
Abstract
Introduction:
Comanagement of hip fractures is thought to optimize outcomes for these high-risk patients, but this practice is not universal. We aimed to determine whether comanagement of patients with hip fracture affects 30-day outcomes.
Methods:
The American College of Surgeons National Surgical Quality Improvement Program database was queried for all hip fractures between January 2015 and January 2017, totaling 15 461 patients (144 hospitals). Patients were divided into 3 cohorts: 11 233 comanaged throughout stay (CM), 2537 partially comanaged during stay (PCM), or 1691 not comanaged (NCM), by orthopedic surgeons with medicine physicians or geriatricians. Data collected included demographics, hip fracture type, postoperative outcomes, and length of stay (LOS). Logistic regression and linear regression analyses were performed.
Results:
Both CM and PCM patients were older, with more dementia, poorer mobility, and more comorbidities than NCM patients. Mortality rates were 4.55%, 0.81%, and 0.33% for CM, PCM, and NCM, respectively, and risk-adjusted odds ratios (ORs) were 1.63 (95% confidence interval = 1.22-2.23) and 1.22 (0.87-1.74) for CM and PCM, respectively, compared to NCM. Morbidity rates were 11.06%, 15.45%, and 7.63% for CM, PCM, and NCM, respectively, and ORs were 1.74 (1.41-2.16) and 1.94 (1.57-2.41) for CM and PCM, respectively, compared to NCM. Risk-adjusted mean square LOS was 6.38, 8.80, and 7.23 for CM, PCM, and NC, respectively (P < .01).
Conclusions:
Comanaged patients with hip fracture had poorer cognition, function, and general health, with the shortest LOS. Surprisingly, NCM was associated with reduced morbidity and mortality, which may relate to them being the healthiest patients. Overall, our findings still support orthogeriatric comanagement in this high-risk group to maximize outcomes.
Introduction
Hip fractures are common injuries with significant associated morbidity and mortality. 1,2 The risk of osteoporotic hip fracture increases with age, 1,2 and in an aging population, the incidence and associated disability are also likely to increase. The number of hip fractures is projected to exceed 500 000 per year in the United States by 2040. 3 In addition, hip fractures are associated with excess mortality for 5 to 10 years postinjury, 4 with a 20% mortality rate at 1 year. 5 The reasons for this excess mortality are likely related to the presence of comorbidities 6 and complications following fracture, 7,8 which also contributes to the loss of mobility and need for nursing care. Despite medical and surgical management, often focused on these risk factors, the mortality rate remains high. 9
Nevertheless, it is crucial to continue to try to optimize the care of these high-risk patients. Perioperative management has traditionally been performed by orthopedic surgeons, yet with the comorbidities and complications of hospitalization, medicine physicians or geriatricians may be better suited to provide care outside of fracture surgery. Comanagement of hip fractures between orthopedic surgeons and geriatricians was first developed in England, 10 where it has been successful along with other countries in reducing complications, 11 -13 time to surgery, 10,11 length of stay, 11,14 mortality, 12 -15 readmission, 13 dysfunction, 3 and the need for higher levels of care following discharge. 15 The preoperative optimization and postoperative care of these frail patients have also been shown to reduce mortality and costs. 16 In fact, national guidelines in the United Kingdom recommend routine geriatric care for these high-risk patients, 17,18 and hospitals are incentivized to provide this alongside other markers of care (Best Practice Tariff) with performance recorded in the National Hip Fracture Database. The United States has a very different health-care system, and comanagement is now being increasingly adopted as a universal practice. Hip fractures have recently been targeted by the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP), 19 following the path of other countries with more established national hip fracture databases, and thus fueling a drive to standardize care, improve outcomes, and reduce costs when managing these patients. 1
To our knowledge, no studies have examined the effect of comanagement of hip fractures on a national scale in the United States. The primary aim of this study is to determine whether comanagement of patients with hip fracture affects 30-day mortality. The secondary objective is to determine the influence of comanagement on outcomes such as morbidity, length of stay, and readmission.
Methods
This was a retrospective analysis of prospectively collected data in the NSQIP database of sampled surgical patients aged 18 years or older. The NSQIP is a nationally validated, risk-adjusted, outcomes-based program implemented to improve surgical care. 19 The database was queried for all adult patients (>18 years of age) with a hip fracture between January 2015 and January 2017. Patients with missing data on comanagement or other critical hip fracture data were excluded. All other standard NSQIP variables and outcomes are not permitted to be missing as an inherent requirement of the database. Typically, there is a very low level of incompleteness.
Patients were divided into 3 cohorts according to the amount of comanaged care received during their inpatient stay: comanagement throughout stay (CM), partial comanagement during stay (PCM), and no comanagement (NCM). Patient comanagement was defined as joint care of an orthopedic surgeon with medicine physicians or geriatricians. Partial comanagement occurred when there was joint patient care for at least 1 day but not the full hospital course. Data collected included standard ACS NSQIP baseline characteristics, the type of hip fracture surgery, postoperative outcomes, and length of stay. Outcomes measures such as length of stay, morbidity, discharge destination, and the 30-day mortality, readmission, and reoperation rates were also collected.
Statistical analysis was completed using SAS 9.4 (SAS Institute Inc, Cary, North Carolina). The 3 comanagement cohorts were first compared with respect to preoperative risk factors and unadjusted postoperative event rates and length of stay; P values for associations between risk factors and group were addressed using chi-square statistics or regression for continuous variables, either without or with adjustment for hospital clustering. Length of stay was estimated using linear regression with comanagement type plus 5 NSQIP variables for risk adjustment. Least square means and standard deviations for comanagement groups were reported, and (Tukey-Kramer) pairwise P values of ≤.05 were considered statistically significant. Logistic regression, with and without adjustment for clustering, was used to assess the effects of comanagement on mortality and morbidity using guided (forward) selection of NSQIP predictor variables (17 for mortality and 16 for morbidity).
Results
Of 16 126 patients with hip fractures from available records, 665 were excluded because of missing comanagement or other critical hip fracture variables. We examined 15 461 patients, from 144 hospitals, who were either CM (n = 11 233), PCM (n = 2537), and NCM (n = 1691). Hospitals tended to use comanagement styles differentially. The average hospital-level percentage of NCM patients was 12%, but 58 of the 144 hospitals had ≤1% NCM patients. The average hospital-level percentage of PCM patients was 13%, but 51 of the 144 hospitals had ≤1% PCM patients. The average hospital-level percentage of CM patients was 75%, but 54 of the 144 hospitals had ≥95% CM patients.
Differences between CM, PCM, and NCM groups in baseline characteristics are shown in Table 1. Without adjustment for clustering, there were significant differences in all criteria apart from 2 comorbidities, stroke (P = .07) and chronic kidney disease (P = .07). There were fewer differences in baseline characteristics with adjustment for the clustering of cases within hospitals. Cephalomedullary nailing was the most commonly performed surgery type, followed by hemiarthroplasty, sliding hip screw, and total hip arthroplasty in all cohorts (Table 2).
Baseline Characteristics (Percentages or Mean and Standard Deviations) Using ACS NSQIP Definitions for CM, PCM, and NCM Groups.

Abbreviations: ACS NSQIP, American College of Surgeons National Surgical Quality Improvement Program; ASA, American Society of Anesthesiology; BUN, blood urea nitrogen; CM, comanagement; PCM, partial comanagement; NCM, no comanagement.
a Without adjustment for clustering.
b With adjustment for cluster sampling.
Bold face values indicate P value < 0.05.
Surgery Type for All Patients (Percentages Using ACS NSQIP Definitions for CM, PCM, and NCM Groups).

Abbreviations: ACS NSQIP, American College of Surgeons National Surgical Quality Improvement Program; CM, comanagement; NCM, no comanagement; PCM, partial comanagement.
a Ordinary chi-square.
b Rao-Scott chi-square (includes adjustment for cluster sampling).
Bold face values indicate P value < 0.05.
Table 3 shows unadjusted lengths of stay were lowest in the CM cohort at 5.37 days, followed by NCM at 6.04 days, and PCM at 7.92 days (P < .01). Table 3 also shows unadjusted postoperative outcomes, where each category is significantly different apart from reoperation <30 days (P = .18) and renal failure (P = 006). Specifically, the mortality rates were 4.55%, 0.81%, and 0.33%, and the morbidity rates were 8.03%, 2.54%, and 0.83% for CM, PCM, and NCM respectively. The mean length of stay with linear regression with clustering adjustment was lowest in the CM, followed by the NCM and PCM cohorts (Table 4). Table 5 shows increased odds ratios (ORs) for mortality and morbidity of CM and PCM compared to NCM.
Raw Outcomes (Percentages or Mean and SD), Using ACS NSQIP Definitions, for CM, PCM, and NCM Groups.
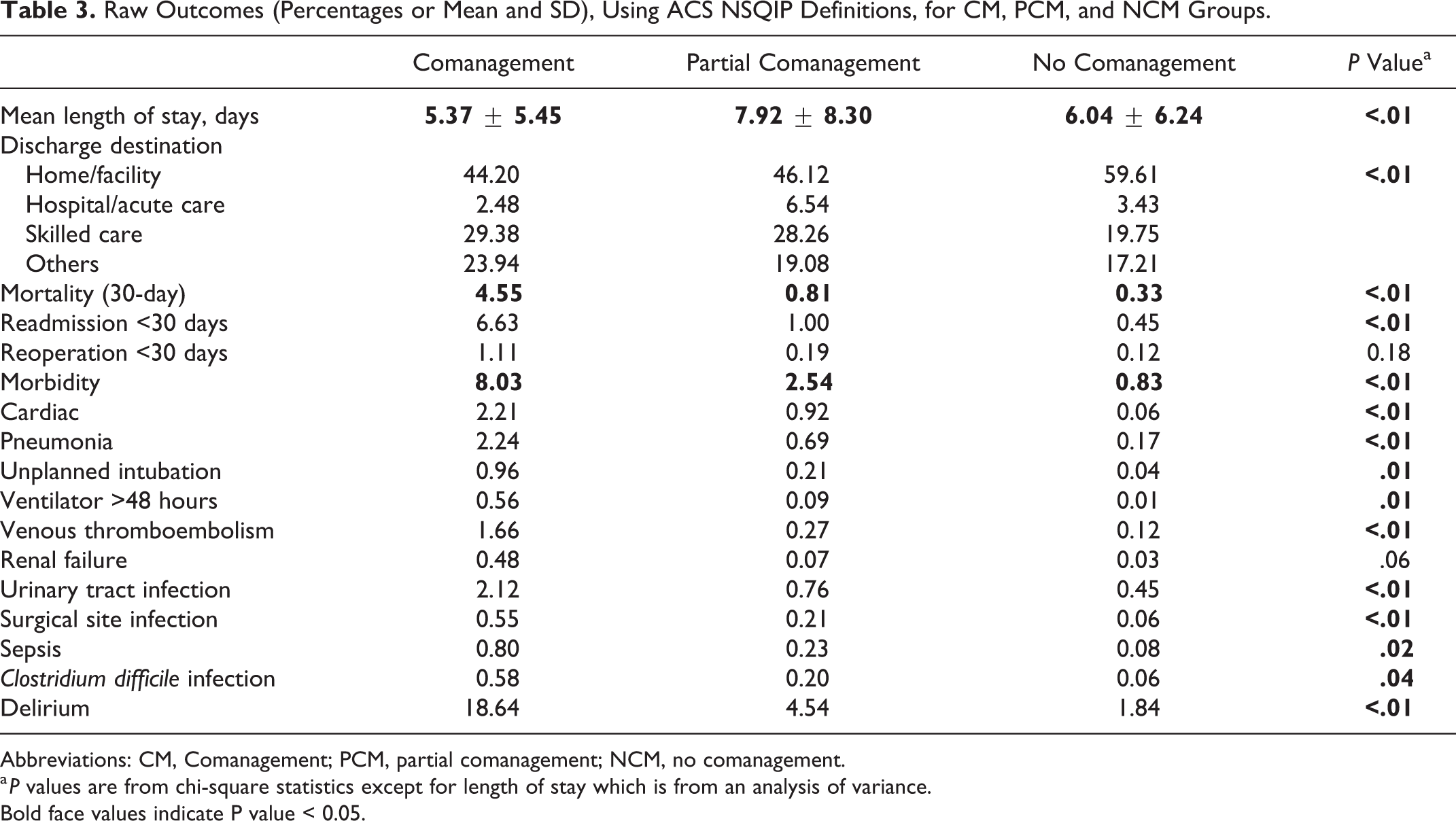
Abbreviations: CM, Comanagement; PCM, partial comanagement; NCM, no comanagement.
a P values are from chi-square statistics except for length of stay which is from an analysis of variance.
Bold face values indicate P value < 0.05.
Risk-Adjusted Least Square Mean Lengths of Stay (standard error).
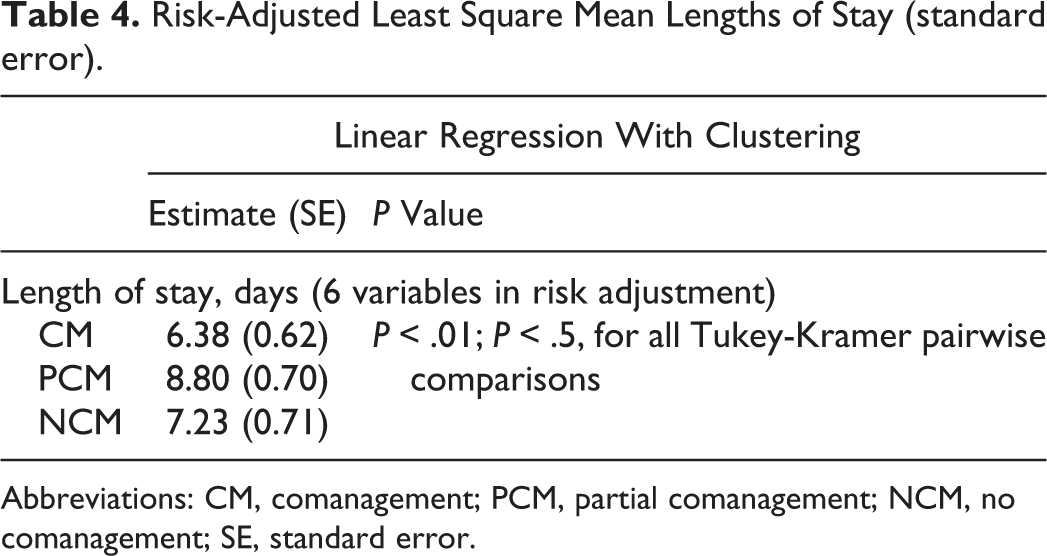
Abbreviations: CM, comanagement; PCM, partial comanagement; NCM, no comanagement; SE, standard error.
Mortality and Morbidity Odds Ratios (confidence intervals) Associated With Comanagement Status.
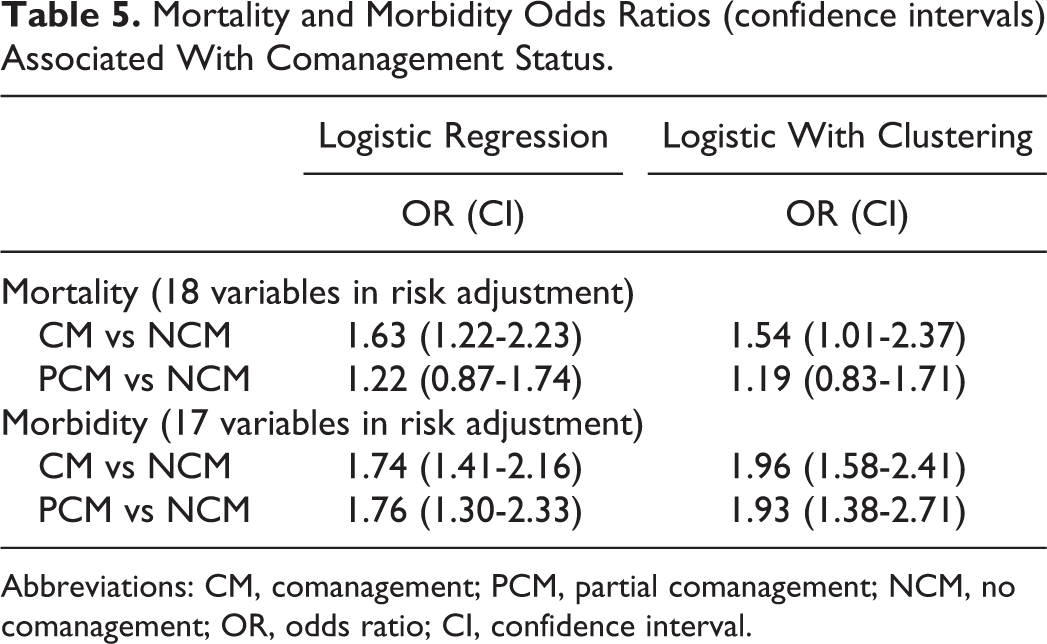
Abbreviations: CM, comanagement; PCM, partial comanagement; NCM, no comanagement; OR, odds ratio; CI, confidence interval.
Morbidity rates were 8.03%, 2.54%, and 0.83% for CM, PCM, and NCM, respectively, and ORs were 1.74 (1.41-2.16) and 1.936 (1.58-2.41) for CM and PCM, respectively, in comparison to NCM.
Discussion
Hip fractures are associated with significant morbidity and mortality. They commonly occur in elderly comorbid patients and, as such, geriatricians are more suited to provide pre- and postoperative care. As a result, comanagement between orthopedic surgeons and geriatricians has evolved but is not yet standard care in the United States, despite immense potential benefits in outcomes and costs. In the largest study of its kind, we analyzed a national database and found that CM patients had the lowest length of stay compared to PCM and NCM patients. Patients with PCM had the highest length of stay, and interestingly, NCM was associated with reduced morbidity and less so for mortality.
Evidence for comanagement has been emerging in the United States more recently, with authors recommending an interdisciplinary approach. 3,6,20,21 Friedman et al described a model of comanaged care of older patients with hip fractures in Rochester, New York, with protocol-driven geriatrician-led care, and early discharge planning. They found shorter time to surgery, lower mortality, complications, length of stay, and readmissions. The same authors demonstrated improvements in all parameters and costs in 758 patients. 21 Gosch et al examined comanagement of hip fractures in 265 long-term care residents who are an especially high-risk group. They found improved outcomes and a lower mortality than comparable cohorts, with possible benefits of improved function and reduction in future fracture risk. 9
All 3 cohorts were found to have significantly different preoperative risk factors. Although patients with hip fracture are considered high risk, as they are generally older adults with varying number and severity of comorbidities, these differences may account for the results seen in this study. Specifically, CM and PCM patients were almost 5 years older than the NCM patients who were also more independent and had less dementia than the other cohorts. The CM patients had significantly more abnormal platelet counts, blood urea nitrogen, and albumen levels, with almost all comorbidities being more significantly more common in the CM cohort and to a lesser magnitude the PCM cohort, compared to the NCM cohorts. The NCM patients had lower American Society of Anesthesiology (ASA) grades and, combined with the aforementioned, suggests that they were significantly healthier in terms of function, cognition, and comorbidities. Multiple studies have shown that these parameters influence morbidity and mortality after hip fracture surgery. 4,5,7,8 Comorbid conditions must be managed alongside their fracture and can often place these patients at risk of delirium, infection, and surgical complications from hip fracture surgery. 3 Geriatricians are well suited to identify comorbidities and manage them in the perioperative period to maximize patient outcomes. 21
In this study, mortality rates were highest in the CM group, followed by PCM and NCM. At first glance, this is contrary to that expected for patients being comanaged by medicine physicians and geriatricians. Indeed, Fisher et al examined 951 hip fractures with historical controls and found a significant reduction in mortality from 7.7% to 4.7% with CM. 13 However, previous studies have found that the influence of CM on mortality may not be so positive, especially in the short term. In a case–control study of 291 patients with hip fracture, CM was found not to influence in-hospital mortality and 3 months but only at 6 and 12 months. 22 Biber et al also found no difference with in-hospital mortality in a cohort study of 114 patients at a geriatric fracture center. 11 Others have found a non-significant reduction in mortality. 2,16 Various explanations may account for this finding, including older, frailer, and more comorbid patients with hip fracture being more likely to be admitted to centers that have CM or have the option for PCM. Even if they present to smaller centers with less resources, patients may be transferred out. This may result in healthier patients being managed in these centers with NCM. In addition, heterogeneity in the criteria used to assign CM, and the CM options itself, may limit conclusions.
In the United States, the American Academy of Orthopedic Surgeons (AAOS) has published guidelines (2014) on managing hip fractures in the elderly individuals. 23 However, in the United Kingdom, the “Blue Book” contains more established national standards of care, with specific description of what CM entails. 18 In addition, unlike the United States, there is incentivization for hospitals in the United Kingdom to adhere to these guidelines for financial reward, but also good publicity when performing well, as results are available for public access. That being said, Patel and coworkers found a nonsignificant reduction in mortality at 30 days before and after the introduction of national CM guidelines in the United Kingdom. 2 As compliance and experience with CM continues to improve, there will inevitably be less heterogeneity in care and better outcomes. For example, universal CM in geriatric fracture center (>70 years) has led to equivalent mortality rates between patients with hip fracture and non-hip fracture patients. 9 The benefits of CM appear to be clearer with higher levels of evidence such as a randomized trial of 319 CM patients with significantly lower inhospital mortality 12 and a meta-analysis of 9094 patients with a significant reduction in in-hospital (relative risk 0.60) and long-term mortality (relative risk 0.83). 23
The morbidity outcome rate was highest in the PCM patients in our study. This may be explained by comanagement being used only when patients become unwell or a sign of less organized care, thus warranting a medicine or geriatrician consult who then presumably continue to care for the patient alongside the orthopedic surgeon. As noted earlier, these are high-risk patients, and such reactive management with medical or geriatric care-initiated part way through their stay, when it may be difficult and take longer to address any medical issues, may account for the higher morbidity rate. Interestingly, patients with no comanagement had the lowest morbidity outcome score. This may relate to these patients being relatively healthy patients, thus being more likely to be treated in larger centers with medicine or geriatric input available or simply not needing such input. However, this does not fully explain our findings. Although there are benefits of comanagement including reducing complications, morbidity, mortality, 12,13 and costs, 24 heterogeneity in the implementation and components of a comanagement model may explain this and some of the lack of positive outcomes seen in the literature. 23 For example, Naglie et al failed to show any significant differences in outcomes at 3 and 6 months, 25 which may a result of the variation in care components delivered. 25 Indeed, the authors suggested that inappropriate targeting of patients, who should not be too well or unwell to gain maximum benefit, and an underpowered study as reasons behind this.
The length of stay was lowest in CM patients in our study. Aside from mortality, length of stay was one of the 12 selected parameters to evaluate comanagement for hip fractures, 26 suggesting a faster postoperative course to discharge with less complications. Prior studies have shown reduction in length of stay with medical comanagement. 2,6,10 -12,16,22,23 In a randomized controlled trial of hip fractures with either multidisciplinary (n = 155) or standard (n = 164) care, Vidan et al found the length of stay way 2 days shorter in the comanagement group (P = .06). 12 A systematic review and meta-analysis of 18 studies and 9094 patients showed a 'shared care' model significantly reduced length of stay, 23 and other groups have found reductions in up to 6.3 days (P < .01). 16 Interestingly, we showed that PCM had the highest length of stay which may be explained by patients becoming unwell postoperatively, requiring geriatric hospitalist input to start, thus increasing the length of stay. Related to this, there are studies that have shown equivalent 13 or higher lengths of stay, such as that by Prestmo and colleagues in the 198 patients randomized to receive geriatric care, compared to the 199 patients receiving orthopedic care. 20 This may be accounted for by the greater number of patients being discharged home and thus needing more complex care coordination. Another randomized controlled trial of 279 patients examined interdisciplinary versus standard postoperative care for hip fractures also showed a higher length of stay by 8.3 days (P < .01). 25
As comanagement is inherently a value-added process, one would intuitively expect CM and PCM to be protective for risk-adjusted rates of mortality and morbidity, compared to NCM. In this study, the observation that NCM was associated with the lowest risk-adjusted rates of mortality and morbidity could be attributed to at least 2 factors. First, there might be underlying hospital effects that had not been accounted for. The availability of, and allocation to, comanagement groups varied by hospital so that some hospitals are predisposed to assign or not assign most (or all) patients to a single group, regardless of patient characteristics. In addition, hospitals may differ with respect to hip fracture treatment quality regardless of comanagement condition. These issues could degrade the adequacy of logistic, or a potential propensity-score-based, risk adjustment. Second, assignment to PCM is likely to be influenced by the actual occurrence of a postoperative morbidity event, where some patients may be moved from NCM to PCM. This might have several consequences including: (1) NCM will have better outcomes than predicted because patients with events are removed from the group; (2) PCM will have worse outcomes than predicted because it has patients from the NCM group who experienced the event; and (3) CM patients may have worse outcomes than NCM because the CM group cannot move patients out, as is the case for NCM.
This study has limitations, many of which are inherent to database studies of this nature. First, this observational study may be limited by a lack of NSQIP database robustness, such as issues with underlying hospital effects and comanagement availability/allocation, as noted earlier. Nevertheless, we used statistical analyses (eg, propensity matching within hospitals) to make these findings close to representing that of higher level studies as possible, bar doing a prospective randomized controlled trial. Second, the power of the study is dependent on the quality of the data, which relate to the accuracy of data collection and entry. However, NSQIP is likely to be the most accurate database available in the United States due to data collector training, support, and auditing. Third, although we attempted to represent a large population on a national scale, we cannot be certain it is generalizable to the entire population of the United States. The database only includes patients from participating centers, which may not include an important number of patients treated in nonparticipating centers. Finally, the findings in this study only include outcomes at 30 days, an inherent limitation of the database itself. However, many significant outcomes occur during this early period, and thus it is a clinically relevant timeframe.
Conclusion
Comanagement of patients with high-risk hip fracture has been shown to improve outcome and reduce costs, and there is a paucity of data from the United States. Using a national database, we have shown that CM patients had the lowest length of stay. Partially comanaged patients had the highest length of stay and actual morbidity, which may reflect patients developing problems during their stay and heterogeneity in the implementation/components of a comanagement model. No comanagement was associated with less morbidity and mortality, which may signify that the healthiest patients, not requiring any medical input, were managed this way. The fact that this was observed on risk-adjusted data suggests, for reasons already described, that this data set does not permit methods that are sufficiently robust to simultaneously adjust for patient risk profiles and hospital characteristics. In this context, it was a crucial finding that baseline characteristics differed significantly, with CM and PCM patients having the poorest levels of cognition, function, and general health. Overall, our results do support the use of CM of patients with hip fracture between orthopedic surgeons and medicine physicans or geriatricians to maximize outcomes for this high-risk group.
Footnotes
Authors’ Note
Ethical approval was obtained from our university institutional review board.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BLH is consulting director for the ACS NSQIP.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.