparisons between the pre-COVID and COVID era cohorts. A p value of less than 0.05 was considered statistically significant.
Survival probabilities were assessed using Kaplan-Meier, while multivariate analysis identified mortality predictors, estimating odds ratios and 95% confidence intervals. Surgery delay impact on 1-year mortality was measured using the Hazard Ratio. Statistical analyses used R (v4.2.1) and SPSS (v15).
Result
Demographic and Clinical Characteristics of Patients Operated for Hip Fractures.

Note. Age are presented as median and interquartile range (IQR) values. Statistical values include z-test or chi-squared test results; P indicates the significance level. *: Fisher’s exact test. +: Post-op Covid (+) patients before discharge. PFNA: proximal femoral nail antirotation.
Operative Details and Post-Operative Outcomes for Patients.
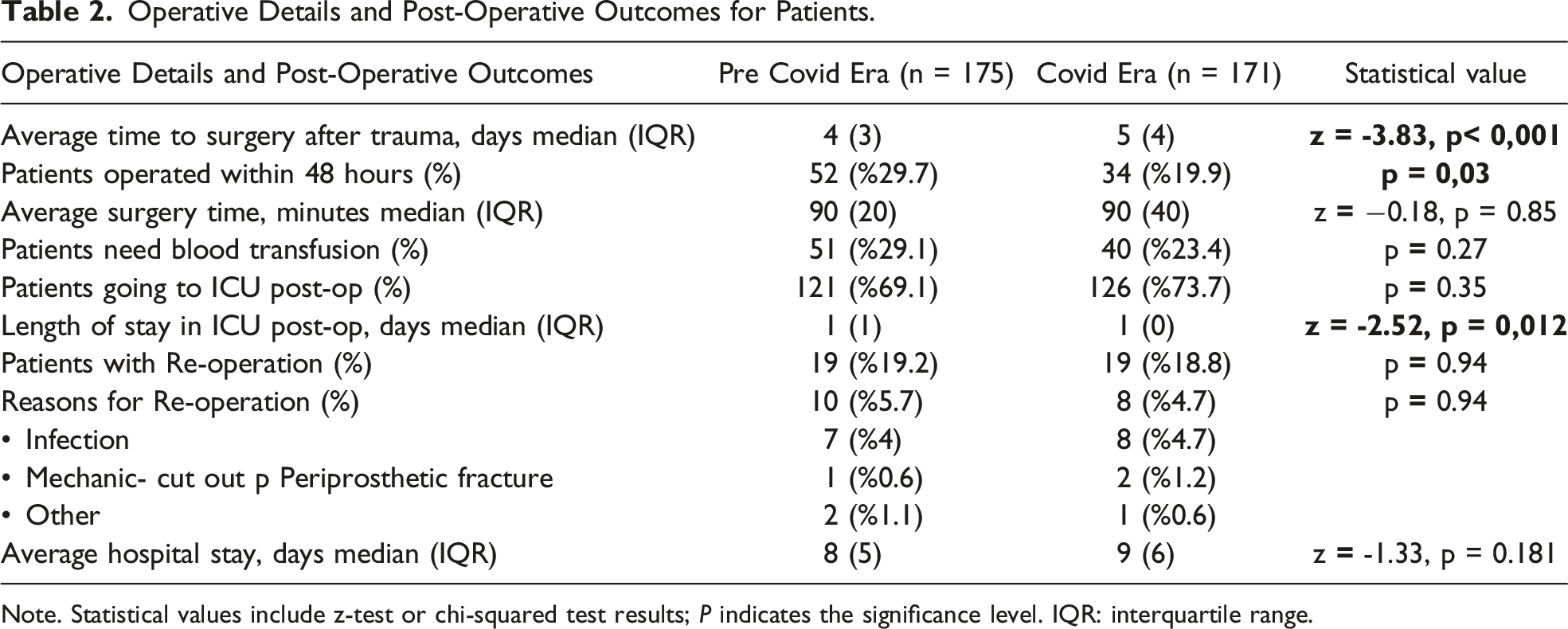
Note. Statistical values include z-test or chi-squared test results; P indicates the significance level. IQR: interquartile range.
Mortality Rates, Comorbid Conditions, and Causes of Death in Pre-covid and Covid Group.

Note. Statistical values include z-test or chi-squared test results; p indicates the significance level. IQR: interquartile range.
Mortality Rates Over Time
In the pre-COVID group, the cumulative mortality rates at 1, 3, 6, and 12 months were 13.7%, 34.9%, 44%, and 49.1%, respectively. During the COVID era, these rates were 11.7%, 30.4%, 39.8%, and 43.9% for the same intervals (respectively p = 0.537, p = 0.852, p = 0.462, p = 0.325).
During both the pre-COVID and COVID eras, a significant proportion of deaths, 71% and 69.2% respectively, occurred within the initial 90 days. Overall, throughout the entire study period, 70.1% of the deaths within the first year also occurred within the first 90 days.
Considering the total era, both pre-COVID and COVID, the cumulative mortality rates at 1, 3, 6, and 12 months were 12.7%, 32.7%, 41.9%, and 46.5%, respectively.
Mortality Rates and COVID Test Results in COVID Era
During the COVID era, out of 171 patients, 160 tested negative for COVID, and 11 tested positive. Of these 11 patients, 4 were COVID-positive before the operation, while 7 tested positive in the pre-discharge period after the surgery. The cumulative mortality rates for COVID-positive patients at 1, 3, 6, and 12 months were 0%, 36.4%, 54.5%, and 54.5%, respectively. During the same period, the cumulative mortality rates for COVID-negative patients at 1, 3, 6, and 12 months were 12.5%, 30%, 38.7%, and 43.1%, respectively. However, no significant difference was detected in the mortality rates between COVID-negative and COVID-positive patients at 1, 3, 6, and 12 months (p = 0.226, p = 0.852, p = 0.462, p = 0.587).
Multivariate Analysis of Factors Influencing Mortality in the Pre-COVID and COVID Eras.

Note. OR, Odds Ratio; CI, Confidence Interval.
Time to Surgery and Mortality
In the pre-COVID era, no statistical link could be established between the length of time patients waited before undergoing surgery and mortality (p = 0.246). However, the situation markedly shifted during the COVID era, where each additional day a patient waited before surgery significantly impacted the 1-year mortality rate (Hazard Ratio = 1.146, 95% CI: 1.073-1.223, p < 0.01). In other words, during the pandemic, delaying surgery by 1 day increased the 1-year mortality rate by 14.6%.
Considering all patients, including both pre-COVID and during-COVID eras, each additional day waited before undergoing surgery also significantly affects the 1-year mortality rate (Hazard Ratio = 1.101, 95% CI: 1.044-1.162, p < 0.001). This overall trend suggests that delaying surgery by 1 day increases the 1-year mortality rate by 10.1%.
One-Year Survival Rate Over Time
The 1-year survival rate is 53.8% according to the Kaplan-Meier test. In the pre-COVID patient group, the 1-year survival rate is 50.9%, while the survival rate of patients during the COVID era is 56.1%. There was no statistical difference in terms of 1-year survival between the pre-COVID and COVID-era patients, as shown in Figure 1 (p = 0.3). In Figure 2, the comparison of 1-year survival rates between COVID-positive and COVID-negative patients is shown. A significant difference was not shown between 1-year survival rates among COVID-positive and COVID-negative patients, p = 0.587. Comparison of one-year survival rates between the pre-COVID and COVID-era patients using kaplan meier analysis. Comparison of one-year survival rates between COVID positive and COVID negative patients using kaplan meier analysis.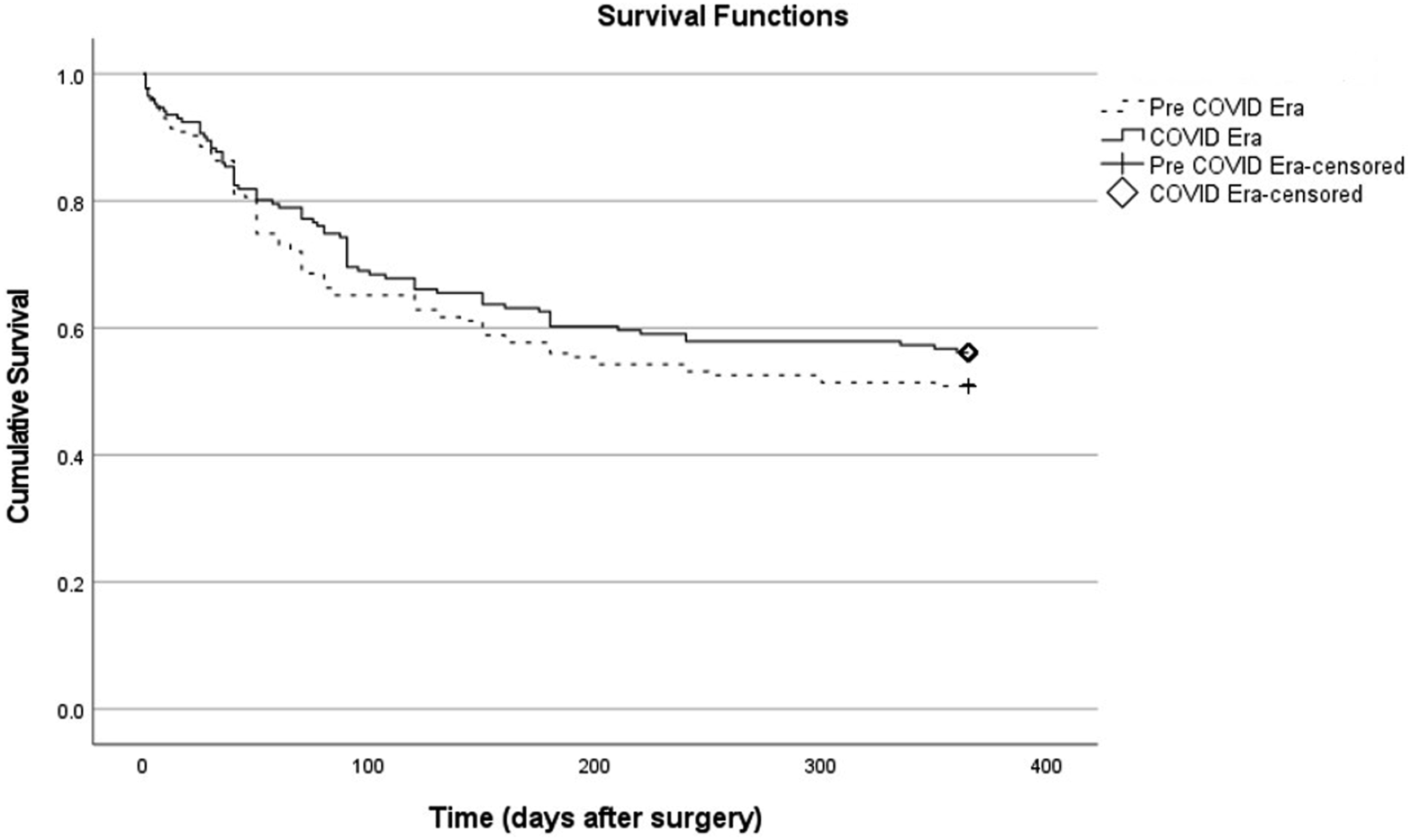

Surgery Timing and Survival Rates
The 1-year survival rate for patients who underwent surgery within 48 hours of hospital admission is 60.5%, while for those who had surgery after 48 hours, it’s 51.2%. Upon examination of the 1-year survival rate with the Kaplan-Meier test, a statistically significant difference was found between patients who underwent surgery within the first 48 hours and those who did not (Breslow p = 0.031, Tarone-Ware p = 0.044, Figure 3). Comparison of one-year survival rates for who underwent within 48 hours patients using kaplan meier analysis.
Impact of ICU Admission on Survival Rates
In the pre-COVID era, patients without ICU admission post-surgery had a 1-year survival rate of 74.1%, while those with ICU admission had 40.5%, as per Kaplan-Meier analysis. In the COVID era, ICU-avoidant patients showed a 1-year survival rate of 75.6%, contrasting with 49.2% for ICU-admitted patients (Figure 4). Between both eras, no significant difference was detected in ICU groups (p = 0.18). Comparison of one-year survival rates based on intensive care requirement using kaplan meier analysis.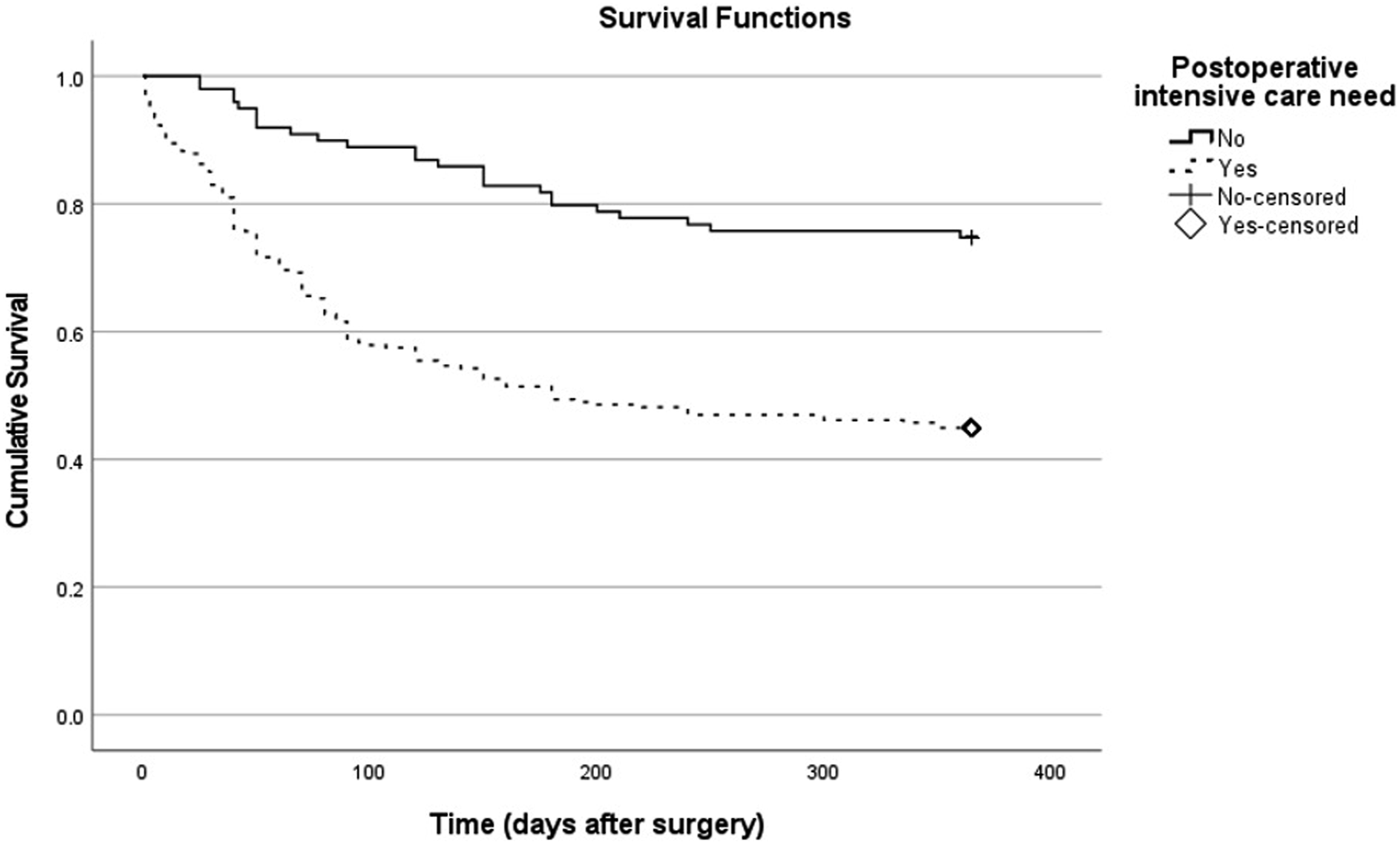
Overall, the 1-year survival rate was notably higher for patients who didn’t need post-op ICU care compared to those who did. Kaplan-Meier survival analysis showed 74.7% of patients avoiding ICU (74/99) were alive after 1 year, against 44.9% in the ICU group (111/247). This survival rate difference was statistically significant, as shown by the Log-rank test (χ^2 = 26.372, p < 0.001). Median survival for ICU patients was 180 days (95% CI, 43.8-316.2 days). Median survival for the non-ICU group couldn’t be presented, as over 50% were alive after 1 year, leading to a censored median survival. Mean survival for the entire cohort was 234.4 days (95% CI, 218.6-250.2 days). These results suggest not needing ICU post-hip fracture surgery is linked to higher 1-year survival chances. Out of 346 patients, 161 experienced death, and 185 were censored, with an overall event occurrence of 53.5%.
Discussion
Comparison of Mortality Rates in Pre-COVID and COVID Eras
In this study, the 30-day mortality rates was 13.7% in the pre-COVID era and dropped to 11.7% during the COVID era (p = 0.573). In the literature, pre-COVID studies show that 30-day mortality rate varies between 7%–10%, while during the COVID era it varies between 16.3% and 33.3%. According to these data, our 30-day mortality rate in the pre-COVID era is higher than the mortality rates in the literature. However, this rate has dropped to 11.7% during the COVID era and has remained lower compared to the mortality rates in the literature.17,22,23 This situation can be explained by the fact that COVID-19 cases in Türkiye started to appear later compared to other countries where similar studies were conducted. This delay provided the necessary time for our hospital to prepare and make the required arrangements. The lower rate of mortality in the COVID era could also be attributed to a decrease in the number of elective surgeries and closer postoperative monitoring of trauma cases.
It is explained that 1 of the reasons for the high 1-year mortality rate (46.5%) is that our hospital is the only large, well-equipped hospital in the region. All patients with comorbidities and additional problems from surrounding provinces are referred to our center. Due to the limited capacity of the intensive care unit, these patients often have to wait a long time for surgery. Consequently, only a very small number of patients can be operated on within the first 48 hours, which leads to higher mortality rates compared to the literature.
In our study, the 1-year mortality rate was found to be 49.1% in the pre-COVID era, which was decreased to 43.9% during the COVID era, p = 0.325. The fact that there is only a 1-day difference in pre-operative waiting time between the pre-COVID and COVID periods can be cited as a reason for the lack of a significant change in mortality rates. In the literature, the 1-year mortality rate for patients with hip fractures in the pre-COVID era varies between 14%–40%.5,8,9 Nevertheless, a downward trend in this rate was observed during the COVID era in this study. Our higher pre-COVID mortality could be attributed to fewer early surgeries (29.7% within 48 hrs), more comorbidities (92.6% with ≥1), and increased ICU needs (69.1% pre-COVID, 73.7% COVID) vs other centers.
A notable point in our study is that the majority of deaths occurred within the first 90 days. In this study, 71% of the deaths during the pre-COVID era, 69.2% during the COVID era, and 70.1% in the entire period occurred within the first 90 days. There is no data available that could explain or relate to this situation in this study.
Mortality Rates in COVID-19 Positive and Negative Patients
The overall 30-day mortality rate was 11.7% during covid era in our study. Specifically, we observed no deaths among COVID-19-positive patients (0% mortality), while the mortality rate among COVID-19-negative patients was 12.5%. Over a 90-day period, the total mortality rate was 11.7%. The mortality rate among patients who were COVID-19 positive was 36.4%, while the mortality rate among COVID-19-negative patients was 30%.
In a retrospective study by Karayiannis et al 24 , 484 patients were studied, and among the 27 COVID-19 positive patients, 4 had died, leading to a 30-day mortality rate of 14.8%. Similarly, in a prospective study conducted by Egol et al 25 with 124 patients, 9 out of the 17 COVID-19-positive patients with hip fractures had died, resulting in a 30-day mortality rate of 52.9%.
In three separate retrospective studies conducted by Mamarelis et al, Ward et al and Kayani et al, involving 31, 124 and 442 patients respectively, the 30-day mortality rates for patients with proximal femoral fractures who were COVID-19 positive were reported to be 54.4%, 37% and 30.5% respectively.26-28
In comparison to those studies, this study demonstrates that during the COVID era, lower early-stage mortality rates were observed. This can be attributed to Türkiye encountering COVID at a later stage than other countries where these investigations were conducted, allowing ample time for adequate preparations to be made. Prolonged curfews for individuals aged 65 and above can contribute to this situation. The absence of any deaths in the first 30 days among the 11 COVID-positive patients can be explained by the relatively low number of COVID-positive patients. Furthermore, there was no significant reduction in personnel numbers, and the emphasis was placed on trauma patients by canceling elective surgeries, which serves as another contributing factor.
Unlike these studies, our research also provides information about the mortality rates of patients over a longer duration at 3, 6 months and 1 year. The cumulative mortality rates for COVID-positive patients at 3, 6 and 12 months were 36.4%, 54.5% and 54.5%, respectively. Meanwhile, for the same periods, the cumulative mortality rates for COVID-negative patients were 30%, 38.7% and 43.1%, respectively (p = 0.852, p = 0.462, p = 0.587).
Comparing the data from our study to the findings in the study by Hall et al, which reports 1-year mortality rates in the literature, reveals both similarities and differences in the impact of COVID-19 on 1-year mortality rates for hip fracture patients. 29 In our study, the overall 1-year mortality rate was 46.5%. For COVID-19 positive patients, the 1-year mortality rate was 54.5%, while for COVID-19 negative patients, it was 43.1%. Conversely, Hall et al reported a significantly higher 1-year mortality rate for COVID-19 positive patients at 46.5% compared to 27.2% for COVID-19 negative patients, indicating a 2-fold increase in mortality risk associated with COVID-19. However, in our study, no such statistical increase was observed. This discrepancy could be attributed to Hall’s study covering a 2-month period during the initial United Kingdom COVID-19 surge, whereas our study spans a broader timeframe.
Impact of Surgical Timing on Mortality Rates
In a comprehensive meta-analysis encompassing 16 studies, Nikol et al highlighted that early surgical intervention leads to a 45% reduction in the 1-year mortality rate. 9 Similarly, in our study, the 1-year survival rate for patients who underwent surgery within 48 hours of hospital admission is 60.5%, while for those who had surgery after 48 hours, it’s 51.2%. There was a 19% reduction in mortality with early surgery.
In the study conducted by Mattison and colleagues, they reported that a delay of 36 hours for surgery resulted in a 31% increase in 1-year mortality rate. 8 In the study conducted by Toshiya et al, it was determined that a delay of 48 hours in surgery led to a 32% increase in the 1 year mortality rate. 10 In our study, it was observed that an additional 24 hours delay in surgery during the COVID-19 era escalated the 1-year mortality rate by 14.6% (Hazard Ratio = 1.146, 95% CI: 1.072-1.223, p < 0.001). During the pre-COVID era, no such correlation was identifiable. However, across all periods encompassing both pre-COVID and COVID eras, an additional 24 hours delay in surgery corresponded to a 10.1% increase in the annual mortality rate (Hazard Ratio = 1.101, 95% CI: 1.044-1.162, p < 0.001).
As shown in both the literature and our study, hip fractures should be operated on as soon as possible, ideally within the first 48 hours. Early surgery is important to minimize the pain experienced by patients and to reduce mortality rates. However, unfortunately, due to operational reasons, high demand, and our hospital being the only central hospital in the region, the proportion of patients operated on within the first 48 hours is low.
Impact of ICU Admission on Survival Rates
In patients with hip fractures, a factor not mentioned in other studies emerged in this study that affects survival rates. Admission to the ICU appears to significantly affect survival rates, with a higher 1-year survival rate observed for patients who did not require ICU admission post-surgery in both the pre-COVID and COVID eras. A similar number of patients entered post-op intensive care in the pre-COVID and COVID eras. The 1-year survival rate for patients who did not go to the ICU in the pre-COVID, COVID, and total era were as follows: 74.1%, 75.6%, and 74.7%, respectively. The survival rates for patients who went to the ICU are 40.5%, 49.2%, and 44.9% respectively (Log Rank p < 0.001, p = 0.001, p < 0.001).
In our study, several limitations were encountered. Firstly, the study was retrospective and not randomized. The number of COVID positive patients included in our study was relatively small compared to the population (6.4%). Additionally, patient compliance with postoperative care, socioeconomic status, and access to healthcare facilities, were not included in the analysis, which could be crucial for the study. Another limitation is that our study did not include the reasons for the waiting times and why patients required intensive care at such a high rate.
The IMPACT Protect study by Andrew J. Hall et al 30 has demonstrated that vaccination against COVID-19 significantly reduced the mortality risk for COVID-positive hip fracture patients and underscore the importance of vaccination in mitigating the severity of infection and reducing mortality rates in this vulnerable patient group. However, our study lacks sufficient data on this subject, and due to the multiple types of COVID vaccinations administered in our country, this aspect is inadequate in our paper.
To address current limitations and better understand the factors influencing mortality rates, future research should prioritize larger sample groups and ICU, comprehensive data on post-hospital care and follow-up.
Conclusion
The mortality rate of geriatric hip fractures remains high both before and during the COVID-19 pandemic and COVID positive patients. Operational changes during the COVID period caused a 1-day delay in the waiting process for surgery, and there was no significant change in mortality rates between the pre-pandemic and pandemic periods. The findings emphasize the importance of pandemic preparedness and prompt surgeries and attentive ICU care in reducing mortality rates. Notably, postoperative mortality rates were particularly significant within the first 90 days, warranting close monitoring during this period.
Footnotes
Acknowledgments
We would like to thank Cem Çopuroğlu, Mert Özcan, and Mert Çiftdemir for their significant contributions to this study.
Author Contributions
Idea/concept and design: E.S.; Data collection and/or processing: M.E., O.M.; Control/supervision and analysis and/or interpretation: E.G.S.; Literature review: E.S., M.E.; Writing the article: E.S. Critical review: E.S., M.E., References and fundings: E.G.S, M.E.; Materials: E.G.S., O.M.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.