
Abstract
Introduction:
We report the clinical and radiographic results of hip arthroplasty using extensive porous-coated stems over 15 years in Korea.
Methods:
This retrospective study included 210 patients (268 hips) who underwent total hip arthroplasties (232 hips) and bipolar hemiarthroplasties (36 hips) between June 1996 and December 2002 for avascular necrosis of the femoral head, hip fracture, or osteoarthritis, after excluding those who died or were lost to follow-up. One senior author (K.H.M.) evaluated Harris Hip Score (HHS); limping gait; and leg length discrepancy, and 3 independent reviewers assessed the radiographic findings, including the level of stress shielding, Dorr classification, subsidence and loosening of femoral stem, heterotopic ossification (Brooker classification), osteolysis of acetabulum, wear rate of the polyethylene liner, component loosening, and revision rate.
Results:
The mean follow-up duration was 16.9 years and average age at operation was 50.9 years. The HHS improved at the last follow-up. Stress shielding was grade 1 in 185 hips, grade 2 in 35 hips, grade 3 in 37 hips, and grade 4 in 11 hips. Femoral stem subsidence was <3 mm in 4 hips and >3 mm in 6 hips. Femoral stems with stable bony ingrowth were observed in 258 hips, fibrous stable femoral stems in 4 hips, and unstable femoral stems in 6 hips. Heterotopic ossification was class 1 in12 and class 2 in 4 hips. Revision surgery was performed for periprosthetic osteolysis of cup (45 hips), recurrent dislocation (1), unstable femoral stem (1), and infection (1). The Kaplan-Meier survivorship at the 15-year follow-up was 86.2%. The survivorship of femoral stem at 15 years was 99.3%, and if including impending revision due to unstable femoral stem was 97.1%.
Disscussion:
This study has all the limitations inherent with a retrospective design. However, a large number of patients in this cohort operated on by a single surgeon and a long-term follow-up are some of the potential advantages of the current study.
Conclusions:
At the 15-year follow-up, extensive porous-coated stem showed relatively good survivorship even in geriatric patients (Dorr type C).
Keywords
Introduction
Hip arthroplasty is a reconstructive surgery that is indicated for patients with severe pain and gait restriction due to various causes of hip arthropathy, by treating the pain and enabling early mobilization. Initially, cement was used to fix the implant to the femur and acetabulum during total hip arthroplasty (THA), but cemented THAs resulted in debonding of the acetabular component and femoral stem, leading to implant failure. 1,2
To solve this problem, methods have been developed to fix the implant to the bone without cement. 3,4 Cementless THAs, that fix the prosthesis to the bone biologically, have been clinically and radiologically evaluated positively over the long term, and the survival rate of these implants has increased due to the reduction of failure by fixation. 5 The Anatomic Medullary Locking (AML, DePuy, Warsaw, Indiana) stem is one of the first-generation cementless implant that is still in use since the 1970s, with good results at the short- and medium-term follow-up, 6 -9 and high survival rate of the implants over the long-term follow-up. 5,10,11
The purpose of this study is to report the clinical and radiographic results of hip arthroplasty using extensive porous-coated stem at a minimum 15 years in Korea.
Material and Methods
Demographics
Between June 1996 and December 2002, the senior author performed consecutive hip arthroplasties in 250 patients using extensive porous-coated stem for patients who were diagnosed mainly with avascular necrosis of the femoral head, hip fractures, and osteoarthritis, among other causes of hip arthropathy. We excluded 25 patients who died before the 15-year follow-up and 15 patients who were lost to follow-up. Among the 210 patients (268 hips; 232 hips of total hip arthroplasties and 36 hips of bipolar hemiarthroplasties) who were finally enrolled in this retrospective study, 148 patients were male and 120 patients were female. The diagnosis of all patients who had bipolar hemiarthroplasty was fracture, there mean age was 65.37 years (52-80). The mean age at the index operation was 50.9 years (range: 15-80 years), and the mean follow-up period for the 210 patients (268 hips) was 16.9 years (range: 15.0-21.5 years; Table 1). We collected the data of the clinical examination, including the Harris Hip Score (HHS excluding fracture cases), limping gait (antalgic, trendelenburg, and short leg), leg length discrepancy (LLD) which were evaluated in outpatient clinic, and radiography, including the level of stress shielding, Dorr classification, subsidence and loosening of femoral stem, heterotopic ossification, osteolysis of acetabulum, wear rate of the polyethylene liner, component loosening, and revision rate. All radiological evaluations had been performed by 3 independent reviewers including the last follow-up X-ray. The survival rate of the implants was determined according to the time of revision surgery. We investigated the revision rate and survivorship. The protocol for this study was approved by institutional review board of author’s affiliated institution.
Demographics, Causes of Hip Arthroplasty.

Abbreviations: AVN, avascular necrosis; M, male; F, female.
Surgical Method and Implants
The same surgical technique and postoperative management protocol was utilized in all patients and was performed by a single surgeon series (K.H.M.). In all patients, a posterolateral approach was used and an AML femoral stem inserted. A ceramic head was used in 218 cases (BIOLOX forte, CeramTec, Plochingen, Germany) and a metal head in 14 cases (DePuy). We used 2 types of bearing surfaces in THA or a bipolar cup in hemiarthroplasty; a polyethylene liner was used in 147 cases (Enduron; DePuy; ultra-high molecular weight polyethylene), a ceramic liner was used in 85 cases (BIOLOX forte, CeramTec), and 36 bipolar cups in hemiarthroplasty. Acetabular components were all uncemented hemispherical cups (Duraloc cup series 1200 [Depuy], PINNACLE 100 Series [Depuy]).
Clinical Evaluation
The functional outcome measures were HHS 12 (excluding fracture cases), limping gait, LLD, and thigh pain. The limping gait was defined as any patient with antalgic, Trendelenburg, or a short leg gait.
Radiologic Evaluation
Radiographic evaluations were performed during each follow-up visit at 6 weeks, 12 weeks, 6 months, 1 year, and yearly thereafter.
The level of stress shielding on simple radiography was classified into 4 levels according to the criteria established by Engh et al. 8 Subsidence of the stem was defined as distal migration of femoral implant measured by the change in the distance between the proximal shoulder of the femoral component and the greater trochanter. The fixation of the femoral component in the follow-up radiographs was classified as bone ingrowth, fibrous stable, or unstable fixation according to Engh et al. 8 Heterotopic ossification was classified by the Brooker classification. 13 Osteolysis of the acetabular cup was defined as newly formed radiolucency around the implants and was graded as small, large, or expansive. In THA cases, the wear rate of the polyethylene liner was measured using the method described by Livermore et al. 14 The Dorr type was checked to see whether there were any differences in failure by type. 15
Statistical Analysis
Preoperative and postoperative HHS, limping gait (antalgic, trendelenburg, and short leg), and postoperative LLD were compared using a 2-sample t test. The types of liner were compared using the log-rank test in the Kaplan-Meier survival analysis. Logistic regression analysis was used to analyze revision results according to age and diagnosis of preoperative fractures. The revision results according to the Dorr type were analyzed using the Cox proportional hazard model. A P value <.05 was considered statistically significant for all differences. All data were analyzed using SPSS software (version 18.0; SPSS Inc, Chicago, Illinois).
Results
Clinical Outcomes
The mean HHS was 67.47 ± 5.41 preoperatively, which had improved to a mean of 83.64 ± 8.44 points at the final follow-up (95% confidence interval [CI], P < .001). Preoperatively, most patients had a limping gait. Postoperatively, the limping gait improved (95% CI, P < .001). Postoperatively, 199 patients had no LLD, whereas LLD persisted in 21 patients (Table 2).
Clinical Outcomes.

Abbreviations: LLD, leg length discrepancy; SD, standard deviation.
Other postoperative complications (Table 3) included dislocation (5 hips), periprosthetic fracture (3 hips), sciatic nerve injuries (2 hips), deep vein thrombosis (1 hip), and wound infection (1 hip; Table 3).
Complications.

We analyzed the correlation of revision rate and age. Revision surgery decreased with age (P = .004). No significant correlation was found between an initial diagnosis of fracture and the need for revision surgery (P = .939).
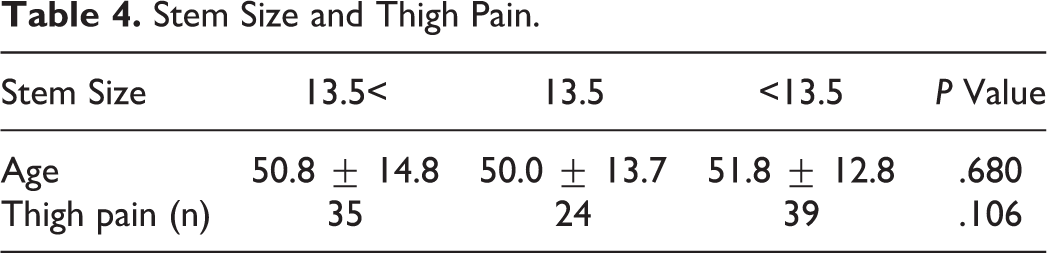
In the revision results according to Dorr type (A: 6 hips, B: 209 hips, and C: 53 hips), Dorr type did not correlate with revision surgery (P = .970, .839). Stem size did not correlate with age (P = .680) or thigh pain (P = .106; Table 4).
Stem Size and Thigh Pain.
Radiologic Outcome
In the radiographic assessment at the final follow-up, stress shielding was observed to be grade 1 in 185 (69.0%) hips, grade 2 in 35 (13.1%) hips, grade 3 in 37 (13.8%) hips, and grade 4 in 11 (4.1%) hips. Subsidence of femoral stems was <3 mm in 4 (1.5%) hips and >3 mm in 6 (2.2%) hips. With respect to the femoral stems, stable bone ingrowth was noted in 258 (96.3%) hips, fibrous stable femoral stems in 4 (1.5%) hips, and unstable femoral stems in 6 (2.2%) hips. Heterotopic ossification was found to be class 1 in 12 (4.5%) hips and class 2 in 4 (1.5%) hips. With respect to the osteolysis of the acetabulum, small lesions were observed in 12 (4.5%) hips, large in 5 (1.9%) cases, and expansive in 31 (11.6%) cases (Figure 1). There were 2 cases of ceramic on ceramic bearings (small and expansive). The polyethylene liner wear rate was 0.11 mm/y ± 0.005 (Table 4).
Survival Rate
The causes of revision (Table 5) were femoral loosening (1 hip), dislocation (1 hip), osteolysis of the acetabulum (45 hips), and infection (1 hip).
Radiologic Outcomes.

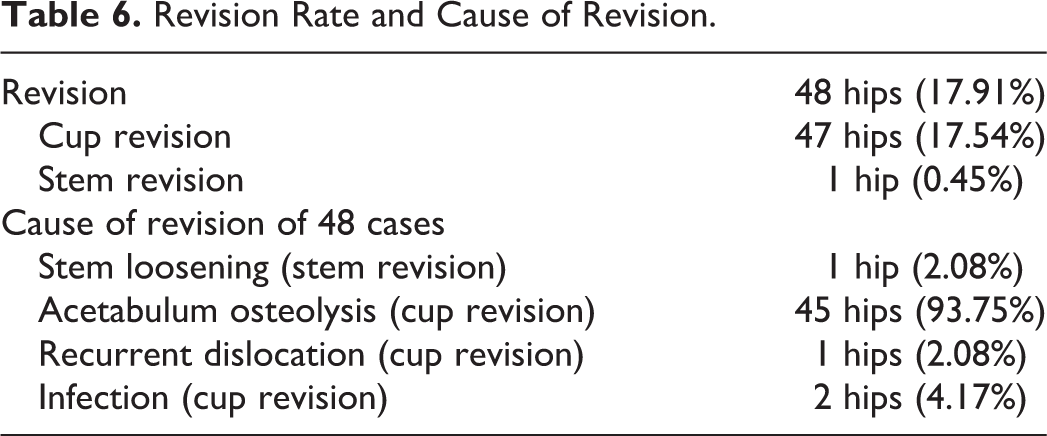
The overall survival rate was 86.2% at the final follow-up with revision for any reason as the end point. On the basis of the articular surface, survival rate of polyethylene liner was 69.4%, ceramic liner was 100%, and bipolar cup was 94.7%. Survivorship of the femoral stem excluding cup revision at the 15-year follow-up for any reason as an end point was 99.3% and including survivorship of unstable femoral stem was 97.1% (Tables 6 and 7).
Revision Rate and Cause of Revision.
Survival Rate at 15 Years.

Discussion
Cementless prostheses, due to their biological stability, have the advantage of survival without disassembly over a long-term period, compared to cement-based prostheses. 9,16,17 Engh and Massin reported a 98.5% survival rate at the 15-year follow-up of patients with first-generation AML. 9 In our study, results similar to previous studies were obtained. Incidence of revision surgery decreased with age. This may be due to lower activity levels in older patients.
Dorr type was not related to revision surgery in our analysis. Engh et al reported that patients with large-diameter, extensively porous-coated femoral components are no more likely to be revised, loose, or have thigh or activity-limiting pain than patients with smaller diameter stems. 18 These results were similar to our research. Stem size was not age related and thigh pain. Therefore, regardless of old age or Dorr type, extensive porous-coated stem is a good option of hip arthroplasty.
Engh et al and Kwon et al also reported that while stress shielding did occur in a cohort of extensively porous-coated stems, it did not result in adverse clinical consequences. 19,20 Our study produced similar results.
Heterotopic ossification is a potential complication following THA, with a reported incidence ranging from 8% to 90%. In our study, 6 cases of class 4 heterotopic ossification were found, which is a lower number than that in other studies. Joice et al reported that the effectiveness of selective nonsteroidal anti-inflammatory drugs (NSAIDs) in preventing heterotopic ossification when compared with a placebo. 21 In our study, NSAIDs were prescribed for more than 2 weeks after surgery, and high-risk group such as osteoarthritis or patients with ankylosing spondylitis were treated 700 cGy (1 fraction) radiation therapy just after surgery suggesting that heterotopic ossification was reduced.
The most common reason for revision surgery was osteolysis of the acetabulum, and therefore, mainly cup revisions were performed. Stem revision was only 1 case. This is due to the characteristics of the AML stem. Since the AML stem is a distal-fitting stem, the polyethylene debris was deposited only on the proximal femur (Gruen zone 1 or 7) and does not affect the stability even if osteolysis occurs. Morcellized bone grafting was performed when proximal femoral osteolysis was found during cup revision surgery.
The concept of “effective joint space,” which includes all prosthesis areas that are accessible to joint fluids and thus to particulate debris, is dispersed in the joint fluid, has been proposed as a mechanism. 22 In other words, polyethylene debris could migrate to distal part of femoral stem. Because AML stem is the extensive porous stem for bone ingrowth in the whole femur, the polyethylene debris does not migrate to the distal end of the stem.
Cup revision was performed frequently when a polyethylene liner had been used. Yan et al reported poor performance of Enduron polyethylene liner in comparison with other polyethylene liner (Trilogy). Therefore, other types of polyethylene liners should be considered when operating patients who need polyethylene liners. 23
Sierra et al reported the dislocation rate of primary THA in elderly patients was 5.3%. We believe the reasons for the low dislocation rates in this study are that the postoperative rehabilitation exercise was performed well during the hospital stay for 2 weeks, and the short external rotator repair was performed at the operation. 24
In Western countries, the incidence of deep vein thrombosis (DVT) following THA, total knee arthroplasty, or hip fracture surgery is 40% to 60%, when no pharmacological prophylaxis is prescribed. 25 However, in Asian countries, including South Korea, the reported DVT rate after hip arthroplasty is reported to be as low as 0.88. 26 The reasons for the low DVT incidences after surgery were genetic characteristic of Asian patients and less fat dietary habit than Western people. In addition, rehabilitation was performed to prevent DVT.
Peitgen et al reported postoperative periprosthetic fracture is a long-term major complication after THA that used proximal-fitted tapered titanium stem (1.6% at 10 years). 27 In our study, the cumulative long-term incidence of periprosthetic fracture was 1.4% at 15 years. We need more comparative analysis and research, and extensive porous-coated stems are stable for prevention of periprothetic fracture.
This study has all the limitations inherent with a retrospective design. However, a large number of patients in this cohort operated on by a single surgeon and a long-term follow-up are some of the potential advantages of the current study.
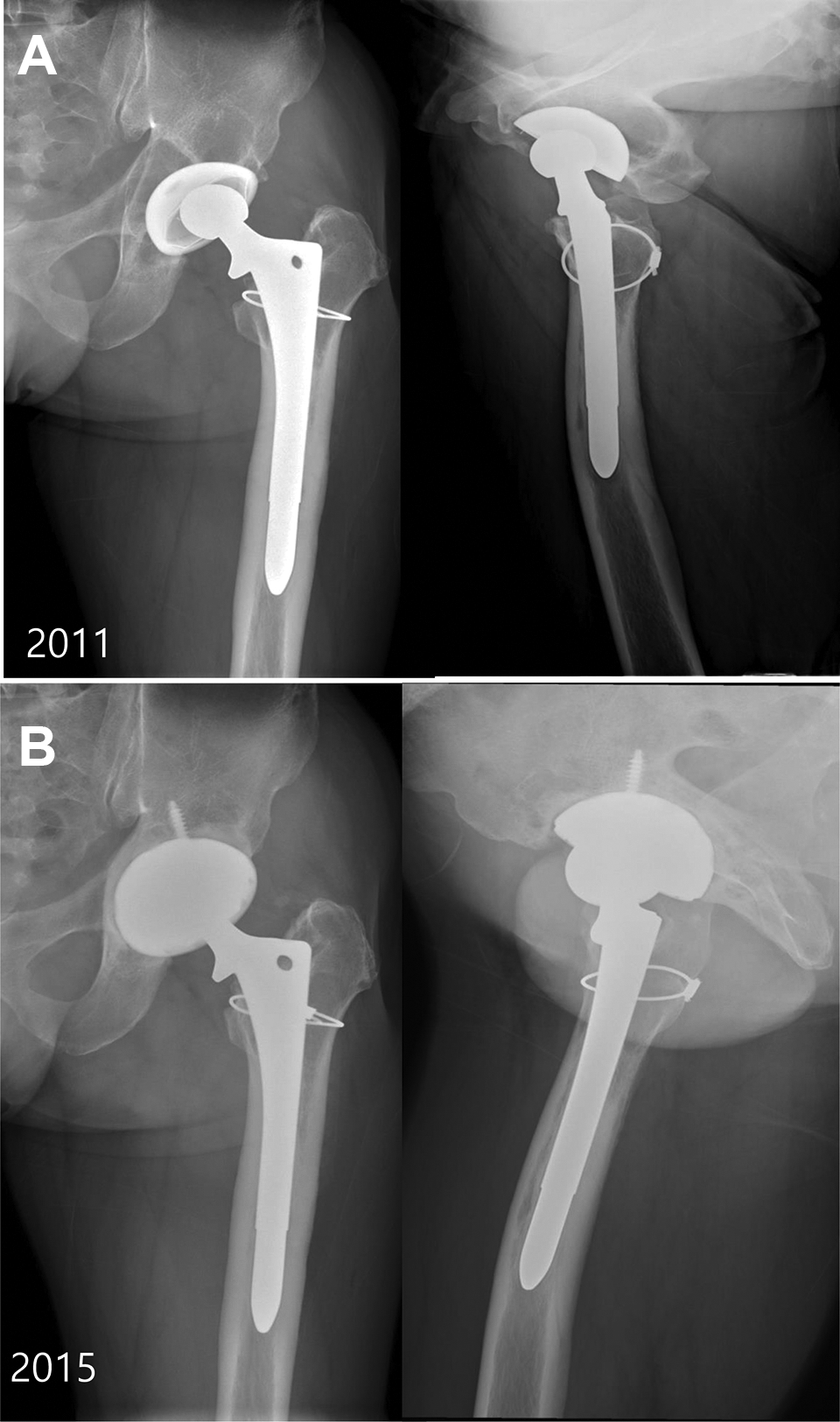
Twenty-nine-year-old male patient diagnosed with avascular necrosis underwent total hip arthroplasty at 2000. A, After 11 years, osteolysis was found on acetabulum. Cup revision sugery was done on 2000. B, Final follow-up X-rays at 2015.
Conclusion
Our results suggest that extensive porous coated stem provide excellent long-term clinical and radiologic outcomes even in geriatric patients(Dorr type C). Furthermore, the bearing surface was very important for component durability and decreasing the revision rate. Ceramic-on-ceramic bearing, extensive porous coated stem provides an outstanding survivorship without other complications requiring revision operation.
Footnotes
Authors’ Note
All authors contributed equally. The protocol for this study was approved by the institutional review board of Inha University Hospital, Incheon, Korea (IRB-2018-03-010).
Acknowledgment
This study was supported by INHA University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.