
Abstract
Introduction:
Recent clinical evidence suggests that total hip arthroplasty (THA) provides improved clinical outcomes as compared to hemiarthroplasty (HA) for displaced femoral neck fractures in elderly individuals. However, THA is still utilized relatively infrequently. Few studies have evaluated the factors affecting utilization and the role socioeconomics plays in THA versus HA.
Methods:
In the United States, the National Inpatient Sample (NIS) database was used to identify patients treated surgically for femoral neck fracture, between 2009 and 2010. Patients were identified using International Classification of Diseases, Ninth Revision, codes for closed, transcervical femoral neck fractures and closed fractures at unspecified parts of the femoral neck. All candidate predictors of THA versus HA were entered into a multilevel mixed-effect regression model.
Results:
Older patient age, being Asian or Pacific Islander, and having Medicaid payer status were all associated with lower odds of receiving THA. Patients with private insurance including Health Maintenance organization (HMO) had higher odds of THA as did patients with other insurance. Odds of THA were significantly lower among patients in teaching hospitals and higher at hospitals with greater THA volume.
Discussion:
Ethnicity, payer status, hospital size, and institutional THA volume were all associated with the utilization of THA versus HA in the treatment of geriatric femoral neck fractures.
Level of Evidence:
Level III Retrospective Cohort study.
Introduction
Geriatric femoral neck fractures represent a major source of patient morbidity and mortality. 1,2 The optimal management strategy remains uncertain; nondisplaced and valgus impacted fractures are typically treated with fixation, while displaced fractures are treated with arthroplasty. Historically, displaced fractures were treated with hemiarthroplasty (HA), but there has been increasing interest in total hip arthroplasty (THA) with numerous contemporary studies demonstrating better clinical outcomes at a lower overall cost. 3 –17 However, studies performed in the United States have demonstrated that despite strong clinical evidence, overall rates of THA as compared to HA have not increased significantly over time. 18,19
Multiple provider-specific factors may help to explain this observation. It is possible that evidence from recently published clinical trials may not yet have impacted practicing surgeons. Surgeons comfortable with performing HA may not be comfortable performing THA, which is technically more demanding and associated with a higher rate of dislocation. A growing body of evidence suggests that socioeconomic factors may influence arthroplasty-related decision-making and quality of care for patients with hip fracture. 20 –23 Factors such as race, sex, and socioeconomic status have been shown to impact both surgeon recommendations for surgery and perceived outcomes after elective joint replacement surgery. 21,22,24,25 However, the importance of these variables in femoral neck fracture decision-making is unknown.
A recent study conducted by Bishop et al found that overall rates of THA increased from 1998 to 2010. In light of these findings, few studies have evaluated the factors affecting utilization rates when compared to HA and the role certain factors such as race, ethnicity, insurance status, and other socioeconomic measures may have on the odds of receipt. 26 The purpose of this study was to evaluate the associations of patients’ race, sex, geography, and other socioeconomic factors on receipt of THA versus HA in the treatment of femoral neck fracture.
Methods
Data from the National Inpatient Sample (NIS) was utilized in this study. National Inpatient Sample is the largest all-payer, inpatient, publicly available health-care database sponsored by the Agency for Healthcare Research and Quality as part of the Healthcare Cost and Utilization Project. Discharge data are deidentified for approximately 8 million hospital stays from more than 1000 hospitals annually. The NIS samples from 46 states account for 97% of the US population and approximate 20% stratified sample of US hospitals.
The cohort for this study included patients with closed, transcervical femoral neck fracture as well as patients with closed fractures at unspecified parts of the femoral neck who underwent THA (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] 81.51) and HA (ICD-9-CM 81.52). Fractures at the base of the femoral neck (ICD-9-CM 820.0, excluding 820.03) were excluded, as fixation rather than arthroplasty is generally recommended for this fracture location. Patients treated with internal fixation were excluded as our goal was to evaluate decision-making for displaced fractures in the elderly individuals, and the vast majority of elderly patients treated with internal fixation likely had nondisplaced or valgus impacted fractures.
The NIS contains information on hospital variables and patient characteristics that were included in our analysis. Patient characteristics including sex, race, and primary expected payer status (Medicare, Medicaid, private including HMO, self-payers, no charge, and other) were included. Reference groups were as follows: gender (male), race (white), payer status (Medicare), median household income for patient’s zip code (USD1-24 999), teaching status (teaching), region (Northeast), hospital location (rural), number of beds (small; see Appendix A for hospital size by number of beds according to NIS). Age was analyzed by patient age in years. To evaluate the effect of patient-level income on THA utilization rates, NIS-provided median household income level of the patient’s zip code was used. Hospital characteristics including urban or rural location, teaching status, region, bed size, and case volume by procedure were also examined as predictors of THA.
In order to determine significant predictors of THA versus HA (yes/no), all candidate predictors were entered into a multilevel mixed-effect logistic regression model which included an adjustment for age.
Hospital ID was included as a random effect in order to account for the clustering of patients within health-care facilities. Odds ratios (ORs) and 95% confidence intervals (CIs) for all parameter estimates were derived from this model. Analyses were conducted using the LME4 package in the R Version 3.0.0.
Results
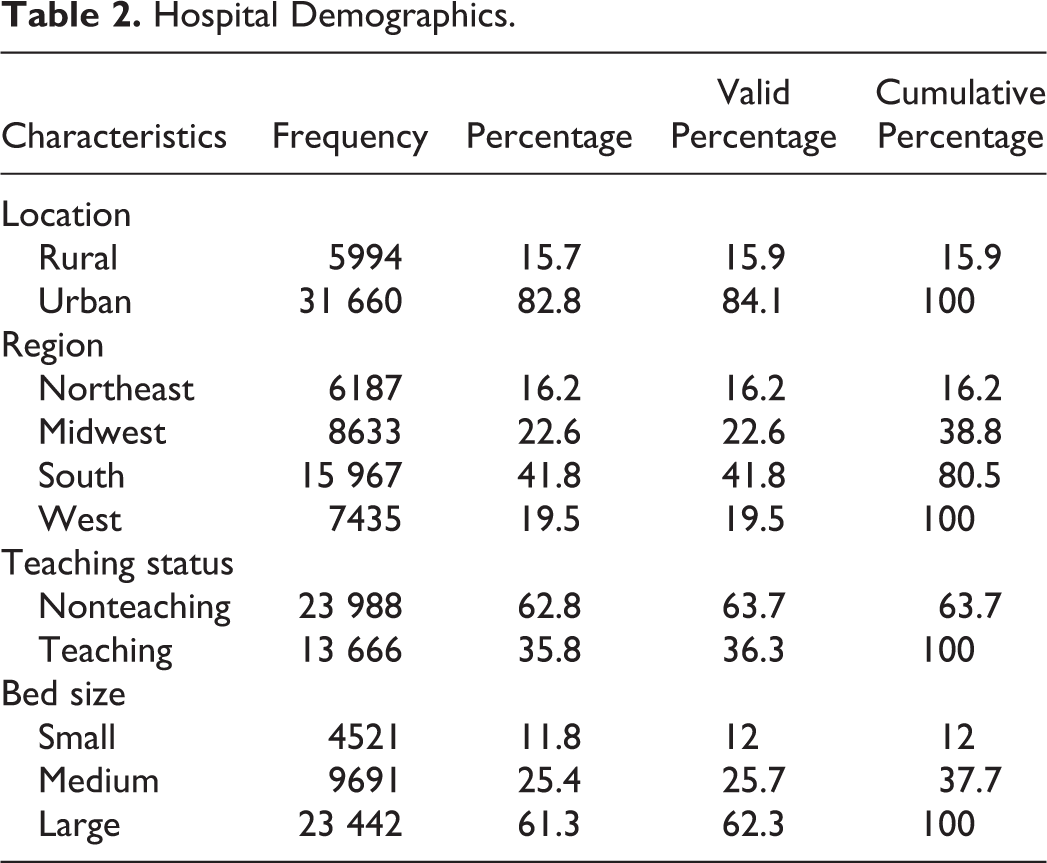
Our cohort included 38 222 femoral neck fracture patients who underwent THA or HA from 2009 to 2010. Of the 38 222 patients included, 29 348 (76.8%) were white, 1365 (3.6%) black, 1294 (3.4%) Hispanic, 499 (1.3%) Asian or Pacific Islander, 185 (0.5%) Native American, 609 (1.6%) other race/ethnicity (Table 1). Among these patients, 3659 underwent THA and 34 563 underwent HA. Hospital region and practice setting (urban vs rural, teaching vs nonteaching) were evaluated. Of the patients included in this study, 31 660 (82.8%) underwent surgery at urban hospitals, while 5994 (15.7%) underwent surgery in rural hospitals (Table 2); 41.8% of patients were from the South region, 19.5% of patients from the West, 22.6% of patients from the Midwest, and 16.2% of patients from the Northeast (Table 2). In all, 23 988 (62.8%) patients underwent surgery in a nonteaching hospital, while 13 666 (35.8%) underwent surgery at a teaching hospital (Table 2).
Patient Demographics.a

Abbreviations: IF, internal fixation; HA, hemiarthroplasty; THA, total hip arthroplasty.
aMedian household income represents income national quartiles for patient’s zip code.
Hospital Demographics.
Older patient age was associated with lower odds of receiving THA (OR: 0.944, P value < .0001, 95% CI: 0.941-0.948; Table 3). Asian or Pacific Islander patients had statistically lower rates of THA compared to Caucasian patients (OR: 0.507, P value = .0019, 95% CI: 0.330-0.778; Table 3). Sex and other race/ethnicities were not significantly associated with odds of receiving THA.
Predictors of THA Versus HA.

Abbreviations: CI, confidence interval; HA, hemiarthroplasty; OR, odds ratio; THA, total hip arthroplasty. Bold represents statistically significant values, p-value <0.05, and or greater or less than 1.
aStandard error represents standard error of fixed effects.
bOther includes CHAMPUS/TRICARE, Children’s Rehab Services, worker’s compensation, Indian Health Services, other, tobacco tax.
cNo charge includes charity.
dPrivate insurance includes Health Maintenance Organization (HMO), Preferred Provider Organization (PPO), Blue Cross, and commercial carriers.
eNote hospital control/ownership was included in the original analysis. No significance was achieved, and a subsequent analysis was run without hospital control variables.
Household income was evaluated using median household income for patient’s zip code as individual patient income was unavailable. Income was stratified into 4 income brackets and compared relative to patients in the $1 to 24 999 income bracket (Table 3). No statistical difference was identified in the rates of THA according to median zip code income.
Discussion
Recent studies indicated that THA is associated with improved clinical outcomes and lower overall cost when compared to HA in the treatment of displaced femoral neck fractures in elderly patients. 3 –5,9 –15 In 2010, over 326 100 total hip replacements were performed in the United States. 27 In this study, data from 38 222 patients with femoral neck fracture treated with either HA or THA were analyzed to identify factors associated with the selection of surgical THA over HA.
This study has inherent limitations. The use of the NIS cannot assess physician or patient rationale or preferences for a particular procedure or treatment over another. Although we were able to account for all patients treated surgically for a closed transcervical femoral neck fracture based on ICD-9 diagnosis and treatment codes, the NIS information cannot account for the degree of fracture displacement, functional status of the patient, or comorbidities, all of which likely influence decision-making. Moreover, the NIS does not have individual-level income and therefore the median household income of patient’s zip code was used, which is an additional limitation of this study. Despite these limitations, this is a large study including data from over 38 000 patients that identifies evidence of disparities in the selection of HA versus THA for femoral neck fracture based on race, payer status, and type of treating hospital.
Older patients in our cohort were less likely to be treated with THA as compared to HA, likely reflecting an emphasis on avoidance of complications rather than maximizing functional outcomes in the oldest and potentially lowest demand patients. This finding is supported with recent literature showing that in patients >70 years of age with an intracapsular fracture had no significant difference in functional outcomes between HA and THA. 28 Moreover, mean ages were similar among Medicare and Medicaid patients (80.59 and 80.74, respectively); however, patients undergoing THA were 6.65 years younger than patients undergoing HA (THA 74.54 and HA 81.19). This finding is consistent with a recent study that the rate of THA for the treatment of femoral neck fractures is increasing for patients younger than 70, but decreasing for patients older than 80. 29 Total hip arthroplasty has been shown to be a cost-effective treatment for displaced femoral neck fractures in patients 45 to 65 years of age. 30 There was significantly less THA in Asian Pacific Islanders. Previous studies indicated significantly lower rates of total hip replacement and total knee replacement surgery among minorities, with researchers hypothesizing that patient preference, perceived and real differences in outcomes, access, insurance status, and other demographics all play a role 21,22,25,31 (Supplementary Table 1).
Medicaid payer status was associated with lower odds of THA utilization (OR: 0.707, P value = .0086, 95% CI: 0.547-0.916) when compared to Medicare patients. Patients with private insurance including HMO had higher odds of THA (OR: 1.456, P value < .0001, 95% CI: 1.297-1.635) as did patients with other insurance (including workers’ compensation, CHAMPUS/TRICARE, Children’s Rehab Services, Indian Health Services, other, tobacco tax; OR: 1.709, P value < .0001, 95% CI: 1.340-2.179). There was no difference between the rates of HA and THA in self-pay patients compared to Medicare patients (Table 3).
The odds of THA were significantly lower among patients in teaching hospitals when compared to nonteaching hospitals (OR: 0.822, P value = .044, 95% CI: 0.679-0.995; Table 3). There was no significant difference in the odds of THA by region (ie, Northeast, Midwest, South, and West) or hospital urbanicity (rural vs urban). When hospital size was evaluated, patients treated at medium-size (OR: 0.702, P value = .003, 95% CI: 0.557-0.884) and large-size hospitals (OR: 0.629, P value = <.0001, 95% CI: 0.503-0.786) had lower odds of THA than patients treated at small-size hospitals. Recent evidence supports that patients treated at hospital with higher THA volume for femoral neck fractures at higher volume arthroplasty centers faired better in regard to lower mortality and 90-day complication rates. 32 In this cohort, patients treated at higher volume THA hospitals also had higher odds of THA for femoral neck fractures (OR: 1.003, P value <.0001, 95% CI: 1.002-1.003) than patients treated at hospital with lower THA volume.
Medicaid patients (including both fee-for-service and managed Medicaid patients) had significantly lower rates of THA, while patients with private insurance including HMO and “other” had significantly higher rates of THA, suggesting that payer status impacts treatment strategy and highlighting another important disparity. Payer status has already been shown to have an important impact on access to care of the orthopedic patient 33 as well as outcomes, rates of postoperative in-hospital complications, and consumption of resources following total joint arthroplasty. 34 When evaluating hospital-level factors, teaching status was associated with significantly lower rates of THA. This difference may partly be accounted for by differences in patient populations between teaching hospitals and nonteaching hospitals, surgical training, or surgeon preference. Bed size was inversely associated with THA rates, suggesting that the smaller hospitals are more likely to perform THA in these patients relative to HA. Finally, higher hospital THA volume was associated with increased THA rates for femoral neck fracture, which is intuitive.
In conclusion, this study revealed disparities in the utilization of HA versus THA in the elderly patient population with femoral neck fracture. Certain minority groups and patients with less favorable payers/insurance are less likely to be treated with THA despite mounting evidence that this is the optimal treatment in many cases. 3 –17 Similarly, patients presenting to teaching hospitals, larger hospitals, and hospitals with a low volume of THA are less likely to be treated with THA. Further research is indicated to identify the underlying causes of these disparities, while educational and health policy interventions should be introduced to ensure that all patients have access to high-quality and evidence-based surgical treatment regardless of their demographics.
Footnotes
Appendix A
Bed Size Categories.

| Hospital Bed Size | |||
|---|---|---|---|
| Small | Medium | Large | |
| Northeast region | |||
| Rural | 1-49. | 50-99 | 100+ |
| Urban, nonteaching | 1-124 | 125-199 | 200+ |
| Urban, teaching | 1-249 | 250-424 | 425+ |
| Midwest region | |||
| Rural | 1-29. | 30-49 | 50+ |
| Urban, nonteaching | 1-74. | 75-174 | 175+ |
| Urban, teaching | 1-249 | 250-374 | 375+ |
| Southern region | |||
| Rural | 1-39. | 40-74 | 75+ |
| Urban, nonteaching | 1-99. | 100-199 | 200+ |
| Urban, teaching | 1-249 | 250-449 | 450+ |
| Western region | |||
| Rural | 1-24. | 25-44 | 45+ |
| Urban, nonteaching | 1-99. | 100-174 | 175+ |
| Urban, teaching | 1-199 | 200-324 | 325+ |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.