
Abstract
Objective
Preoperative frailty and surgical waiting times are associated with the occurrence of adverse outcomes in patients with hip fractures. Specifically, we aimed to investigate the influence of frailty status and surgical timing on the risk of serious adverse events during hospitalization.
Methods
This study utilized an observational single cohort design and included patients aged ≥60 years with a primary diagnosis of hip fracture. Frailty was assessed using the chart-derived frailty index (CFI), which was calculated based on demographic and routine laboratory variables. The primary outcome of interest was the occurrence of in-hospital serious adverse events. A multivariate logistic regression model was utilized to examine the risk factors influencing outcomes.
Results
The study included 427 participants, with a mean age of 80.28 ± 8.13 years and 64.2% of whom were female. Patients with high CFI have more comorbidities (P < .001), lower surgical rates (P = .002), and delayed surgical times (P = .033). A total of 239 patients (56.0%) experienced serious adverse events. The high CFI group had a significantly higher occurrence of serious adverse events compared to the low CFI group (73.4% vs 48.5%, P < .001). After adjusting for surgical timing and covariates, the multivariate logistic regression analysis revealed that high frailty significantly increased the risk for serious adverse events (OR = 2.47, 95% CI 1.398-4.412), infection (OR = 1.99, 95% CI 1.146-3.446), acute heart failure (OR = 3.37, 95% CI 1.607-7.045). However, the timing of surgery did not demonstrate any association with these outcomes. In addition, after adjusting for surgical factors, high CFI remains an independent risk factor for these complications.
Conclusions
Frailty serves as a reliable predictor of the probability of encountering severe adverse events while hospitalized for elderly individuals with hip fractures. This method has the potential to pinpoint particular modifiable factors that necessitate intervention, whereas the impact of surgical timing remains uncertain and necessitates additional research.
Introduction
Hip fractures are a highly detrimental injury in the elderly population. 1 Surgical therapy is the preferred approach for treatment. 2 Despite advancements in surgical and anaesthetic techniques, the occurrence of postoperative complications and mortality remains a significant obstacle to successful patient outcomes and increased costs. 3 Given that the majority of morbidity and mortality is attributed to underlying medical conditions rather than the fracture itself, it is crucial to stratify and effectively manage risk factors associated with adverse consequences. 4
In conventional risk management, the timing of surgery has been the primary focus. Based on international clinical practice guidelines, it is recommended that acute hip fractures undergo surgical intervention within 24-48 hours of admission, 5 as delays in surgery have been shown to elevate the likelihood of complications.6-8 On the other hand, Varady et al 9 recently demonstrated that delayed time to surgery was not independently associated with increased 30 day complications for patients with pathologic hip fractures. Bovonratwet et al 10 also argued that surgery within 2 days of hospital arrival was not associated with reduced complications or death for patients with periprosthetic hip fractures. These controversial findings complicate decision making for older patients with hip fractures, who have more complicated medical conditions.
In addition to timing, frailty status has emerged as a crucial factor influencing outcomes.11,12 Literature suggests that over half of hip fracture patients exhibit frailty, which amplifies the risk of adverse consequences such as postoperative pneumonia, 13 prolonged hospitalization, 14 and diminished quality of life, 14 as well as higher morbidity and mortality.10,12,14,15 An explanation for this predictive capability can potentially be attributed to diminished physiological reserves, compromised immune function, and the presence of multiple chronic conditions. 16 The evaluation of frailty can offer valuable insights into the elderly population’s capacity to maintain homeostasis and cope with stress. Both the American College of Surgeons (ACS) and the American Geriatrics Society (AGS) advocate for the inclusion of frailty assessments in the preoperative evaluation of older adults. However, frailty assessment tools require extra effort for clinical management. The chart-derived frailty index (CFI) uses routine lab values to predict surgical risk in older adults.14,17 Additionally, modifiable factors such as anemia and malnutrition can impact a patient’s recovery after surgery.
The significance of preoperative frailty assessment and reduced surgical waiting times in enhancing the outcomes of hip surgery in older patients has been extensively explored in prior research. Nevertheless, the prevailing factors that exert the most influence remain uncertain, as various studies have yielded conflicting findings. Consequently, it is imperative to conduct standardized investigations to elucidate the impact of frailty status and surgical timing on perioperative outcomes in elderly individuals with hip fractures. This study aims to assess the predictive value of a composite frailty score (CFI) and surgical timing in determining the occurrence of perioperative Serious Adverse Events (SAEs) during hospitalization.
Methods
Study Design and Data Collection
An observational cohort study was conducted at the Orthogeriatric Unit of our hospital between November 2020 and March 2022. The study included consecutively admitted participants aged ≥60years with a primary diagnosis of hip fracture. Exclusion criteria comprised patients with incomplete medical histories or life-threatening severe multiple organ dysfunction. The study protocol received approval from the Ethics Committee of our Institution, and all patients provided written informed consent prior to participation. Demographic data, comorbidities, frailty status, and hospitalization information, surgery wait times (hours from presentation to surgery) and surgical procedure and perioperative complications were retrieved using an electronic medical record.
Frailty Assessment
Before surgery, the frailty status of all participants was assessed using the chart-derived frailty index (CFI) based on Amrock et al’s method. 17 The CFI was calculated using 5 specific conditions: age>70 years, preoperative BMI <18.5 kg/m2, hematocrit <35%, albumin<34 g/L, or serum creatinine>176.8 μmol/L (2.0 mg/dL), with each condition earning 1 point. A higher CFI score indicates greater frailty. Based on published criteria, patients were categorized into high CFI (CFI, 3-5) and low CFI (CFI, 0-2) groups.
Outcome and Definitions
The primary outcome of this study was a composite outcome of the perioperative SAEs during the hospitalization period. The definition of SAEs used in this study was adapted from the International Conference on Harmonization’s definition of Good Clinical Practice. The SAEs that were considered in this study included various types of infections (such as respiratory, urinary, surgical site, and sepsis), delirium (as assessed by the Confusion Assessment Method), thromboembolic complications (including deep vein thrombosis treated with anticoagulation or pulmonary embolism), acute heart failure, acute respiratory failure, malignant arrhythmia, stroke, gastrointestinal bleeding, and acute renal failure and death.
Statistical Analysis
The study employed independent t-tests, ANOVA, or Kruskal-Wallis tests to compare participants’ characteristics across different groups for continuous variables, while the Chi-squared test was used for categorical variables. Effects of the CFI and surgery (Model a) or time-to-surgery (Model b) on SAEs were analyzed by multivariate logistic regression model. Referring to previous cohort study,
18
comorbidities, osteoporosis, fracture type, and polypharmacy were included as covariables. In order to reduce bias, a directed acyclic graph (DAG) diagram was created prior to the study in order to identify possible confounders (Figure 1). At the same time, considering the correlation between CFI and these covariables, we conducted a collinearity test to ensure the reliability of the model. The findings were presented as odds ratios (ORs) accompanied by 95% confidence intervals (CIs). Analyses were performed using SPSS software (version 22.0, IBM Corp, Armonk, NY, USA), with two-sided P < .05 indicating significance. Directed acyclic graph (DAG) for statistical model. The DAG serves as a visual representation of the interconnections within the data, aiding in the elucidation of the study’s underlying assumptions. As a simplification by design, the DAG facilitates comprehension for the reader.
Reaults
Baseline and Perioperative Characteristics
Participants Demographics and Perioperative Characteristics.

Statistics are t-value for t test of normalized continuous variables, M-W for nonparametric variables, or χ2 for test of categorical variables; * The results were statistically significant (P < .05). Abbreviations: CFI, Chart-derived frailty index; ASA, American Society of Anesthesiologists; SAEs, Serious Adverse Events; IQR, Interquartile Range.
Predictive Factors of Perioperative Seious Adverse Events
Incidence of Individual Serious Adverse Events During Hospitalization According to Frailty State and Operation Treatment.

aThe results were statistically significant (P < .05).
Multivariate Logistic Regression Analysis of the Effects of Frailty, Surgical Factors, and Surgical Timing on the Occurrence of Perioperative SAEs During Hospitalization.
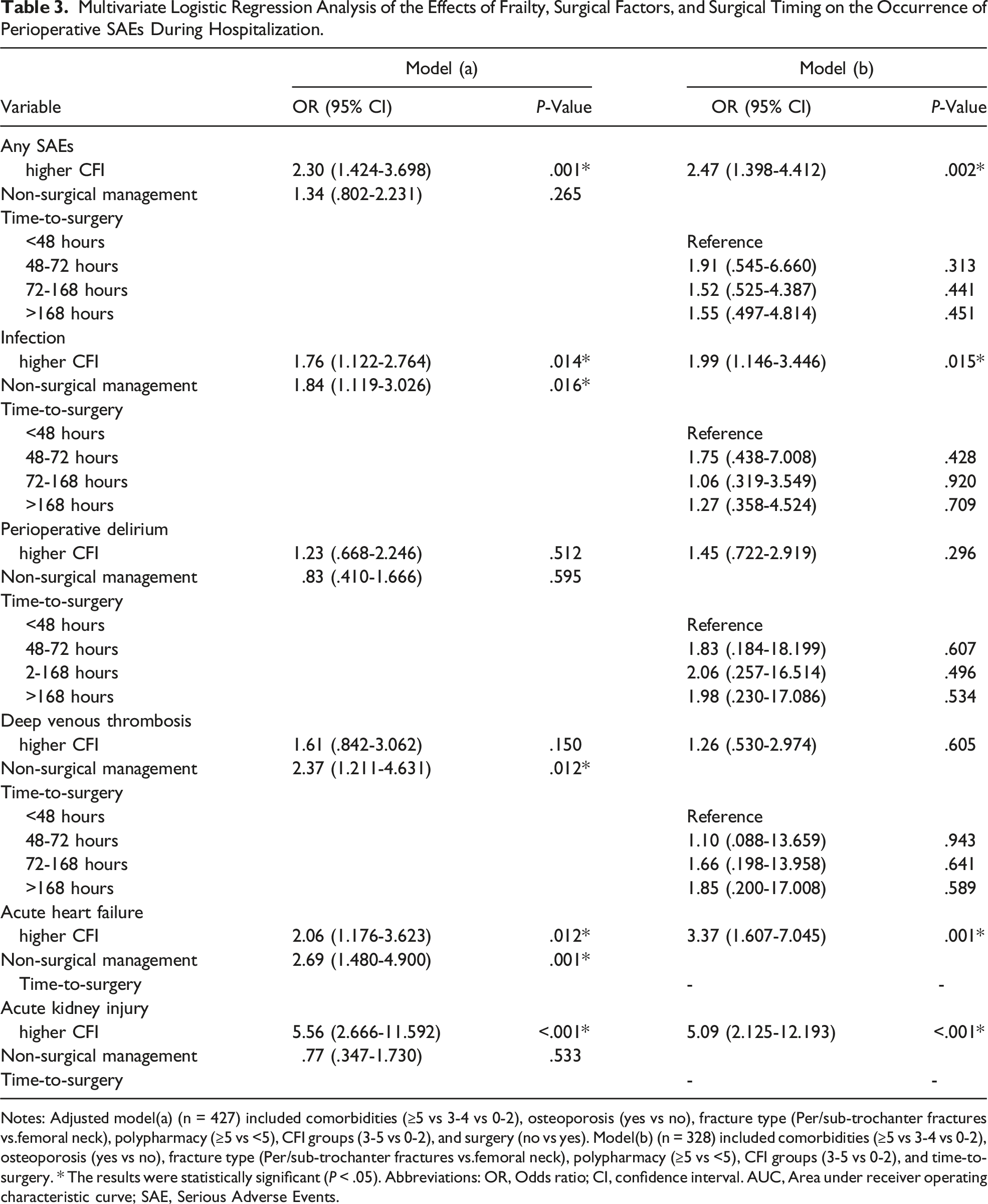
Notes: Adjusted model(a) (n = 427) included comorbidities (≥5 vs 3-4 vs 0-2), osteoporosis (yes vs no), fracture type (Per/sub-trochanter fractures vs.femoral neck), polypharmacy (≥5 vs <5), CFI groups (3-5 vs 0-2), and surgery (no vs yes). Model(b) (n = 328) included comorbidities (≥5 vs 3-4 vs 0-2), osteoporosis (yes vs no), fracture type (Per/sub-trochanter fractures vs.femoral neck), polypharmacy (≥5 vs <5), CFI groups (3-5 vs 0-2), and time-to-surgery. * The results were statistically significant (P < .05). Abbreviations: OR, Odds ratio; CI, confidence interval. AUC, Area under receiver operating characteristic curve; SAE, Serious Adverse Events.
Discussion
In this study, we investigated the relative contributions of frailty and surgical timing to the outcomes of elderly hip fracture patients. Specifically, frailty status was significantly associated with perioperative SAEs during hospitalization, such as infection and acute heart failure. This finding holds implications for enhancing clinical decision-making. It is crucial to minimize surgical delays, however, this study suggests that perioperative risks should be carefully assessed and managed, with particular attention to the patient’s frailty status. This approach may identify specific modifiable factors that warrant intervention.
To assess frailty status, we employed a validated chart-derived frailty score (CFI) and conducted a systematic evaluation among older individuals with hip fractures. A strong correlation was observed between a high frailty index and the occurrence of SAEs, such as infections, acute heart failure, and acute kidney injury. Additionally, the CFI was found to be linked to significant perioperative complications following hip fracture surgery, as reported by Zhao H, et a. 14 This study contributes to the existing understanding of the association between frailty and the prognosis of surgical risks. The predictive significance of frailty in this context is not unexpected, as frail individuals are more susceptible to negative outcomes post-surgery due to their diminished ability to cope with and recover from the procedure. Furthermore, the prevalence of multimorbidity is observed to be higher among frail individuals. 19 Our study findings indicate that patients with a high CFI exhibit a greater incidence of comorbidities, with 27.3% of them experiencing comorbidities compared to 11.4% in the low CFI group (P < .001). This association contributes to elevated rates of unfavorable outcomes in frail individuals. In addition, subgroup analyses reveal that a high CFI is statistically significant solely within subgroups involving surgery and surgery delayed by 72-168 hours. A study has estimated that a considerable proportion (41%) of patients undergoing major orthopedic surgery are at a significantly higher risk of experiencing frailty. 20 Furthermore, a meta-analysis encompassing 45 979 participants has demonstrated that frailty significantly predicts both postoperative and inpatient complications in geriatric hip fracture patients. 12 These results emphasize the importance of considering the substantial risks associated with frailty, regardless of the surgical indication.
In the context of hip fracture surgery for older individuals, the significance of risk stratification and timely identification of vulnerable patients is growing, as it can enhance surgical effectiveness and optimize medical resource allocation. While the ACS recommends preoperative frailty assessment, there is a wide variability among assessment methods and their results. 21 In comparison to other instruments like the Fried phenotype, Edmonton Frail Scale, CSHA-FI, and ACS-NSQIP, the CFI scores can readily identify susceptible patient groups upon admission using routine laboratory results, providing an objective and convenient information source and not requiring any additional effort or cost. For example, Amrock et al. 17 have demonstrated that the CFI is a more effective measure of frailty compared to the Robinson score or the 11-factor modified frailty index. Furthermore, Yu J, et al. 22 have reported that a high CFI is associated with an increased 1-year mortality rate following radical cystectomy in a cohort of 1004 patients with bladder cancer. Additionally, the CFI has been found to enhance the predictive power of the ASA classification in determining the likelihood of delirium, pneumonia, ICU admission, and 1-year mortality after hip fracture surgery. 14 Therefore, the integration of demographic information and routine laboratory variables in the evaluation of CFI has the potential to serve as a proficient and straightforward method for prognosticating outcomes in clinical settings.
It should be noted that, upon accounting for confounding variables, the infuence of surgery timing on SAEs is uncertain and requires further investigation. A potential reason for this conclusion may be that the sample size was not large enough to show the difference. Although early surgery may be linked to reduced suffering, delayed surgery provides ample time for physiological stabilization. The specifics of optimal surgical timing remained ambiguous, despite guidelines recommending surgery within 48 hours. Alvi HM, et al 23 had utilized a nationally representative dataset comprising 6036 elderly individuals who underwent hip fracture surgery, and employing a meticulous statistical approach (including matching for surgery type, age, gender, and ASA class), the authors observed no discernible disparities in 30 day mortality, readmission rate, or overall complication rate across the 3 surgical cohorts (<24 hours, 24-48 hours, and >48 hours). Similar findings also had been demonstrated in older patients with pathological hip fractures 9 and periprosthesis fractures. 10 As previously mentioned, These results are in contrast to other studies about standard hip fractures, which have discovered that patients who undergo early surgical intervention for hip fractures exhibit reduced hospitalization durations, diminished pain duration, lowered susceptibility to decubitus ulcers, and enhanced post-procedural independence.6-8 This phenomenon could potentially be elucidated by various factors, such as disparities in the demographic composition of the sample, sample size, correctional variables, definitions of complication variables, and follow-up periods. Providing care for elderly and fragile hip-fracture patients and minimizing surgical wait times pose challenges for health care providers. Taking into account the frailty status and various other factors in clinical practice, there exists a possibility of moderately modifying the risk of perioperative complications, including the optimization of the time from clinical presentation to surgery. 9 It should be noted that in this population at high risk, merely reducing the waiting time for surgery may not yield significant improvements in outcomes.
Several limitations should be acknowledged in this study. Firstly, the generalizability of the findings may be limited due to the study being conducted in a single center. Conducting multicenter studies could enhance the generalizability of the results. Another limitation is the small number of patients who had surgery within 48 hours, limiting the ability to identify statistically significant differences between groups. In addition, it is important to note that our observations are restricted to adverse outcomes during hospitalization, and therefore, we are unable to make any conclusions regarding long-term effects. Moreover, the outcome variable of SAEs in this study is a composite variable. Due to insufficient data in the research sample, separate analyses for surgery-specific SAEs, such as surgical site infection and postoperative delirium, were not conducted in multivariate logistic regression. However, the existing data have effectively illustrated that the evaluation and intervention of frailty status hold greater significance in enhancing perioperative risk management for elderly patients with fractures, surpassing the sole consideration of surgical timing.
Within the scope of this study, a notable association between frailty and the occurrence of in-hospital SAEs in elderly individuals with hip fractures is evident, while the influence of surgical timing on these outcomes is still unclear. The CFI could be a useful pre-screening tool to identify patients at a high risk of perioperative complications. Future research should focus on defining the optimal components and implementation of precision management for frail patients.
Supplemental Material
Supplemental Material - Risk Factors of Serious Adverse Events for Geriatric Hip Fractures: Is it the Frailty or the Timing?
Supplemental Material for Risk Factors of Serious Adverse Events for Geriatric Hip Fractures: Is it the Frailty or the Timing? by Ling-xiao Wang, Li-juan Guan, Ming-hong Deng, and Li-hua Zhou in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Author Contributions
Ling-xiao Wang, Li-juan Guan, Ming-hong Deng and Li-hua Zhou collected patient data and contributed to the database fill-in process. Ling-xiao Wang performed data analysis and contributed to draft the work. Ling-xiao Wang designed the study and was responsible for data interpretation. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chengdu Science and Technology Bureau (NO.2022-YF09-00014-SN) and the Fifth People’s Hospital affiliated to Chengdu University of Traditional Chinese Medicine (NO. GSPZX2022-01).
Ethical Statement
The study was approved by the Ethics Committee of the Fifth People’s Hospital affiliated to Chengdu University of TCM and conducted in accordance with the 1964 Declaration of Helsinki.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.