
Abstract
Introduction
It is predicted that by the middle of the century, approximately 6 million people worldwide will sustain hip fractures (HF) annually. 1 As the global population ages, the significance of this condition will continue to grow. HF patients are known to experience up to 14% early mortality and up to 40% post-operative complications.1-6 These poor outcomes are attributed to factors such as age, high morbidity (including hypertension, diabetes, obesity, heart failure, osteoporosis, etc.), smoking, alcohol abuse, malnutrition. Due to these reasons, HP is often regarded as “the last fracture of whole life”.1,7-9 Despite some studies showing a decreasing incidence in Northern countries and stabilisation in Central Europe, the rate of complications and treatment costs are expected to rise. 10
Given the fragility of these patients, accurate preoperative assessment of mortality and morbidity risk following HF is essential to modern treatment.5,11 This assessment not only aids in determining the timing of surgery and providing appropriate information to the patient and their family but also identifies patients at the highest risk who require perioperative interventions.1-14 Understanding the risk of surgery is crucial for both the patient and the surgeon.
To address these concerns, risk calculators has been introduced. The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) surgical risk calculator is a unique tool designed to predict 18 different procedure-specific outcomes based on The Current Procedural Terminology (CPT) codes.3,5,14-18 However, its performance in HF patients is understudied. Additionally, C reactive protein/albumin ration (CAR) has previously been found to predict 30 day and 1 year mortality and morbidity in various pathologies, but its effectiveness compared to risk calculators in HF patients is unknow.19-22
In 2007, Nottingham hip fracture score (NHFS) was introduced and has shown reliability in predicting 30 day and 1 year mortality in HF. The NHFS was used as a control measure in the present study.23-25
The objective of this study was to assess and validate the ACS NSQIP, NHFS surgical risk calculators and CAR index in predicting complications and 30 day mortality among HF patients. 26
Methods
General information on patients.
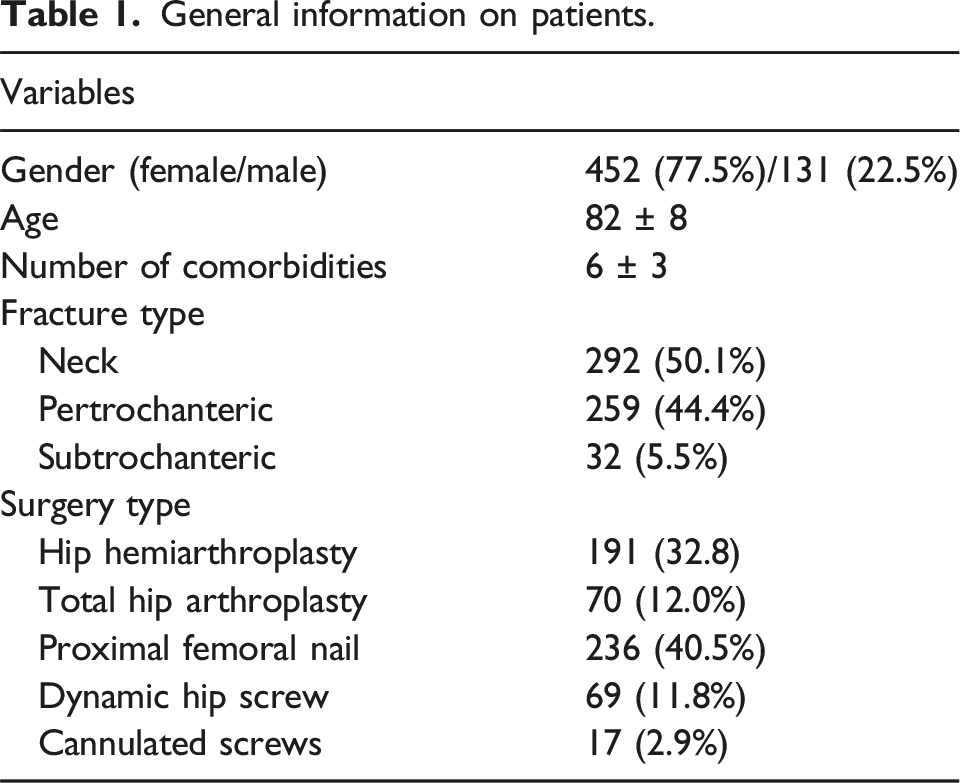

Final Sample Size of Included Patients
All analyses were conducted using IBM SPSS version 26.0 software (SPSS Inc, Chicago, IL) for Windows. Normally distributed data are presented as mean (±standard deviation). Non normally distributed data are presented as median (25-75th IQR). Shapiro-Wilk test was used to assess the normality of data distribution. Discrimination in this study was evaluated using the area under the receiver operating characteristic (ROC) curve, also known as the AUC or c-statistic. The AUC ranges from 1.0 (perfectly discriminating model) to 0.5 (no better than chance). An AUC of 0.6-0.69 indicates poor discrimination, 0.7-0.79 indicates adequate discrimination, 0.8-0.89 indicates strong discrimination, and 0.9-1.0 indicates excellent discrimination.
Results
Frequencies of complications.

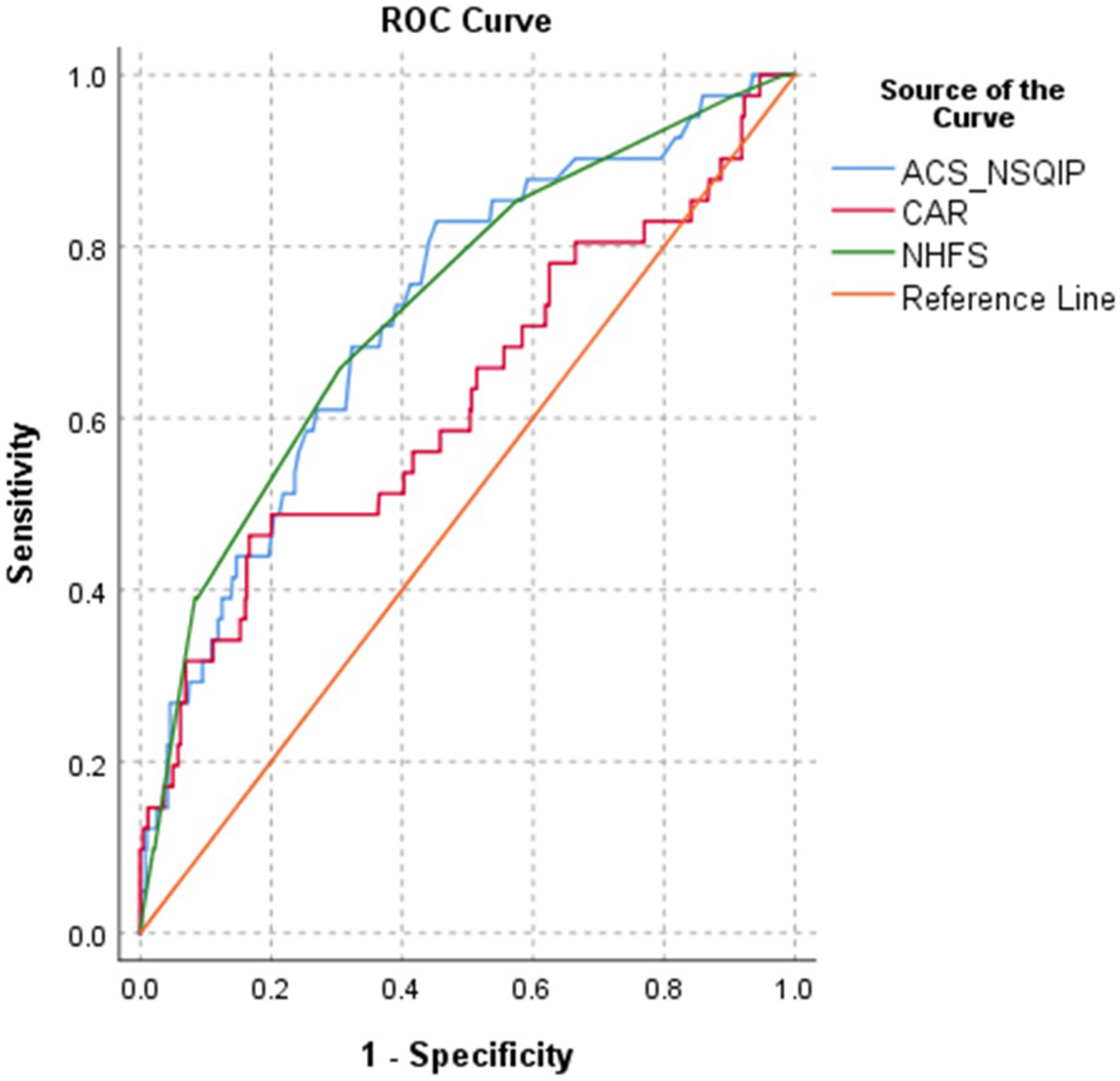
Receiver Operating Characteristics (ROC) of the The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) Surgical Risk Calculator, Nottingham Hip Fracture Score (NHFS) and C Reactive Protein/Albumin Ration (CAR) for Prediction of 30 day Mortality
AUC and p values of risk calculators performances in prediction of death and any complication.


Receiver Operating Characteristics (ROC) of the The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) Surgical Risk Calculator, Nottingham Hip Fracture Score (NHFS) and C Reactive Protein/Albumin Ration (CAR) for Prediction Of Any Complication
AUC and p values of ACS NSQIP risk calculator performance in predicting complications.

Discussion
Surgical risk calculators are highly valuable tools that enhance the understanding of patients and their families, as well as assist in making surgical decisions based on numerical data. In our cohort, none of the models demonstrated excellent discrimination results (AUC >.80) in predicting 30 day mortality and morbidity among HP patients. Since the AUC is greater than 0.7, both the ACS NSQIP and NHFS are effective predictors of 30 day mortality. Only after adjusting for fracture type, did the NHFS show excellent discrimination for 30 day mortality in patients with femoral neck fractures. It should also be noted that the NHFS predicted a lower mortality rate than what was observed in the current study.
To our knowledge, this is the first study to compare CAR to risk calculators in the same cohort. CAR was ineffective in predicting early mortality and even worse in predicting morbidity in our study. This result contrasts with findings in the literature: Cacciola et al found CAR .816 as a reliable predictor, and Balta et al reported an AUC of .727 for intertrochanteric fractures.22,27 It is important to note that both previous studies were retrospective, and at the time of writing, we did not identify any prospective study ROC analysis of CAR in HF patients. Additionally, the timing of CRP sample collection might be crucial—we only included acute fractures, and in this scenario, CRP may not be elevated. However, this hypothesis needs further investigation. Although CAR has been identified as a valuable predictor in various pathologies, our results indicate that its capabilities are understudied in HF patients.
ACS NSQIP is a recent tool that utilizes procedure-specific prediction based on CPT code. The calculator has been shown to be a reliable predictor in various fields of elective and emergency settings. ROC analysis indicates it is adequate predictor of 30 day mortality; however, its ability to predict specific complications is limited, which is a notable drawback in our settings. Additionally, ACS NSQIP was developed using patient data exclusively from United States NSQIP hospitals, which may contribute to its poor discrimination in other countries. 3 Nonetheless, this tool is continuously updated and should be evaluated over time as its design shows significant potential.
The ACS NSQIP calculator was developed from the National Surgical Quality Improvement Program (NSQIP) data to enhance surgical care quality in the USA. Harris et al 11 later created the Hip Fracture Surgery Risk Calculator using the same data, available at https://s-spire-clintools.shinyapps.io/hip_deploy/. The model predicts 30-day mortality with an AUC of .76. Depending on the mortality risk threshold, its sensitivity and specificity vary: a 15% threshold shows 97% specificity and 78% sensitivity. These results suggest that while the model is predictive, it may overestimate mortality for some patients who could benefit from surgery. Surgeons should consider this when making treatment decisions with patients. We did not analyse this model as it was unavailable during development of our study. The author also suggested analysing the performance of risk calculators on patients who were not operated, which has not been done to our knowledge in literature and is 1 of the limitations of our study.
Originally, NHFS was developed to assess the risk for all types of proximal femur fractures. However, intracapsular fractures have been found to have higher mortality and morbidity than compared to extracapsular ones.23-25 This suggests that NHFS could be used for mortality risk stratification for femoral neck fractures in our settings. Moreover, NHFS is a reliable predictor and easy to use, as it only requires preoperative data. To continue, as NHFS inputs objective values, it should be less vulnerable to cultural and social differences among different populations. However, external validation in each country should be conducted before its use.
The observed complication rate in our cohort was 49.2%, which aligns with the 12.5–75% range reported in the literature. 2 The variation in complication rates found in the literature is largely due to differences in study methodologies—retrospective studies typically report lower complication rates compared to prospective studies.2,28 Additionally, follow-up times vary across the literature and should be considered. Furthermore, complications are documented differently across studies. In our study, we registered serious complications according to the ACS NSQIP questionnaire, and for any complication, we recorded every event requiring additional intervention or consultation that deviated from the normal treatment pathway. This methodology for documenting all complications may have increased our reported complication rate. Generally, HF patients should be expected to experience complications, and they and their relatives must be properly informed about this possibility. Considering that NHFS uses fewer preoperative values, it is easier to use compared to ACS NSQIP. In our cohort, NHFS demonstrated strong discrimination in predicting 30 day mortality in intracapsular fractures. Based on these findings, NHFS is recommended for risk stratification in femoral neck fractures within our settings. Additionally, the results indicate that intracapsular and extracapsular proximal femur fractures, which require different surgical approaches, might benefit from fracture-specific risk calculators.
As with all studies, this study has limitations. Firstly, it is a single-centre study of 1 hospital cohort, we cannot confirm that the same results would apply to the entire population. Secondly, we only included risk calculators specific to hip fractures and excluded tools popular in other surgical fields (eg, P-POSSUM, E-PASS, Clarkson comorbidity index). These calculators were excluded purely for methodological reasons—expanding study requires additional human resources and working time. Additionally, recent tools such as the Hip Fracture Surgery Risk Calculator were not available at the time of the study but should be considered for comparison in future research. 2 Lastly, the tools should be evaluated for their sensitivity and specificity.
Footnotes
Ethical Approval
The study was approved by the Institutional Review Board of Republic Vilnius University Hospital and Vilnius Regional Biomedical Research Ethics committee.
Patient Consent
All patients or their proxy gave their informed consent to participate in the study.
Author Contributions
PM conceptualized the present study, collected, analyzed and interpreted the data, performed statistical analysis, interpreted the results and drafted manuscript; RB, SU, RM, VU and IŠ collected, analyzed and interpreted the data, interpreted the results. The manuscript was reviewed by all authors. Finally, all authors read and approved the final manuscript for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.