
Abstract
Introduction:
Displaced femoral neck fractures in the elderly individuals may be treated with total hip arthroplasty (THA) or hip hemiarthroplasty (HHA). However, it is unclear what the short-term medical outcomes are related to these surgical options. The purpose of this study was to compare early postoperative outcomes in THA patients to those of HHA patients.
Methods:
In this study, we compared 30-day mortality, likelihood of still being in the hospital at 30 days, postoperative major and minor complications, discharge disposition, reoperation and readmission, length of stay, days from admission to surgery, and operative time between THA and HHA. Using the American College of Surgeons National Surgical Quality Improvement Project database, hip fracture patients ≥65 years old from 2008 to 2016 were identified. After propensity score matching, there were 2795 THAs and 2795 HHAs. To assess the effect of THA on the above-mentioned outcomes, bivariate regression models were created.
Results:
The THA patients ≥65 years old were at reduced risk for mortality (P = .029) and still being in the hospital at 30 days (P = .017). The THA patients were at an increased risk for minor complications (P = .011) and longer operative times (P < .001). However, THA patients were more likely to have a home discharge (P < .001).
Discussion:
Patients ≥65 years who underwent THA for hip fractures had reduced short-term mortality risk, were more likely to be discharged home, and had less likelihood of being in the hospital at 30 days. This is the first study to explore short-term outcomes in patients ≥65 and has direct implications for alternate payment and merit-based payment models.
Conclusion:
As hip fracture treatment has come under scrutiny with respect to alternate payment models and merit-based incentive payments, this analysis of short-term outcomes warrants consideration when evaluating treatment pathways.
Introduction
Hip fractures occur relatively frequently, with a lifetime incidence of 20% in females and 10% in males. 1 This injury can have devastating consequences, as 1-year mortality rates associated range between 14% and 25%. 2 -5 Not only are hip fractures associated with dramatically increased mortality, but they also bear substantial health-care costs, with the estimated cost of hip fracture admissions in the United States in 2015 ranging between US$10.3 and US$15.2 billion. 6
Displaced femoral neck hip fractures are currently treated with either total hip arthroplasty (THA) or hip hemiarthroplasty (HHA); however, treatment selection is controversial. 7 -12 Guidelines in the United Kingdom recommend THA for patients who can ambulate outside the home, have no cognitive impairment, and are medically fit for the procedure. 13 Formal guidelines in other countries, such as the United States, are yet to be formulated. Several articles have reported a mortality benefit of up to 10 years for those treated with THA when compared with HHA, while other studies have found no mortality benefit. 14 -17 When performed for the treatment of hip fractures, HHAs have shown inferior functional scores but have lower rates of dislocation compared to THA. 18 -20 Additionally, it remains unclear whether either surgical modality is associated with inferior postoperative complication rates. 20 -24 A recent study from Canada also found that the health-care costs in the first year after injury was Can$2700 lower for THAs than HHAs. 20
Although previous studies have examined long-term morbidity and mortality, as well as rates of surgical complications, there is a lack of research on short-term morbidity, mortality, and medical complications. As hip fracture treatment has come under scrutiny with respect to alternate payment models and merit-based incentive payments, an analysis of short-term outcomes is warranted. Therefore, the aim of the current study is to assess the effect of THA compared to bipolar HHA for the management of hip fractures in patients ≥65 years old. Specifically, the following outcomes were assessed: (1) 30-day mortality, (2) still hospitalized at 30 days, (3) 30-day postoperative major and minor complications, (4) discharge disposition, (5) reoperation and readmission, (6) length of hospital stay (LOS), (7) days from admission to surgery, and (8) operative time.
Methods
Data Source
The American College of Surgeons (ACS) National Surgical Improvement Quality Improvement Program (NSQIP) database was utilized. The database contains numerous comorbidity and perioperative care variables as well as postoperative mortality and morbidity outcomes for surgeries in a variety of specialties. 25,26 The 2016 version draws data from 680 hospitals across the United States. The ACS NSQIP database has been used to evaluate short-term outcomes in hip fracture patients. 27 -29
Study Population
Using any iteration of the International Classification of Diseases, Ninth Revision (ICD-9) codes 820 and 821 and ICD-10 code S72, we identified 89 075 hip fracture cases. Patients were then excluded if they did not have a procedure corresponding to Current Procedural Terminology codes 27130 (THA) and 27125 (bipolar HHA). This resulted in 16 582 (18.6%) patients. Patients were then selected if there were ≥65 years old (n = 11 831) for subgroup analysis. There were 9033 HHA and 2798 THAs in the ≥65 subgroup.
Study Variables
The following preoperative variables on patient demographics and comorbidities were also collected: age, sex, race, body mass index (BMI), functional status, American Society of Anesthesiologists (ASA) classification, year in which surgery was performed, anesthesia type, and comorbidity count (Table 1). Functional status was used a surrogate for ambulatory status, specifically the variable options at entry are “independent,” “partially dependent,” “totally dependent,” and “unknown.” 30 The comorbidity count assigned 1 point for the presence of available comorbidity variables: diabetes mellitus, dyspnea, use of a ventilator, history of chronic obstructive pulmonary disease, ascites, history of congestive heart failure, use of hypertension medication, renal failure, use of dialysis, disseminated cancer, wound infection, corticosteroid usage, weight loss, bleeding disorder, prior transfusion, and previous sepsis. The comorbidity count was isolated to all comorbidity variables without missing values in the database.
Demographics in THA and HHA.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; HHA, hip hemiarthroplasty; SD, standard deviation; THA, total hip arthroplasty.
a Student t test.
b Fishers exact test.
Bold values are < 0.05.
Perioperative and Postoperative Outcomes
The perioperative and postoperative outcomes of interest were as follows: 30-day mortality, still in the hospital at 30 days, 30-day complications, nonhome discharge, operative time, and LOS. Thirty-day complications were grouped into major complications and minor complications using the proposed classification of Pulido et al, which identifies complications as major “if they required complex surgical or medical intervention if they were deemed to pose a threat to patient’s life or result in functional impairment.” 31 As defined by the ACS NSQIP, the following complications were classified as major: deep incisional surgical site infection (SSI), organ/space SSI, dehiscence, unplanned intubation, pulmonary embolism, on a ventilator greater than 48 hours, acute renal failure, stroke or cerebrovascular accident, cardiac arrest requiring cardiopulmonary resuscitation, myocardial infarction, deep vein thrombosis (DVT) requiring therapy, sepsis, and septic shock. 25 The following were considered minor complications: superficial incisional SSI, pneumonia, progressive renal insufficiency, urinary tract infection (UTI), and transfusions within 72 hours of surgery.
Propensity Score Matching
Logistic regression was utilized to generate propensity scores for patients in the THA and HHA cohorts. Patients were matched at a ratio of 1:1 using the following covariates: age, sex, race, ASA classification, functional status, anesthesia type, year in which the surgery was performed, and a comorbidity count as previously defined using the “MatchIt” package provided with R software. 32 Due to a large number of missing values, BMI (n = 374, 6.7%) was excluded from the propensity score matching. After propensity score matching, there were 5590 cases, including 2795 THAs and 2795 HHAs.
Data Analysis
Patient demographic characteristics in addition to postoperative outcomes were assessed using χ2 tests for categorical variables and independent sample t tests for continuous variables (Table 2). Bimodal bivariate logistic regression models were used to identify THA as an independent risk factor for the outcomes of interest. To assess for increased LOS, days from admission to surgery, and operative time, bivariate linear regression model were constructed to evaluate THA as an independent risk factor. An α value of <.05 was used as statistical significance for all tests. SPSS Statistics 23 for Mac (IBM Corporation, Armonk, New York) was used to perform all tests.
Outcomes and Complications in THA and HHA.
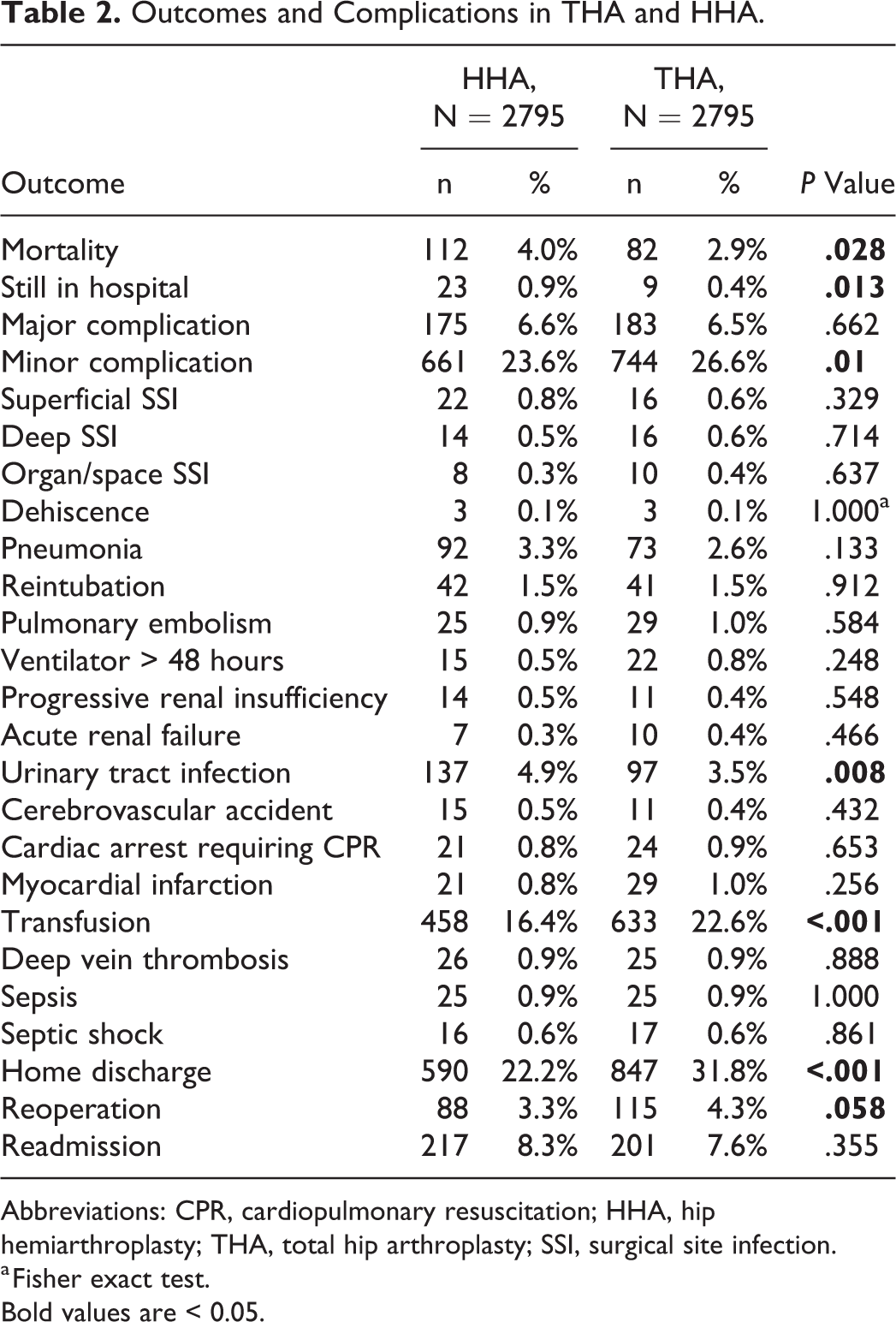
Abbreviations: CPR, cardiopulmonary resuscitation; HHA, hip hemiarthroplasty; THA, total hip arthroplasty; SSI, surgical site infection.
a Fisher exact test.
Bold values are < 0.05.
Results
Thirty-Day Mortality
Using multivariate regression analyses, THA (odds ratio [OR], 0.724; 95% confidence interval [CI], 0.524-0.967; P = .029) was associated with a decreased risk of mortality when compared with HHA.
Still in the Hospital at 30 Days
There was decreased risk for still being in the hospital when treated with a THA (OR, 0.389; 95% CI, 0.180-0.842; P = .017).
Thirty-Day Postoperative Major and Minor Complications
There was no association between major complications (OR, 1.049; 95% CI, 0.847-1.299; P = .662). The THA patients were at an increased risk of minor complications (OR, 1.171; 95% CI, 1.038-1.322; P = .011). The only complication that was associated with a decreased risk of occurring in THA patients was UTI (OR, 0.698; 95% CI, 0.535-0.910; P = .008). There was an increased risk of transfusion (OR, 1.494; 95% CI, 1.307-1.708; P < .001) when being treated with THA. Table 3 contains a full list of ORs for each complication.
Multivariate Regression Analysis of Perioperative Outcomes and Complications.
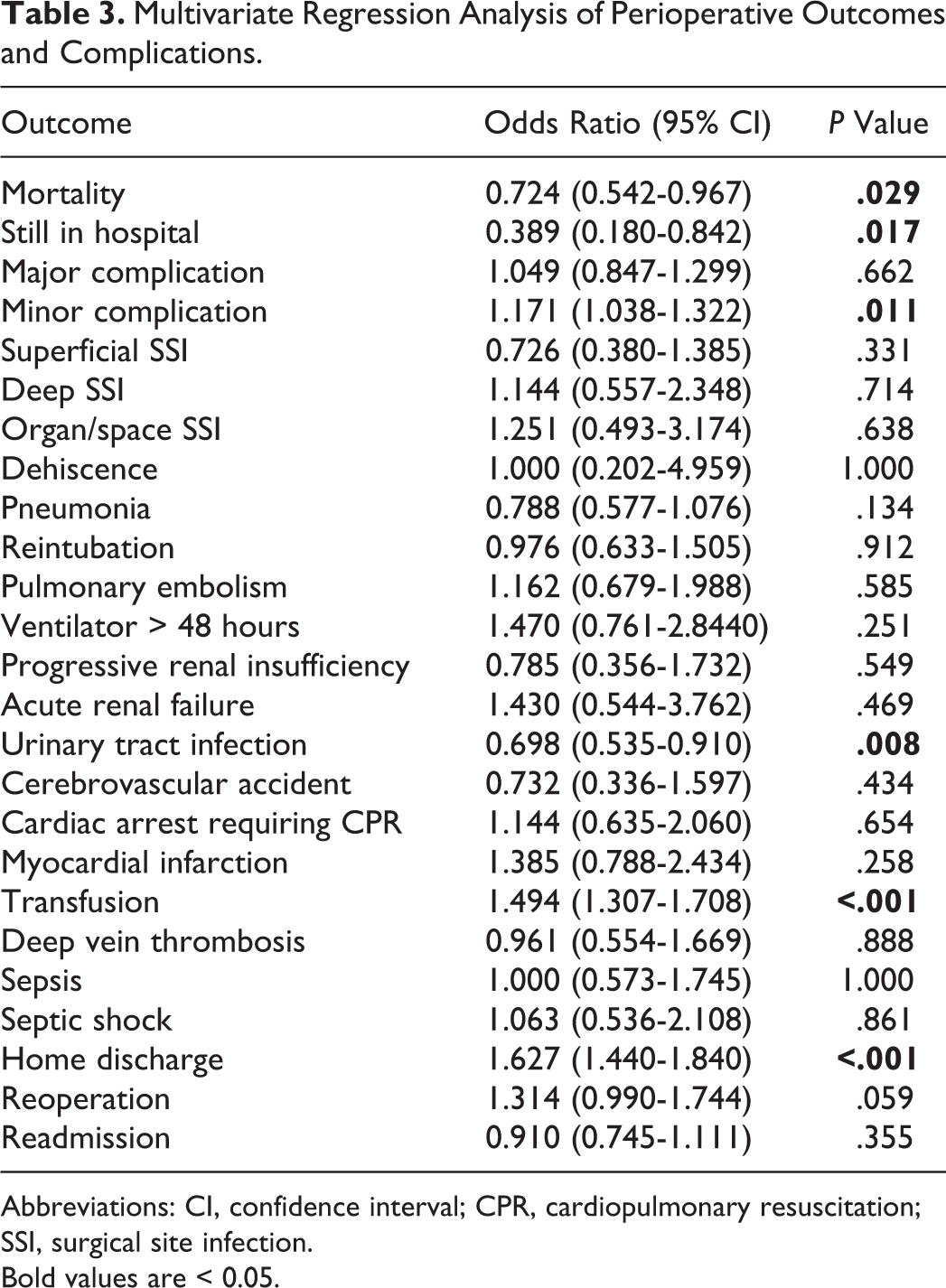
Abbreviations: CI, confidence interval; CPR, cardiopulmonary resuscitation; SSI, surgical site infection.
Bold values are < 0.05.
Discharge Disposition
Total hip arthroplasty was associated with an increased likelihood of home discharge (OR, 1.627; 95% CI, 1.440-1.840; P < .001).
Reoperation and Readmission
There was no statistically significant relationship for treatment choice between THA and HHA for reoperation (OR, 1.314; 95% CI, 0.990-1.744; P = .059) and readmission (OR, 0.910; 95% CI, 0.745-1.111; P = .355).
Length of Stay, Days From Admission to Surgery, and Operative Time
Using linear multivariate regression models, THA was not associated with a decreased LOS (B = −0.381 days; 95% CI, −0.766 to 0.005; P = .053). There was no difference in days from admission to surgery (B = 0.232 days; 95% CI, −0.212 to 0.676; P = .306). Total hip arthroplasty was associated with increased operative time (B = 17.372 minutes; 95% CI, 15.002-19.743; P < .001).
Discussion
Hip fractures place a large burden on our health-care system. 3,4,6 There is substantial controversy regarding the indications for THA and HHA as well as what should be the preferred treatment in different circumstances, 3,7,12,13 including in different age subgroups. Our study found that patients aged 65 years and older who were treated with a THA had decreased mortality when compared with propensity score–matched patients after HHA. These patients were also at a decreased risk of being in the hospital past 30 days postoperatively and were more likely to be discharged home. They were, however, at an increased risk of minor complications and transfusions.
Although this study benefits from propensity score matching, is it not without limitations. Data on patient and surgeon preference for THA versus HHA were not available; however, in an effort to mimic ambulatory status, patients were matched based on their functional status. Moreover, the vast majority of patients were independent prior to their injury indicating these patients may have been appropriate candidates for THA. Additionally, patients were unable to be matched based on Charlson or Elixhauser comorbidity indices; however, in an attempt to as closely replicate these assessments of global health and medical fragility metrics, patients were matched by a comorbidity count as well as ASA classification. Despite this, it is likely that more medically fragile patients received an HHA. Although there were statistically significant differences in BMI, age, and comorbidity count, these differences were clinically irrelevant. Similarly, there were statistically significant differences in ASA classification and anesthesia modality; however, these were as a result of the robust cohort sizes, making even small differences statistically significant. Previous place of residence was not controlled for which may bias the results of the discharge disposition outcome. Preoperative nutrition status was not controlled for using albumin values as 38.8% of the prematched cohort did not have this laboratory value available. It should also be pointed out that there may be an outsized effect of transfusions on the minor complications variables, as there was substantially more transfusion than any other complication. The ACS NSQIP database only contains 30-day complication rates, which will capture many complications directly attributable to the surgical episode. Long-term follow-up data to capture outcomes outside the 30-day window could shed more light on the role of THA versus HHA with respect to complications, including those experienced in the first several years after surgery. Despite these limitations, this study is the first of its kind to describe the role of THA and HHA with respect to short-term medical complications and key health-care-associated metrics.
The findings of this study are supported in prior literature. In a retrospective analysis of 2902 femoral neck fractures treated with THA matched with 2902 fractures treated with HHA, those receiving THA had a decreased risk of mortality at 5 years (risk ratio [RR], 0.51; 95% CI, 0.46-0.570). 14 Similarly, a study of 70 242 femoral neck fractures found that the 2-year survival of patients receiving THA was superior to those receiving HHA (adjusted hazard ratio, 1.67; 95% CI, 1.59-1.92). 15 In one randomized trial, after 100 months of follow-up with 81 displaced femoral neck fracture patients, more HHA patients perished than those in the THA treatment arm (P = .026). 33
Several findings on the topic of complications surrounding the treatment decision of THA versus HHA support our findings. A meta-analysis of 12 randomized control trials, with 624 THA patients and 696 HHA patients treated for displaced femoral neck fractures, found no difference in general complication rate (RR, 1.15; 95% CI, 0.91-1.45) at a minimum of 24 months, 21 similar to our findings on major complications. In Liodakis et al, a study of 3192 HHA versus 866 THAs found that THA was not an independent risk factor for major complications (OR, 0.8; P = .18) but was a risk factor for transfusion (OR, 01.68; P < .001). 22 Similarly, in Burgers et al, a meta-analysis of 472 THA patients and 514 HHA patients with minimum 1-year follow-up found equal rates of major complications (25% in THA vs 24% in HHA). 23 A retrospective review of 2437 THAs and 38 328 HHA treating intracapsular hip fractures patients found no difference in short-term complications at 90 days (OR, 0.89; P = .06). 24 Ravi et al, 20 a retrospective review of 2689 THAs matched to 2689 HHAs, found no differences in myocardial infarction, DVT, pulmonary embolism, nor pneumonia at 90 days.
Our finding that THA patients are more likely to be discharged to home after a femoral neck fracture when compared with HHA patients is supported by prior investigations. A case–control study by Jonas et al of 110 intracapsular hip fractures patients, matched 1:1 THA to HHA, found less HHA patients (33/55) were discharged home when compared with THA patients (35/55). 34 In a survey of US trends in the treatment of femoral neck fractures by Woon et al, THA patients were more likely to be discharged home than their HHA counterparts (23.2% vs 11.6%; P < .01). 35
In Wang et al, a meta-analysis of 8 randomized trials found no difference LOS. Ravi et al also concluded that there was no difference in LOS between THA and HHA patients in addition to findings that THAs had 10 minutes more of operative time. In van den Bekerom et al, a randomized trial with 137 HHAs and 115 THAs found that operative time was longer in THA cases (28% >1.5 hours vs 12% >1.5 hours; P < .001). 36 A comparable randomized trial of 21 THAs and HHAs treating displaced femoral neck fractures found that THA had increased operative time as well (51.80 ± 8.70 minutes HHA vs 119.10 ± 16.75 minutes THR group; P < .0001). 12
An investigation of the treatment decision between HHA and THA in hip fractures found that there may be no difference in revision rates in the elderly individuals. Specifically, a study of 40 THAs versus 72 HHAs in unstable intertrochanteric fractures found no difference in revision rates at a minimum of 2 years follow-up, which may support reoperation. 11
Our article has found several differences in outcomes from what can be found in the literature. In Voskuijl et al, a retrospective study treating femoral neck fractures with 74 088 HHA patients and 8503 THA patients found no difference in in-hospital mortality; however, this was a cross-sectional study of patients treated during 1 year, and no matching occurred despite the large difference in cohort size. 16 A meta-analysis of 7 randomized trials with 828 patients found that reoperation at 1 year was less likely to occur in THA cases (RR, 0.40; 95% CI, 0.24-0.67; P = .0004). 18 However, the minimum follow-up was 1 year, and there was a smaller sample size. Additionally, a retrospective study of 22 675 hip fractures treated with HHA and 8155 treated with THA found increased 1-year revision rates for THA patients (cumulative incidence function 2.4% [95% CI, 2.0-2.7] vs 1.6% [95% CI, 1.4-1.8]) 37 ; however, no match was attempted and the outcome was evaluated at 1 year.
Conclusion
In summary, THA patients ≥65 years old are at a decreased risk of 30-day mortality when compared with HHA patients. Additionally, THA patients were more likely to go home and less likely to be in the hospital after 30 days when compared with HHA patients. However, they were more likely to have minor complications. As hip fracture treatment has come under scrutiny with respect to alternate payment models and merit-based incentive payments, this analysis of short-term outcomes warrants consideration when evaluating treatment pathways.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.