
Abstract
Background
In-hospital mortality and discharge disposition following traumatic hip fractures previously reported in the literature, has mainly focused on a nationwide scale, which may not be reflective of unique populations.
Objective
Our aim was to characterize demographics, hospital disposition, and associated outcomes for patients with the most common hip fractures.
Methods
A retrospective study utilizing the Trauma Registry from the Texas Department of State Health Services. Patient demographics, injury characteristics, and outcomes, such as in-hospital mortality, and discharge dispositions, were collected. The data were analyzed via univariate analysis and multivariate regressions.
Results
There were 17,104 included patients, composed of 45% femoral neck fractures (FN) and 55% intertrochanteric fractures (IT). There were no differences in injury severity score (ISS) (9 ± 1.8) or age (77.4 ± 8 years old) between fracture types. In-hospital mortality risk was low but different among fracture types (intertrochanteric, 1.9% vs femoral neck, 1.3%, P = .004). However, when controlling for age, and ISS, intertrochanteric fractures and Hispanic patients were associated with higher mortality (P < .001, OR 1.5, 95% CI 1.1-2.0). Uninsured, and Black/African American (P = .05, OR 1.2, 95% CI 1.1-1.3) and Hispanic (P < .001, OR 1.2, 95% CI 1.1-1.3) patients were more likely to be discharged home after adjusting for age, ISS, and payment method.
Conclusion
Regardless of age, severity of the injury or admission hemodynamics, intertrochanteric fractures and Hispanic/Latino patients had an increased risk of in-hospital mortality. Patients who were uninsured, Hispanic, or Black were discharged home rather than to rehabilitation, regardless of age, ISS, or payment method.
Introduction
Hip fractures are among the most prevalent injuries in the elderly, resulting in substantial morbidity and death.1–4 Additionally, 30% of hip fracture patients die within a year of the injury, 40% cannot walk without assistance, and 33% are dependent or in a nursing home.5,6 Furthermore, increased life expectancy has led to an increased incidence of fractures at the proximal end femoral neck and intertrochanteric region of the femur in aging people. 7 Previously a few studies have reported in-hospital mortality rates of patients with femoral neck and intertrochanteric fractures to range from 1.52%-1.70%.8,9 However, these prior incidence studies have generally been limited to Medicare recipients on a national scale, which may not represent specific geographic regions.
While discharge disposition significantly impacts hip fracture outcomes, discharge to inpatient rehabilitation has reportedly led to improved early mobilization and a lower short-term mortality risk following hip fracture and surgery. 10 In addition, there is mounting evidence that racial and socioeconomic differences in treatment continue to contribute to these outcomes of hip fractures. 11 Subsequently, disparities in access to inpatient rehabilitation facilities exist as minority patients are reportedly more likely to be discharged home than to rehabilitation facilities.12,13
Texas being a unique population, as the second most populated and arguably one of the most diverse states in the United States, with the second-highest Hispanic population in the U.S. of almost 11.2 million and the highest Black population of over 3.9 million. In addition, it surprisingly has the highest number of uninsured residents.14–16 While it is important to recognize that racial and ethnic disparities in orthopaedics have a significant bearing on hip fracture outcomes, 17 prior research has focused mainly on a national basis. As a result, the currernt literature may not be reflective of a diverse, younger, or immigrant patients, such as the Texas population.8,9,17–22 The extent of these fracture outcomes, such as in-hospital mortality and discharge disposition in special populations like Texas, must be identified and characterized order to identify potential disparities that may persist and methods for improving outcomes.
This study aimed to examine in-hospital mortality and discharge disposition among the most frequent types of hip fractures in the geriatric population and identify whether disparities exist among these fractures at the state level. We hypothesized that these fractures' overall in-hospital mortality rates are low but not without disparities regarding racial, ethnic, and socioeconomic differences.
Methods
Database
This retrospective cohort study was performed using the Trauma Registry from the Texas Department of State Health Services for 2018-2021. The Trauma Registry is an online reporting system that collects legislatively mandated data on all EMS runs, traumatic brain injuries, spinal cord injuries, submersions, and other traumatic injuries within Texas’s 22 trauma service designations covering over 254 counties. 23 To our knowledge, this is one of the first studies to analyze hip fractures in the Texas Trauma Registry. Since the Trauma Registry database is a de-identified database, this study was exempt from Institutional Review Board approval.
Study Population
International Classification of Diseases (ICD-10-CM) for fractures of unspecified part of the neck of femur (S72.001-S72.002, S72.009), the base of neck of femur (S72.042-S72.046), mid-cervical fracture of the femur (S72.031-S72.035) and intertrochanteric fractures (IT) (S72.141-S72.146) were used to retrieve fractures in patients over the age of 60 from the 2018-2021 Texas Trauma Registry data file. Fractures involving the neck any portion of the neck were considered as femoral neck (FN) for this analysis. The data was filtered to remove patients with no signs of life on admission and incomplete data. Furthermore, patients who suffered polytrauma were also excluded to prevent confounding of primary outcomes. This was done to ensure that patients reported by the database only reported hip fracture diagnosis codes at admission.
Variables Studied
For baseline clinical characteristics and demographics of the study population, the following variables were collected: age, sex, race (White, Black or Black/African-American, Asian, American Indian or Other), ethnicity (Hispanic and Non-Hispanic), admission vitals, emergency department (ED) mortality, in-hospital mortality, reported number of and specific comorbidities (including, hypertension (HTN), type 2 diabetes mellitus, dementia, chronic obstructive lung disease (COPD), alcohol use disorder (AUD), bleeding disorder, cardiovascular disease (CVD), cirrhosis, anticoagulant use and steroid usage) geographic setting (rural, urban and other), length of intensive care unit (ICU) stay, ED disposition (admitted to the floor, ICU, transferred, and emergently to operating room (OR)), injury severity score (ISS), Glasgow coma scale (GCS), systolic blood pressure (SBP) on admission, hospital disposition (home/self-care, rehabilitation facility, transferred, hospice), and payment method (Medicaid, Medicare, private insurance, self-pay).
Statistical Analysis
The primary outcome of this study was in-hospital mortality. The secondary outcome was racial, ethnic, and socioeconomic influences on mortality or discharge disposition. Statistical analysis was performed using Stata v17.0 (Stat Corp LLC, College Station, TX, USA) and GraphPad Prism v8.0 (GraphPad Software Inc, San Diego, CA, USA). Descriptive data were performed for all data and categorized using fracture types (intertrochanteric fractures vs femoral neck fractures), ethnicity (Hispanic vs non-Hispanic), and race (White, Black, and Asian). A Pearson Chi-squared, Student t-tests, and Mann-Whitney U tests were used as appropriate for univariate comparisons. Data are presented as number and percentage for categorical data and mean and standard deviation (SD) for ordinal data. Statistical significance was defined a priori as P < .05.
Following univariate analysis, a binomial logistic regression was performed to determine a risk prediction model for in-hospital mortality (yes vs no) and hospital disposition (discharge home/self-care vs rehabilitation). In-hospital mortality regressions were controlled for using age, admission SBP, and ISS. Discharge disposition regressions were controlled for using age, ISS, and payment method. Reference values were determined based off the most common variable in the group. Data are reported with n (%) or mean (SD) with odds ratio (OR) and 95% confidence interval (CI). The null OR was set a priori as a value of 1. The cut-off value for the area under the curve (AUC) was .5.
Results
Clinical Characteristics
A total of 17,104 patients were included in the final analysis. Intertrochanteric fractures comprised the majority of fractures (55%), with the remaining classified as femoral neck fractures (45%). Most patients were female (66.8%). There were no differences in age (77.4 ± 8 years old) between fracture types. Regarding race, 90.1% of patients were identified as White, 2.9% as Black/African American, .8% as Asian, and 5.6% as other. In addition, 18.9% identified as Hispanic/Latino ethnicity. Roughly one-third of all patients had at least one reported comorbidity (34.7%); hypertension (HTN) was the most reported comorbidity (35.1%), followed by type 2 diabetes mellitus (T2DM) (14.4%), and dementia (7.4%).
Demographics, Injury Patterns, and Outcomes of Intertrochanteric Fractures and Femoral Neck Fractures.

SD, standard deviation; ISS, injury severity score; ED, emergency department; ICU-LOS, intensive care unit length of stay.
Demographics, Injury Patterns, and Outcomes of Hispanic and Non-hispanic Patients.
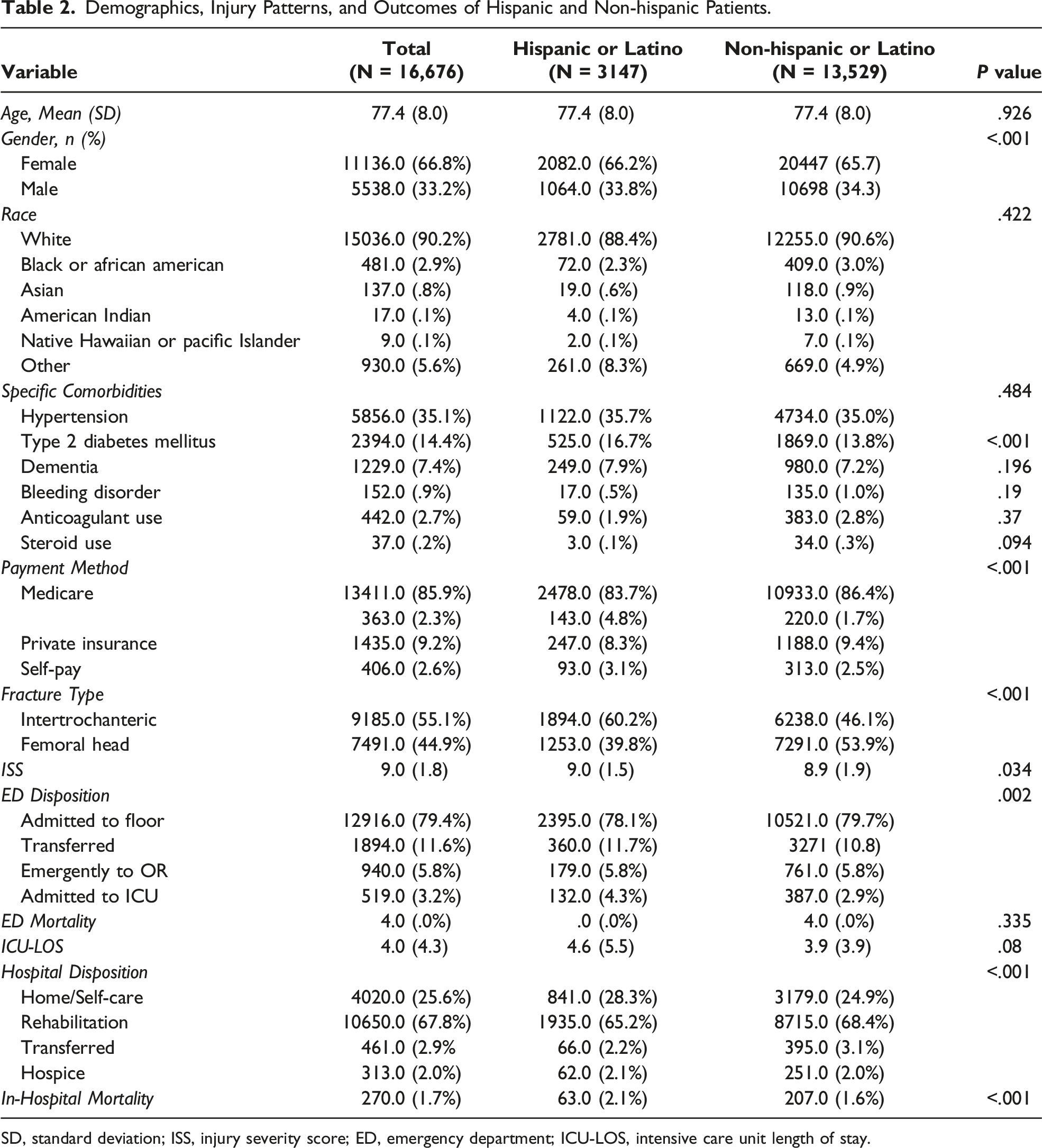
SD, standard deviation; ISS, injury severity score; ED, emergency department; ICU-LOS, intensive care unit length of stay.
Risk Factors Predictive of Emergent Surgery
Most patients were admitted to the floor (79.3%); however, 5.8% went emergently to the operating room, and 3.2% were directly admitted to the intensive care unit. In addition, patients with IT fractures (ref. femoral neck fractures) were more likely to go immediately to the OR (ref. ICU admit) (OR 1.2, 95% CI 1.1-1.3, P = .01).
Risk Factors Associated With in-Hospital Mortality
Demographics, Injury Patterns, and Outcomes Divided by Patient Race.
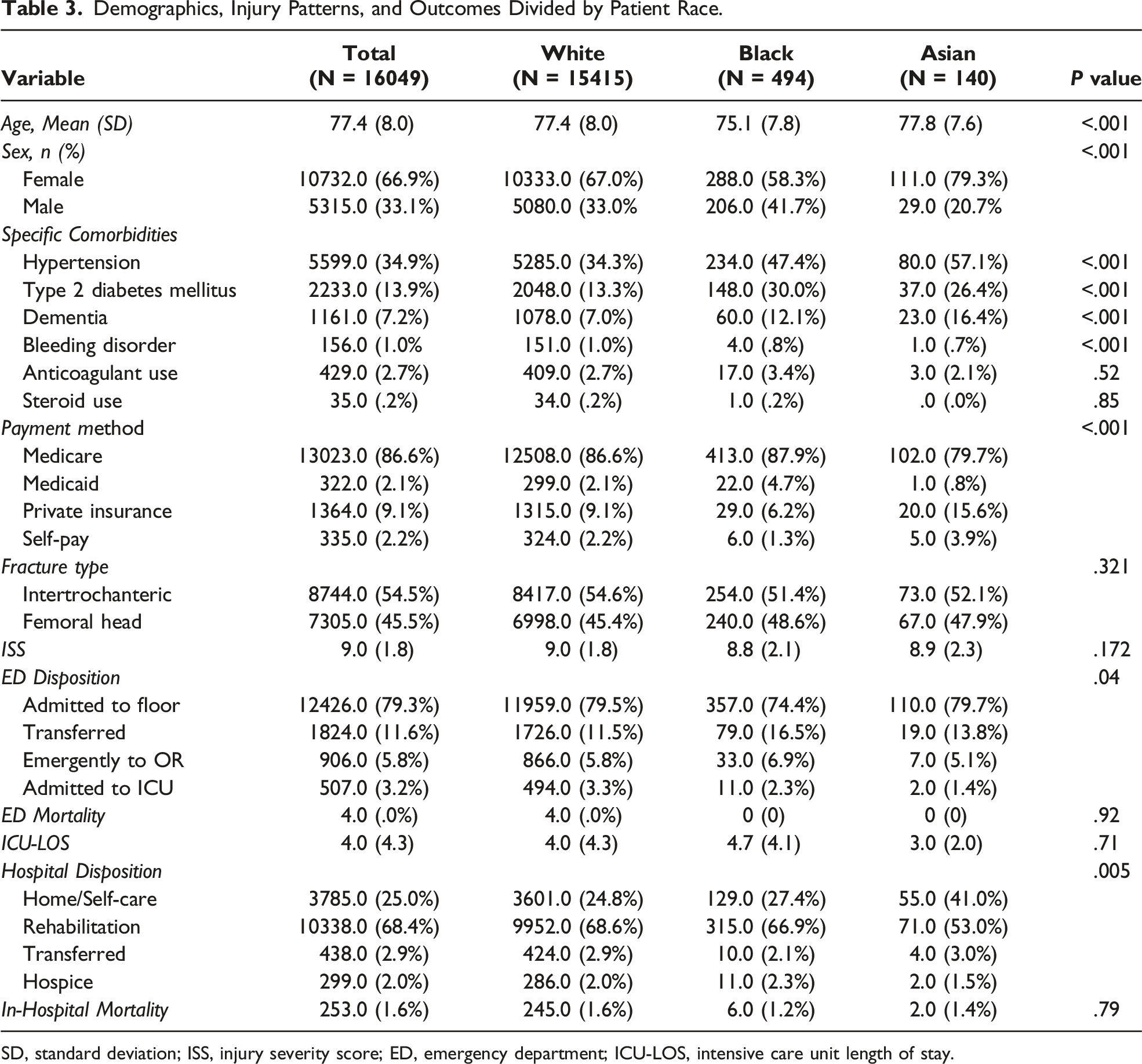
SD, standard deviation; ISS, injury severity score; ED, emergency department; ICU-LOS, intensive care unit length of stay.
Risk of In-Hospital Mortality Adjusted by Age, Injury Severity Score and SBP.

OR, odds ratio; CI, confidence interval; SBP, systolic blood pressure.
Discharge Dispositions
Discharge Disposition Adjusted by Age, Injury Severity Score and Payment Method.
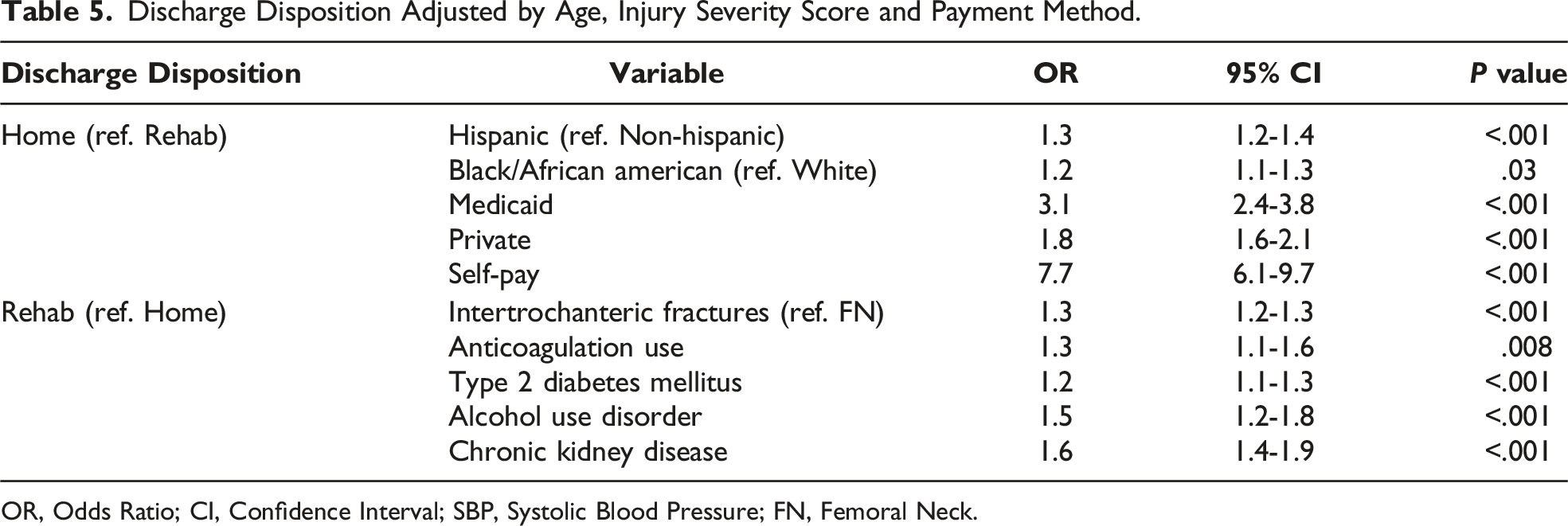
OR, Odds Ratio; CI, Confidence Interval; SBP, Systolic Blood Pressure; FN, Femoral Neck.
Discussion
Although mortality and discharge disposition following traumatic hip fractures have been reported previously in the literature, the bulk of research focus on Medicare recipients nationally, which may not be reflective of specific populations. According to our understanding, more evidence of the in-hospital mortality of these fractures and their related outcomes in unique demographics, such as the Texas population, is needed. Therefore, we aimed to assess the in-hospital risk and discharge disposition of the most common hip fractures and determine if disparities in these fractures persist at the state level.
Our study’s findings report a low in-hospital mortality rate of these fractures consistent with the current literature.8,9 However, we found that disparities in hip fracture care continue to persist between White and minority patients from 2018 to 2021, despite raised awareness and health care initiatives to improve these disparities.21,24,25 Surprisingly, after adjusting for age, ISS, and hemodynamics, Hispanic patients had a significantly higher rate of in-hospital death than non-Hispanic patients. However, no difference was shown between White and non-White patients. A previous study by Amen et al. slightly contrasts these findings. They found no significant difference in-hospital mortality of hip fractures between White and minority populations in their unadjusted analysis. 21 Although they analyzed a larger sample size in a nationwide analysis, their findings may not be as representative of a diverse population as they had a substantially lower percentage of Hispanic patients (5%) compared to ours (19%). Our study is more representative of the unique Hispanic population in Texas, which makes up 40% of its population as it is the second-highest Hispanic population in the country. 15 While it is unclear why this outcome is prevalent in this population, our findings align with the report by the Commonwealth Fund, in that Texas ranks in the 22nd percentile in health systems care due to the state’s poor outcomes in treatment and access to care in Black and Hispanic populations. 26
When considering the impact of comorbidities, hip fracture patients with T2DM, COPD, CKD, and CVD were at higher risk for mortality, consistent with previous studies.1,27–29 Our study did report variability in fracture mortality rates between fracture patterns, as intertrochanteric fractures had a slightly higher risk of mortality than FN fractures in our unadjusted and adjusted analyses. This confirms the magnitude of risk with IT fractures and should not lumped together with FN fractures when considering treatment and post-operative management. 30
When considering discharge disposition, our adjusted analyses demonstrated that IT fractures had a higher rate of being discharged to rehabilitation, which may speak to the increased severity and mortality of these fracture patterns.9,30 When analyzing comorbidities, the number of comorbidities did not influence discharge disposition, while T2DM was the only associated condition that increased the likelihood of being discharged to rehabilitation. This is not surprising due to the additional surveillance and care required of these patients, as diabetes has been shown to increase the risk of mortality after hip fractures.31,32
Another notable finding of this study was the existence of disparities in the discharge disposition between White and minority patients. While Texas represents 19% of the country's uninsured population, 61% of uninsured Texans are Hispanic, and 16% are Black, in which our analysis included a percentage of uninsured patients. 16 To take this into consideration, we adjusted for payment methods to further evaluate the extent of hip fracture outcomes. Specifically, we found that Black and Hispanic patients with the following traumatic hip fractures were more likely to be discharged home than to a rehabilitation facility despite age, ISS, and payment method compared to Whites. These findings are concerning as inpatient rehabilitation after hip fracture surgery has significantly reduced hospital readmissions and lower mortality rates in the short term.33,34 In a similar analysis from 2001-2005, Nguyen-oghalai et al. found that Hispanic patients following hip fractures had 3-fold higher odds of being discharged home to self-care, and Blacks had about 50% higher odds of being discharged home. 20 Furthermore, Amen et al. investigated these hip fracture outcomes from 2006-2015 and found similar results of higher rates of home discharges for these minority populations. 21 This raises a concern that similar outcomes have persisted nationwide since 2001, suggesting a lack of improvement in access and utilization of health care treatment and resources in minority populations, consistent with identified racial disparities in orthopaedic care.20,21,35–38 These outcomes emphasize the historical disparities between Black and Hispanic patients and the underlying complicated, multifactorial causes of these inequalities.
Overall, this study highlights a few essential aspects of hip fracture care that need further evaluation regarding orthopaedic trauma care in Texas. Previously in elective orthopaedic procedures, it has been reported that provider-related factors such as the provider's ability to build meaningful relationships and communication with minorities patients have contributed to the lack of health care utilization in these populations; however, how these factors translate into orthopaedic trauma care is not well understood. 39 Disparities are multifactorial, involving system-level factors such as access to care, provider-level factors including bias, discrimination, and culturally competent communication, and patient-level factors such as cultural beliefs, values, and health behaviors, making these outcomes difficult to address. 40 However, we hope that studies like ours will increase awareness of disparities in orthopaedic trauma care within these vulnerable populations. As awareness continues to improve, it is reasonable to conclude that researchers, hospital organizations and policymakers will seek to fill these knowledge gaps to improve these outcomes.
Limitations
First, the retrospective study included only patients reported over four years. Next, the cause of death, treatment interventions, length of stay, and longer-term outcomes after discharge, including complications and function, are not captured for these patients, and could not be determined. Second, the Texas EMS/Trauma registry does not record discharge-location-specific data such as the length of stay in these facilities. Third, socioeconomic status has been known to affect discharge destinations, and the lack of that data in this database may affect our results. Because these data were unavailable, the authors cannot comment on ways to decrease the mortality rate or mitigate underlying reasons for discharge disposition. Additionally, our findings are dependent on accurate reporting of ICD-10 codes. Finally, these fractures are treated through numerous methods, including total hip arthroplasty, hemiarthroplasty, closed reduction, and percutaneous pinning; these results can be applied broadly to all treatments but are not specific to a single treatment, as the treatment is not reported in the EMS/Trauma registry.
Conclusion
After adjusting for age, ISS, hemodynamics, and payment methods, disparities in hip fracture trauma care persist in regards to in-hospital mortality risk and discharge disposition in Texas’s Hispanic and Black populations. Due to the multifactorial causes of orthopaedic outcomes and health care disparities, as well as the limitations of using a retrospective database, solutions are difficult to suggest. However, this study increases awareness of disparities in orthopaedic trauma care amongst these historically vulnerable populations. Ultimately, efforts to elucidate these specific causes are needed to help improve outcomes in orthopaedic trauma care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.