
Abstract
Introduction:
The aim of this study was to determine the diagnostic value of single-photon emission computed tomography/computed tomography (SPECT/CT) in prediction of avascular necrosis (AVN) after femoral neck fracture and to evaluate whether photon defect in femoral head as seen in SPECT/CT can be an index for choice of surgical method.
Methods:
This study was based on 97 patients who took SPECT/CT after femoral neck fracture from November 2012 to November 2017, with 64 patients with femoral intertrochanteric fracture in which chances of AVN is rare as a comparison group. Among 97 patients with femoral neck fracture, osteosynthesis was conducted in 7 patients with less than 15% of photon defect in damaged femoral head and 7 patients who wanted osteosynthesis, despite photon defect more than 15%, and 83 patients with photon defect more than 25% had arthroplasty. Patient with osteosynthesis was followed up with AVN by conducting magnetic resonance imaging (MRI) in 1 year after the surgery.
Results:
Quantitative analysis of SPECT/CT in 14 patients who had femoral neck osteosynthesis showed that 7 patients with femoral neck fracture showed photon defect of 15% or more, but less than 25% and 3 patients in these were diagnosed with AVN after 1-year follow-up by MRI. Sensitivity and specificity of SPECT/CT in predicting AVN was 100% and 63.6%, respectively, with prediction accuracy of 71.4%. Among 14 patients with femoral neck fracture who had osteosynthesis, photon defect in 3 patients diagnosed with AVN was 19.6% ± 5.2%, but photon defect in 11 patients who was not diagnosed with AVN was 10.7% ± 5.2%, showing statistically significant difference between 2 groups (P = .001).
Conclusion:
Single-photon emission computed tomography/CT in patients with femoral neck fracture is considered to have diagnostic value in predicting occurrence of AVN, and percentage of photon defect is considered to be an useful index in determining the operative method.
Backgrounds
Femoral neck fracture is common fracture in elderly patients, with its incidence rising due to recently growing traffic accidents and aging. It obligates significant economic burden during its treatment, and successful treatment is crucial due to the risk of complication. 1 Treatment for femoral neck fracture can be performed in 2 methods: osteosynthesis and arthroplasty, and the choice of surgical method is based on degree of fracture displacement and age. 2 Femoral neck fracture in young patient is treated with osteosynthesis regardless of displacement, but there are some controversies in treating displaced fracture in elderly patients. 3 Femoral neck fracture in elderly patients requires early ambulation and rehabilitation to prevent various complications related to prolonged immobility, and as the blood vessels to femoral head are damaged in the course of injury, osteosynthesis can result in complications such as avascular necrosis (AVN) or nonunion. 4 Consequently, many authors recommend primary arthroplasty for femoral neck fracture in elderly patients. 5 The risk of AVN after osteosynthesis for femoral neck fracture is about 10% to 15% for nondisplaced fracture whereas 30% to 35% for displaced fracture. Such incidence of complication calls for secondary surgeries such as revision surgery and arthroplasty, imposing an economic and physical burden for patients. 6
Especially, AVN can be diagnosed with clinical symptoms and simple radiologic images, but symptoms occur only after necrosis is progressed, and it must be at least 4 to 6 months past circulatory disorder in femoral head in order to see AVN in simple radiologic image. 7 Predicting AVN after treatment of femoral neck fracture is important in determining surgical method. Bone scan, computed tomography (CT), and magnetic resonance imaging (MRI) are being used to predict AVN with difficulty of diagnosis after the injury, but there are problems with accuracy and high cost.
Single-photon emission computed tomography (SPECT) is known to be excellent in evaluating blood supply to femoral head, better than planar bone scan. But its image prescription is dismal, and it cannot provide accurate anatomical information, reducing specificity. Single-photon emission computed tomography/CT that combines both images from SPECT and CT using hybrid camera has improved specificity than previous SPECT and can identify anatomical location of abnormal area and severity of the injury. 8
This study was aimed to investigate advantage of SPECT/CT compared to conventional nuclear medicine imaging by performing SPECT/CT on patients diagnosed with femoral neck or intertrochanteric fracture before surgery and provide approaches to quantitatively measure blood supply to the femoral head. And this study was performed to determine the diagnostic value of SPECT/CT in prediction of AVN after femoral neck fracture and to evaluate whether photon defect in femoral head as seen in SPECT/CT can be an index for choice of surgical method.
Methods
Patients
This study was based on 97 patients who took SPECT/CT after femoral neck fracture from November 2012 to November 2017, with 64 patients with femoral intertrochanteric fracture in which chances of AVN are rare as a comparison group. Average period of follow-up was 16 (12-56) months, with average age of 75.4 (16-93). Most common cause of hip fracture was fall (155 patients) followed by traffic accident (6 patients). Twenty-eight patients were Garden type 1 fractures, 15 were Garden type 2 fracture, 12 were Garden type 2 fracture, and 42 were Garden type 4 fracture. Treatment method for femoral neck fracture was decided by patients and guardians after enough explanation on osteosynthesis and arthroplasty. Among patients who took surgery for femoral neck fracture, those who did not take SPECT/CT before surgery or those who had not been followed up less than for 1 year were excluded from the study. Any patients who had arthroplasty in contralateral side or internal metal implant were also excluded. This study was conducted after letter of consent was acquired for participation of the study after enough explanation in advance with the approval from medical research ethics committee.
Among 97 patients with femoral neck fracture, osteosynthesis was conducted in 7 patients with less than 15% of photon defect in damaged femoral head and 7 who wanted osteosynthesis despite photon defect more than 15% and 83 patients with photon defect more than 25% had arthroplasty. Among 83 patients who had arthroplasty, total hip arthroplasty was conducted in patients less than 70 years old or high demand level of activity, and hemiarthroplasty was conducted in patients more than 70 years old or low demand level of activity.
Among 64 patients diagnosed with femoral intertrochanteric fracture, osteosynthesis was conducted in 49 patients with less than 15% of photon defect and 4 patients who wanted osteosynthesis, despite more than 15% of photon defect. Six patients with more than 25% of photon defect and 5 patients who could not anticipate successful internal fixation due to comminuted fracture or terrible bone quality had hip arthroplasty (Figure 1).

Flow diagram.
Informed consent was waived due to the retrospective nature of the study and anonymous clinical data. This study was approved by the institutional review boards of Inha University Hospital.
Evaluation
Patients who were diagnosed with femoral neck fracture or intertrochanteric fracture had SPECT/CT within 48 hours after admission. Single-photon emission computed tomography/CT image was taken in 3 hours after administering technetium-99m (Tc-99m) hydroxymethylene diphosphonate. Symbia T6 model (Siemens Medical Solutions USA, Hoffman Estates, Illinois), a dual head γ camera with 2 detectors, was used to take image after placing both hip joints symmetrically. Acquired axial, sagittal, and coronal images were convenient for detecting photon defect from loss of blood flow.
Analysis of the SPECT/CT results was performed in quantitative method. For quantitative evaluation of femoral head, blood flow was performed with work station, which is used in radiology image room. As radiologic image test is influenced by amount of injected radiologic nuclide, interval from injection to test, biodistribution which is dependent on liver and kidney function, there may be difference according to individual, despite normal blood flow in femoral head. Therefore, in this study, the results were analyzed not with absolute quantification but with comparative quantification using following technique to compensate such individual difference. First, CT image of SPECT/CT was used to establish region of interest (ROI) that did not invade cortical bone but includes trabecular bone as much as possible with femoral head as circle. And axial, sagittal, and coronal images in SPECT image that corresponded to established ROI were measured of average bone scan uptake rate to calculate average of results from 3 images. Average bone scan uptake rate in healthy femoral head was measured in identical manner, then ratio of uptake rate in damaged side to that in healthy side was calculated in percentage (100 × affected/unaffected femoral head), and then it was subtracted from 100 to be defined as photon defect (Figure 2). Patients were followed up in 6 weeks, 3 months, 6 months, and 1 year after surgery. After 1 year, the patients visited hospital every year for simple radiologic test and clinical evaluation to follow-up on AVN. Patient with osteosynthesis was followed up with AVN by conducting MRI in 1 year after the surgery.

Photon defect: measurement of radioactivity (femoral head).
Surgery and Post-Surgery Management
All the surgeries were performed by the author alone. When multiple pinning was performed in femoral neck fracture, 4 to 6 cm of skin incision was made in lateral proximal thigh. Iliotibial band and gluteus medius muscle was made an incision in same direction as skin incision, then after reaching external trabecular bone. Three cannulated screws were parallelly inserted 5 mm into subchondral bone of femoral head in reverse triangle shape just under vastus lateralis line. To prevent displacement of bone fragment after surgery, it was inserted so that it could have 3-point fixation that can connect external femoral cortical bone, lower femoral neck cortical bone, and femoral head subchondral bone. Weight bearing was restricted for at least 6 weeks after surgery.
When conducting reduction and internal fixation for intertrochanteric fracture, proximal femoral nail antirotation (PFNA, AO Synthes, Oberdorf, Switzerland) was selected. Closed reduction was attempted under image intensifier, and after making about a 5-cm incision at apex of greater trochanter, entry point for nail was created by awl and guiding pin was inserted to the medullary canal. After reaming medullary canal 2 mm larger, nail was inserted, and guiding pin was inserted via proximal sleeve of targeting device. After placing lag screw on the pin, set screw was tightened and then was untightened about 1/4 for gliding. After inserting lag screw, transverse screw was fixated in distal femur. Weight bearing was restricted for at least 6 weeks after surgery.
As for total hip arthroplasty in femoral head and intertrochanteric fracture, summit system, noncement type, was used for femoral stem, and Depuy Pinnacle Acetabular Cup (Warsaw, Indiana) was used for acetabular cup. Two implants were fixated with compressed fixation, and BIolox delta, fourth-generation ceramic, was used for articular surface. As for bipolar hemiarthroplasty, summit system was used, and surgery was conducted to achieve press-fit in proximal metaphysis. Prophylactic antibiotics were administered 1 hour before surgery, and posterior external approach was used. Drainage was removed in 1 to 2 days after surgery. Ambulation was allowed with walker or crutch from the day of removal. Suture was removed in 2 weeks after surgery, then the patients were discharged with walker or crutch.
Statistical Analysis
Based on final follow-up results after osteosynthesis, the patients were grouped into a group with AVN and group without AVN. Sensitivity and specificity of AVN prediction with quantitative femoral head blood flow evaluation were calculated by cross analysis. Continuous variables such as age, bone mineral density (BMD), body mass index (BMI), average bone scan uptake, and bone scan consumption were analyzed with Mann-Whitney U test to compare differences in the 2 groups. Categorical variables such as sex and fracture classification were analyzed with Fisher exact test. The results were analyzed statistically by SPSS with significance level of P < .05.
Result
Quantitative analysis of SPECT/CT in 14 patients who had femoral neck osteosynthesis showed that 7 patients with femoral neck fracture showed photon defect of 15% or more, but less than 25%, and another 7 patients with femoral neck fracture showed that of less than 15%. In 7 patients with photon defect of 15% or more, but less than 25%, 3 patients were confirmed with AVN. Seven patients with photon defect less than 15% all showed union. There was no significant difference in sex, BMD, and BMI between 3 AVN patients and the other 11 patients. However, average age of AVN group was 55.3 years which was statistically significantly lower than 75.1 years of non-AVN group (P = .043, Table 1). Two patients in AVN group were Garden type 3 and 1 patient was Garden type 4. Period till developing AVN was 2, 6, and 6 months. After AVN was confirmed, 1 patient had total hip replacement arthroplasty (THRA) and 2 patients were advised to have surgical treatment, but they did not show specific symptoms and want surgical treatment and were followed up ever since (Figure 3; Table 2). AVN was not observed in 53 patients with intertrochanteric fracture who had osteosynthesis.
Demographic Data of Patients Treated by Osteosynthesis.

Abbreviations: AVN, avascular necrosis; BMD, bone mineral density; BMI, body mass index.
a Values are presented as number.

A, Preoperative radiograph shows a Garden type III femoral neck fracture. B, Preoperative SPECT/CT shows photon defect on affected side (affected/unaffected femoral head uptake ratio = 0.28). C, Immediate postoperative radiograph shows well-reduced femoral neck with cannulated screw. D, Postoperative 2-month follow-up radiograph shows mild femoral head collapse and AVN was diagnosed. AVN indicates avascular necrosis; SPECT/CT, single-photon emission computed tomography/computed tomography.
AVN Patients Treated by Osteosynthesis.
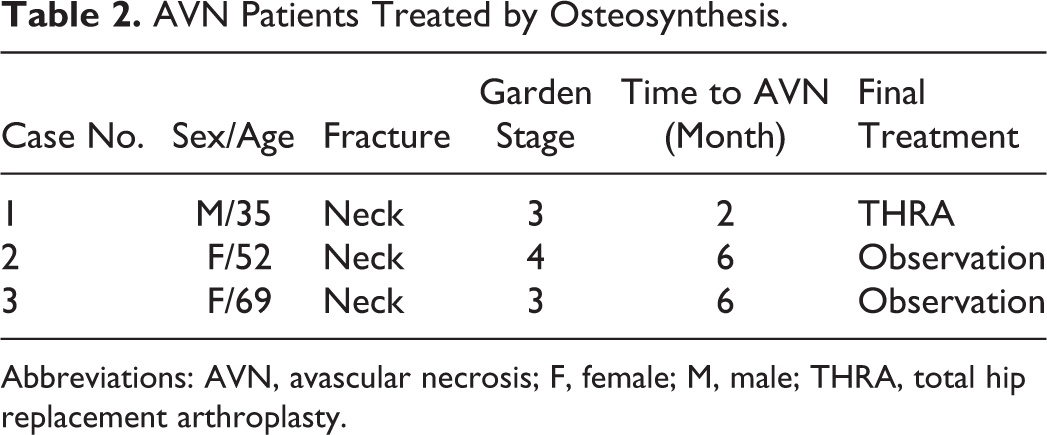
Abbreviations: AVN, avascular necrosis; F, female; M, male; THRA, total hip replacement arthroplasty.
Sensitivity and specificity of SPECT/CT in predicting AVN were 100% and 63.6%, respectively, with prediction accuracy of 71.4% (Table 3). Among patients with femoral neck fracture who had osteosynthesis, photon defect in 3 patients diagnosed with AVN was 19.6 ± 5.2%, but 11 patients who were not diagnosed with AVN showed photon defect of 10.7 ± 5.2%, showing statistically significant difference between 2 groups (P = .001).
2 × 2 Contingency Table Used for Calculation of the Sensitivity and Specificity in Patients Treated by Osteosynthesis.

Abbreviation: AVN, avascular necrosis.
Average photon defect depending on Garden classification type was 10.3 ± 5.2 for type 1, 14.1 ± 7.9 for type 2, 20.0 ± 9.4 for type 3, and 24.9 ± 4.3 for type 4. Average photon defect of type 1 and 2 was 12.8 ± 6.3, whereas average photon defect of type 3 and 4 was 21.8 ± 9.6. There was statistically significant difference between average photon defect of Garden type 1 and 2 and Garden type 3 and 4 (P < .05). The percentage of photon defect showed negative correlation with Garden classification with R 2 value of .29, P < .05.
Discussion
Early evaluation of femoral head avascularity after femoral neck fracture is a crucial factor in decision for treatment method of the fracture, and although medical imaging tests have been developed to evaluate viability of femoral head after femoral neck fracture, there has been consistent attempts to find more simple and accurate method. Mitchell et al have reported that MRI is known as the best test in early diagnosis of AVN and in a comparative study of MRI, CT, and bone scan in their diagnostic value. 9 However, MRI must be taken for a long time in same position and high costs. Kim et al have reported that SPECT has its diagnostic value as screening test with its excellent diagnostic accuracy better than bone scan, accuracy close to MRI, and low cost. 10 Recently, SPECT/CT that integrates SPECT and CT using hybrid camera technique has been developed, and SPECT/CT was used in this study as it has increased specificity and can accurately identify anatomical location and severity of injury. Lee has reported that femoral head blood flow evaluation by SPECT/CT in patients with femoral neck fracture can be a treatment protocol for predictive factor of AVN, since it can accurately evaluate blood flow in femoral head and predict AVN with quantitative evaluation. 11
In 1984, Holmberg and Thorngren have reported that 117 patients with femoral neck fracture showed osteosynthesis regardless of displacement of fracture when uptake ratio of affected to unaffected femoral head is 0.90 or higher in bone scan using Tc-99m methylene diphosphonate before surgery, but the ratio lower than 0.9 is associated with high complications rates. 12 When determining the operative method based on percentage of bone scan intake ratio, there is not yet an established standard for in what percentage we should disregard osteosynthesis but consider hip arthroplasty. In our study, when blood flow loss has been defined if photon defect is 15% or greater, sensitivity of AVN prediction is 100%, whereas specificity, 56%, with predictive accuracy of 67%. Generally, if photon defect is 15% or higher, it is recommended that osteosynthesis is disregarded, and hip arthroplasty must be considered as primary treatment and if it is lower than 15%, osteosynthesis would be preferred. However, factors such as Garden classification, patient’s age, underlying disease, and time until the surgery must be considered to determine the operative method between osteosynthesis and hip arthroplasty.
According to Shah et al, greater displacement of femoral neck fracture poses higher risk of AVN complications. 2 In this study, Garden type 3 and 4 fractures with greater displacement has shown significantly lower percentage of bone scan uptake than Garden type 1 and 2, which it has been confirmed that percentage of bone scan uptake has negative correlation with displacement. Quantitative evaluation of perfusion in femoral head has confirmed that greater displacement of femoral neck fracture causes higher risk of AVN complication, and SPECT/CT is considered to have sufficient value in diagnosing AVN.
With SPECT/CT, perfusion state of femoral head can be evaluated objectively before surgery, and predictive accuracy of AVN is improved. A certain treatment protocol for displaced femoral neck fracture in elderly patients is not yet established, so determining the operative method is based on subjective experience of surgeon and clinical preference. Therefore, quantitative blood flow evaluation with SPECT/CT can serve as a protocol for treating patient as a predictive factor of AVN and simultaneously make decision-making process of treatment more rational and objective. However, its low specificity and predictive accuracy requires routine MRI follow-up on AVN.
Avascular necrosis incidence after intertrochanteric fracture is very rare with 0.3% to 0.8%, 13 -15 but there has been reports that actual AVN incidence would be higher because patients are old, have many underlying diseases, and are difficult to follow-up. 16,17 In our study, AVN was not observed in 53 patients with intertrochanteric fracture who had osteosynthesis.
Limitations in this study, first, is that there are a few cases of having osteosynthesis in femoral neck fracture because all the operations were performed by 1 surgeon in a single center. However, this study has confirmed positive possibility of SPECT/CT of predicting AVN, and further study in large scale is necessary. Second, our study could not make actual comparison between displaced fracture patients with photon defect of 25% or more and nondisplaced fracture patient with photon defect of less than 25%. In order to compare the groups, Garden type 3 or 4 patients with greater displaced fracture and higher photon defect must have osteosynthesis instead of arthroplasty to confirm incidence of AVN, but since it was predicted that it would bring poor outcome to patient, it was dismissed. Third, in order to quantitatively measure bone scan uptake ratio in CT image of SPECT/CT, sagittal, coronal, and axial image in SPECT image which corresponds to established ROI have been measured of ROI, respectively, and an average of 3 measurements has been calculated. However, there is limitation to precise measurement, as uptake rate can be exaggerated when it is measured based on the largest plane because blood flow to femoral head decreases from femoral head and blood flow to femoral head cannot be evaluated in 3D. Recently, devices that can measure femoral head bone scan uptake in 3-dimension are being developed, which promises more accurate quantitative measurement.
Conclusion
Single-photon emission computed tomography/CT in patients with femoral neck fracture is considered to have diagnostic value of predicting occurrence of AVN, and percentage of photon defect is considered to be a useful index in determining the operative method. However, the test has low specificity, and AVN must be followed up with routine MRI. Further large-scale study is wanted to learn significance of SPECT/CT in intertrochanteric fracture.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Inha University research grant.