
Abstract
Objective
To evaluate and compare the 1-year mortality outcomes of elderly patients with hip fractures treated with either hemiarthroplasty (HA) or proximal femoral nailing (PFN), focusing on both intracapsular and extracapsular fractures.
Methods
This retrospective cohort study included 210 patients aged 60 years or older who underwent hip fracture surgery between January 2020 and December 2021. Patients were categorized into three groups: Group 1 (PFN for extracapsular fractures), Group 2 (HA for intracapsular fractures), and Group 3 (HA for extracapsular fractures). Demographic variables, surgical details, and 1-year mortality were analyzed.
Results
The overall 1-year mortality rate was 37.6%. Mortality was lowest in patients treated with PFN for extracapsular fractures and highest in those treated with HA for extracapsular fractures. Older age and male gender were associated with increased mortality, while female gender had a protective effect.
Conclusion
PFN should be considered the preferred surgical approach for elderly patients with extracapsular hip fractures due to its lower mortality and complication rates. HA, while effective for intracapsular fractures, presents higher risks in extracapsular cases. Tailoring surgical strategies to fracture type is essential to optimize patient outcomes.
Introduction
Hip fracture is a severe injury that frequently occurs in older adults after low-energy falls. It is a significant health issue, particularly in the elderly, as it can result in long-term disability, reduced quality of life, and increased healthcare costs. Whether to use hemiarthroplasty (HA) or total hip arthroplasty for elderly intracapsular hip fractures is controversial, but arthroplasty is traditionally preferred. 1 In contrast, osteosynthesis is widely accepted as the treatment of choice for extracapsular proximal femur fractures.2,3 Among osteosynthesis techniques, the proximal femoral nail (PFN) has become the most frequently preferred method for extracapsular hip fractures. However, complications such as nonunion, malunion, femoral head collapse, and limited partial weight-bearing ability have led some surgeons to favor HA in select cases of extracapsular fractures.4-6
There are many studies in the literature comparing HA and osteosynthesis in the surgical treatment of hip fractures.7,8 These studies have primarily focused on extracapsular fractures, examining mortality and clinical outcomes, with differing results. While some report similar mortality rates between techniques, others suggest higher mortality rates in patients treated with arthroplasty.7,8 However, a notable gap exists in the literature: no study has comprehensively examined and compared mortality outcomes for both intracapsular and extracapsular fractures treated with arthroplasty and osteosynthesis. Understanding how fracture type and surgical approach influence mortality is essential for guiding clinical decision-making in this high-risk population.
The objective of this study is to evaluate and compare the mortality outcomes of patients treated with HA or PFN for extracapsular fractures and patients treated with HA for intracapsular fractures. By addressing this gap, this study aims to provide a broader perspective on the interplay between fracture type, surgical technique, and mortality outcomes, offering valuable insights to optimize treatment strategies for elderly hip fracture patients.
Patients and Methods
This retrospective cohort study was conducted in a tertiary orthopedic center. Patient data were obtained from the hospital information system and national registry, covering hip fracture surgeries between January 2020 and December 2021. Additional details were retrieved via telephone contact when necessary. The manuscript was prepared in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cohort studies.
Study Population
The study included all eligible patients who met the inclusion criteria during the study period. Therefore, a priori sample size calculation was not performed
The study included 210 patients aged ≥60 years who sustained either: • An extracapsular proximal femur fracture (AO/OTA 31A1.2, 31A1.3, 31A2) treated with either HA or PFN, • Or an intracapsular fracture treated with HA.
Patients were independently ambulatory before the fracture and had at least one year of follow-up.
The inclusion criterion regarding independent ambulation was chosen to ensure that all participants had a similar level of pre-fracture physical activity, providing a more standardized evaluation of postoperative outcomes.
The exclusion criteria were: • AO/OTA 31A3 fractures, • Pathological or multiple fractures, • Pre-existing arthritis, • Use of supplementary internal fixation devices (eg, cerclage wires, cables, or trochanteric plates) in conjunction with hemiarthroplasty.
Patients were categorized as: Group 1 (PFN for extracapsular hip fracture), Group 2 (HA for intracapsular hip fracture), Group 3 (HA for extracapsular hip fracture).
The detailed patient selection process is illustrated in the study flowchart (Figure 1). Flowchart of the Study.
Surgical Techniques and Perioperative Management
All surgical procedures were performed by the same experienced surgical team to ensure consistency. For patients undergoing hemiarthroplasty, cementless arthroplasty with a bipolar head was utilized. For those treated with proximal femoral nailing (PFN), the Intertan PFN design was used in all cases. Postoperatively, all patients were mobilized with full weight-bearing as tolerated, starting within 48 h after surgery under the supervision of healthcare personnel. In our institution, short-term Intensive Care Unit (ICU) admission (typically <24 h) is a common precautionary practice for elderly patients, based on preoperative assessment by anesthesiologists. Many patients are monitored in a first-level ICU unit located within the operating complex and are transferred to the ward as soon as clinically stable. As institutional protocol, early mobilization is attempted even in ICU-monitored patients, provided their condition permits.
All patients received low molecular weight heparin for thromboprophylaxis for four weeks following surgery. Preoperatively, all included patients were ambulatory without assistive devices and able to perform their daily activities independently, aligning with the inclusion criterion of pre-fracture physical activity independence.
In this study, postoperative blood transfusions were administered according to standardized clinical guidelines specifically tailored for elderly patients with hip fractures.
The primary triggers for transfusion, both before and after surgery, included hemoglobin levels falling below 8 g/dL, symptomatic anemia (eg, shortness of breath, dizziness, tachycardia, or chest pain), significant blood loss exceeding 500 mL, or the need for hemodynamic stabilization. Additionally, patients with cardiovascular or pulmonary insufficiency were also considered for transfusion under these criteria.
For those with a history of cardiovascular disease, a more conservative approach was taken, with transfusions initiated when hemoglobin levels dropped below 10 g/dL. This protocol was designed to optimize oxygen delivery and reduce potential complications, prioritizing safety and positive outcomes for this high-risk elderly population.
Data Collection
The clinical and demographic data collected for this study included the following parameters: • Age, gender, and surgical site, • Time from fracture to surgery, • American Society of Anesthesiologists (ASA) scores, • Presence of comorbidities, • Mortality rate, • Postoperative complications, • Type of anesthesia used, • Blood transfusion rate, • Duration of surgery, • Length of hospital stay, and • ICU admission status.
ASA scores were recorded based on the preoperative evaluations conducted by the attending anesthesiologist, as part of routine anesthesia assessment.
The primary outcome measure of this study was 1-year all-cause mortality following hip fracture surgery. Secondary outcome measures included postoperative complications (such as infection, dislocation, and reoperation), postoperative blood transfusion requirement, ICU admission, and length of hospital stay.
Ethical Considerations
This study was conducted with respect to the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board (IRB) of the authors’ institution prior to initiating the study (IRB decision date and no:01/11/2023, 2023/728). The study protocol ensured the confidentiality and anonymity of patient data by removing all personal identifiers during data collection and analysis. As this was a retrospective study utilizing pre-existing data, informed consent was not required according to the IRB guidelines.
Statistical Analyses
During our data analysis, we presented summary statistics, including frequencies (n) and percentages for categorical variables, as well as mean ± standard deviation (SD) or medians with interquartile range (IQR) for continuous variables. To assess the distribution of the continuous data, we employed a combination of the Shapiro-Wilk test, histograms, and Q-Q plots. Subsequently, we applied various statistical tests, such as the Kruskal-Wallis or Chi-square tests, to compare variables among different surgery groups. For post hoc pairwise analysis, Chi-square test or Dwass Steel Critchlow Fligner (DSCF) test were peformed as appropriate. To investigate mortality predictors, we initially conducted univariate analyses, including the Student t-test, Mann-Whitney U test, Chi-square, or Fisher’s exact test. Subsequently, univariate regression analyses were performed. Finally, multivariate logistic regression analysis was conducted, and Wald test statistics along with hazard ratios (HR) with 95% confidence intervals (95% CI) were reported. All statistical analyses were performed using R-based statistical software, Jamovi Software (version 2.3). We established a significance threshold at P < 0.05 for all tests, considering results with P-values below 0.05 as statistically significant.
Results
The Baseline Characteristics of Patients and Surgeries.

IQR: Inter Quantile Range, ICU: Intensive Care Unit.
A Detailed Comparison of Characteristics Among Three Surgery Groups.

IQR: Inter Quantile Range, ASA: American Society of Anesthesiologists, ICU: Intensive care unit, Post-op: Postoperative. Statistically significant p values shown in bold (p < 0.05).
The median age varied significantly, with Group 1 at 77.0 years (IQR: 67.8-82.5), Group 2 at 83.0 years (IQR: 73.2-86.8), and Group 3 at 84.0 years (IQR: 78.0-88.8) (P < 0.001). The median age of patients in Group 1 was slightly lower than Group 2 and 3 (DSCF test, P = 0.029, and P < 0.001; respectively). Gender distribution, fracture side surgeries, ASA scores, complications, anesthesia types, postoperative transfusions, hospital stay, postoperative hospitalization duration, and 1-year mortality exhibited group-specific variations. Mortality rates in group 1 and group 2 were similar, but mortality in group 3 was higher than the others.
In Group 2, the distribution according to Garden classification was as follows: approximately 9.0% were classified as Garden I, 18.0% as Garden II, 29.5% as Garden III, and 43.6% as Garden IV resulting in nearly 73% of cases presenting as displaced fractures (Garden III and IV combined). However, statistical analysis revealed no significant association between Garden classification and 1-year mortality (P = 0.48).
Comparison of Clinical and Surgical Characteristics Between Survivors and Deceased Patients.

IQR: Inter Quantile Range, ASA: American Society of Anesthesiologists, ICU: Intensive care unit, Post-op: Postoperative. P < 0.05 was considered statistically significant. All statistical tests were two-sided. Statistically significant p values shown in bold (p < 0.05).
aFisher Exact Test.
Univariate and Multivariate Analysis of Predictors for 1-Year Mortality in Elderly Patients Undergoing Hip Fracture Surgery.
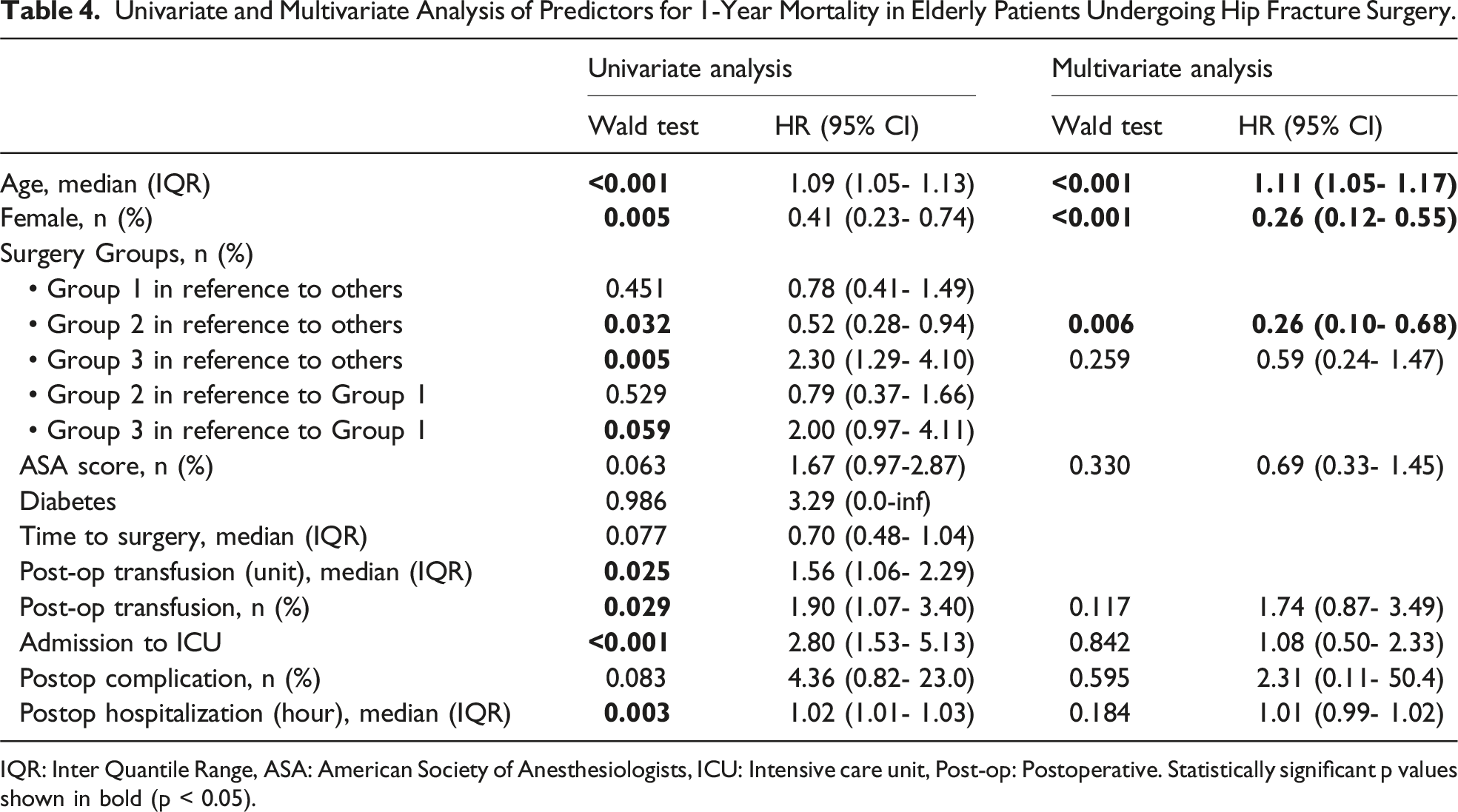
IQR: Inter Quantile Range, ASA: American Society of Anesthesiologists, ICU: Intensive care unit, Post-op: Postoperative. Statistically significant p values shown in bold (p < 0.05).
Age consistently emerged as a robust predictor, with each additional year associated with a 9% higher risk in the univariate analysis (Wald test P < 0.001; HR = 1.09, 95% CI: 1.05-1.13) and a slightly higher risk in the multivariate analysis (P < 0.001; HR = 1.11, 95% CI: 1.05-1.17). Female gender exhibited a protective effect, with a statistically significant hazard ratio of 0.41 (95% CI: 0.23-0.74, P = 0.005) in the univariate analysis and a more pronounced effect (HR = 0.26, 95% CI: 0.12-0.55, P < 0.001) in the multivariate analysis. Surgical group classifications revealed distinctive risk patterns, with Group 2 indicating a lower risk (P = 0.032; HR = 0.52, 95% CI: 0.28-0.94) and Group 3 associated with a higher risk (P = 0.005; HR = 2.30, 95% CI: 1.29-4.10) in the univariate analysis. These associations persisted in the multivariate analysis only for Group 2 (P = 0.006; HR = 0.26, 95% CI: 0.10-0.68).
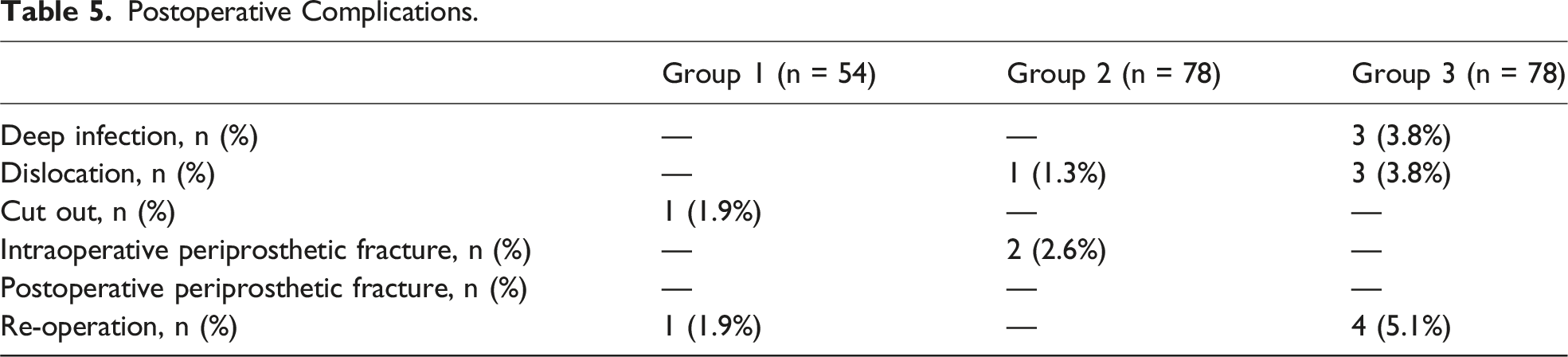
Postoperative Complications.
Discussion
This study examined 1-year mortality in elderly patients with hip fractures, focusing on both fracture type and surgical approach. Among patients with extracapsular fractures, PFN (Group 1) was associated with lower mortality and fewer complications than HA (Group 3). When HA was used for intracapsular fractures (Group 2), mortality was significantly lower than in Group 3, despite similar demographic and clinical characteristics. These findings suggest that fracture morphology, in combination with the surgical burden of HA, may contribute to poorer outcomes in extracapsular cases.
There remains a lack of consensus in the literature regarding the optimal treatment for extracapsular hip fractures. Çiloğlu et al reported that HA may be linked to lower mortality and fewer complications in such fractures. 9 However, most evidence supports PFN due to its biomechanical stability and reduced surgical trauma. 9 Our findings align with this consensus. Although functional scores were not evaluated in this study, mortality differences highlight the need to tailor surgical interventions to the fracture type and the physiological status of elderly patients.10–13
Studies comparing PFN and HA have demonstrated improved morbidity profiles with PFN, even though early postoperative recovery may be better with HA.14-16 Görmeli et al also found lower 1-year mortality with PFN despite better early function with HA. 17 Similar conclusions were drawn in studies comparing PFN, HA, and sliding hip screws, where HA was associated with higher short- and long-term mortality. 18 The significantly higher mortality in Group 3 likely results from both procedural complexity and fracture characteristics. HA for extracapsular fractures typically requires wider incisions, greater soft tissue dissection, and longer operating times, which impose additional physiological stress. To isolate the effect of fracture type from patient health status, we compared these patients to Group 2, who underwent the same procedure but had intracapsular fractures. Despite similar age, ASA scores, and comorbidities, Group 3 showed substantially higher mortality. This reinforces the role of fracture morphology and surgical complexity in patient outcomes.
Regression analyses confirmed that age and male sex were independent predictors of mortality. While the impact of HA in extracapsular fractures diminished in multivariate models, the trend remained. This supports the idea that fracture location and surgical invasiveness influence mortality beyond baseline health factors. Dementia, analyzed separately, showed no significant correlation with mortality or treatment group allocation.
Regarding the treatment of displaced femoral neck fractures, the choice between THA and HA remains debated. While THA is increasingly favored for its superior long-term outcomes, HA is still commonly used, particularly in older adults where minimizing operative time and surgical stress is a priority. A recent international analysis by Foote et al demonstrated that the decision between THA and HA is nearly evenly split globally, with each option representing approximately 50% of surgical treatments for geriatric displaced femoral neck fractures. 19
In our institution, HA is the standard approach for patients over 70 years of age, regardless of pre-fracture ambulatory status. Therefore, the use of HA in this cohort should not be interpreted as a proxy for poor functional baseline but as a reflection of institutional guidelines. The elevated mortality in certain subgroups likely reflects procedure-related burdens rather than selection bias for frail patients.
Overall, our study highlights the importance of selecting the appropriate surgical technique based on fracture type. PFN appears to offer clear advantages in extracapsular fractures due to reduced operative trauma and preservation of the native bone structure. In contrast, HA, though effective for intracapsular fractures, presents higher risks when applied to extracapsular cases. Nonetheless, HA remains an essential option in revision settings, such as after failed PFN.
Interestingly, the median hospital stay in our cohort was only two days, even though nearly one-third of patients were temporarily monitored in the ICU. This brief hospitalization duration reflects our institutional and national healthcare strategies, which prioritize early discharge supported by home-based rehabilitation services. In our country, elderly patients are commonly cared for at home by family members, with support from a well-structured national home healthcare system that provides postoperative wound care, physical therapy, and medical supervision. Importantly, all patients included in this study were independently ambulatory prior to fracture and surgery, ensuring a relatively high level of pre-fracture functional capacity. Postoperative discharge decisions were made only for patients whose vital signs were clinically stable, in accordance with institutional protocols. While such a short hospital stay may seem unusual from an international perspective, it has not been associated with increased early mortality or hospital readmissions in our cohort. This practice highlights the importance of adapting perioperative management strategies to the sociocultural context and available healthcare infrastructure.
Our findings also emphasize the anatomical and biomechanical differences between intracapsular and extracapsular fractures. HA-treated intracapsular fractures showed more favorable outcomes. This suggests a lower physiological burden associated with the procedure in this context. Treatment decisions should thus consider both fracture characteristics and individual patient factors.
Study Limitations: This study has limitations inherent to its retrospective and single-center design, which may restrict generalizability. Functional outcomes and quality-of-life metrics were not assessed. A priori power analysis was not performed, as all eligible patients within the study period were included. Although ASA scores and comorbidities were similar across groups, unmeasured confounders may still have influenced outcomes. Additionally, comprehensive indices such as the Charlson Comorbidity Index could not be applied, and cancer history was not reliably available due to incomplete records. These factors limit our ability to fully assess long-term prognostic influences.
Future multi-center prospective studies with larger patient cohorts and functional evaluations are warranted to validate our findings and further explore cognitive and clinical outcomes associated with different surgical techniques.
By including patients treated with both HA and PFN across intracapsular and extracapsular fracture types, this study offers a practical perspective on optimizing surgical decisions in elderly hip fracture patients. Individualized approaches that consider fracture morphology and surgical invasiveness are essential to improving survival and recovery in this high-risk population.
Conclusion
PFN should be prioritized as the first-line treatment for extracapsular hip fractures due to its lower mortality and complication rates compared to HA. While HA shows lower mortality in femoral neck fractures, it is associated with higher mortality in extracapsular fractures. These findings highlight the importance of tailoring surgical decisions to fracture type to improve outcomes in elderly patients.
Footnotes
Ethical Statement
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection were performed by Fatih Günaydın, Yusuf Bayram. Analysis were performed by Mahmud Aydın and Ali Çelik. Fatih Günaydın wrote the first draft of the manuscript and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.