
Abstract
Introduction:
Preliminary analysis of accelerometry measurements has shown physical activity may not increase significantly after total knee arthroplasty (TKA). This study evaluates the effect of TKA on physical activity accelerometry measurements and body mass index (BMI).
Methods:
Using the multicenter Osteoarthritis Initiative (OAI) database, a cohort of patients with physical activity level accelerometry measurements and BMI before and after TKA was identified. Physical activity levels and BMI were acquired at pre-TKA and post-TKA accelerometry visits 2 years apart. Survey scores pertaining to knee functionality and quality of life were also analyzed before and after knee surgery. Each patient included in the study had a unilateral TKA completed between these 2 accelerometry visits. Accelerometry measurements, BMI of the patients, and survey scores relating to knee functionality and pain relief from before and after TKA were compared using paired samples t tests.
Results:
Twenty-three patients from the OAI database were identified for the paired analysis. They were evaluated at a mean postoperative follow-up of 15 months. There were no statistically significant differences between the post-TKA group and pre-TKA group for the accelerometry variables and BMI, though patients experienced a significant improvement in knee function and pain relief measures included in this analysis.
Discussion:
Although TKA can successfully restore function and relieve pain, there remains no good evidence that neither physical activity nor BMI improve postoperatively.
Conclusion:
No significant differences in physical activity and BMI were observed after TKA in this study.
Keywords
Introduction
Total knee arthroplasty (TKA) is a successful procedure in improving patient function and quality of life. 1 Much of the existing evidence on the changes in patient physical activity levels after TKA has relied on self-reported outcome scores. 2 -4 However, these patient-reported outcomes, some of which are designed to ascertain information on physical activity levels, have shortcomings in both validity and reproducibility. 3,5 -10 Patients expect to become more active following TKA, and this expectation may be reflected in their self-reported survey results, which have often suggested an increase in physical activity post-TKA. 2,3 Thus, it remains unclear whether patients objectively achieve improvements in physical activity levels after surgery.
One objective method of measuring physical activity is by accelerometry, which is widely considered an accurate means of quantifying physical activity. 11 -13 Accelerometry provides information on various parameters of physical activity including the duration, frequency, and intensity of activity. 13 -15 Prior analysis of accelerometry measurements has shown that patient physical activity may not improve significantly after TKA. 5 -7,16 Moreover, some studies have shown that only a small subset of patients meets the activity levels recommended by the American Physical Activity Guidelines following TKA. 5 -7,16 Patients’ inability to improve physical activity levels post-TKA may reflect limited improvements in ambulatory function, as well as hamper any improvements in body mass index (BMI), which can be a predictor of significant morbidity and mortality when elevated. 17,18
While there is a plethora of patient-reported outcome studies on subjective changes in activity levels post-TKA, accelerometry studies evaluating physical activity have only recently emerged, and the conclusions are unclear. 3,5 -7,9,10 The purpose of this study is to evaluate the effect of TKA on different physical activity accelerometry measurements and BMI. Our hypothesis is that there is no significant difference between the pre- and post-operative activity levels and BMI in TKA patients.
Methods
Study Design and Population
The multicenter Osteoarthritis Initiative (OAI) database was used for analysis in this study. 19 The OAI database included 4796 patients who had clinically significant osteoarthritis were at high risk for developing clinically significant osteoarthritis, or had no risk factors for osteoarthritis. Risk factors considered for subject inclusion in the OAI study were older than 70 years, history of knee injury causing difficulty walking for over 1 week, history of knee surgery, and elevated weight with varying minimum weight cutoffs based on age and gender. The presence of knee osteoarthritis in potential patients was assessed using radiographic evidence of tibiofemoral osteophytes as well as reported pain, aching, and stiffness. Patients who consented to participate in an OAI accelerometry substudy were instructed to wear the accelerometer from morning until night, for 7 consecutive days, only taking it off for water-involving activities. Two accelerometry visits took place at 4 and 6 years from baseline OAI visit, for which patient enrollment began in 2004.
All of the patients from the OAI database who were retrospectively identified and included in this study had elevated risk for developing clinically significant disease or clinically significant osteoarthritis at their baseline OAI visit. The patients included in this study all underwent unilateral TKA between their first OAI accelerometry visit (pre-TKA visit) and second OAI accelerometry visit (post-TKA visit). These visits were 2 years apart, with the post-TKA visit taking place at least 3 months after surgery. The study design is shown in Figure 1.
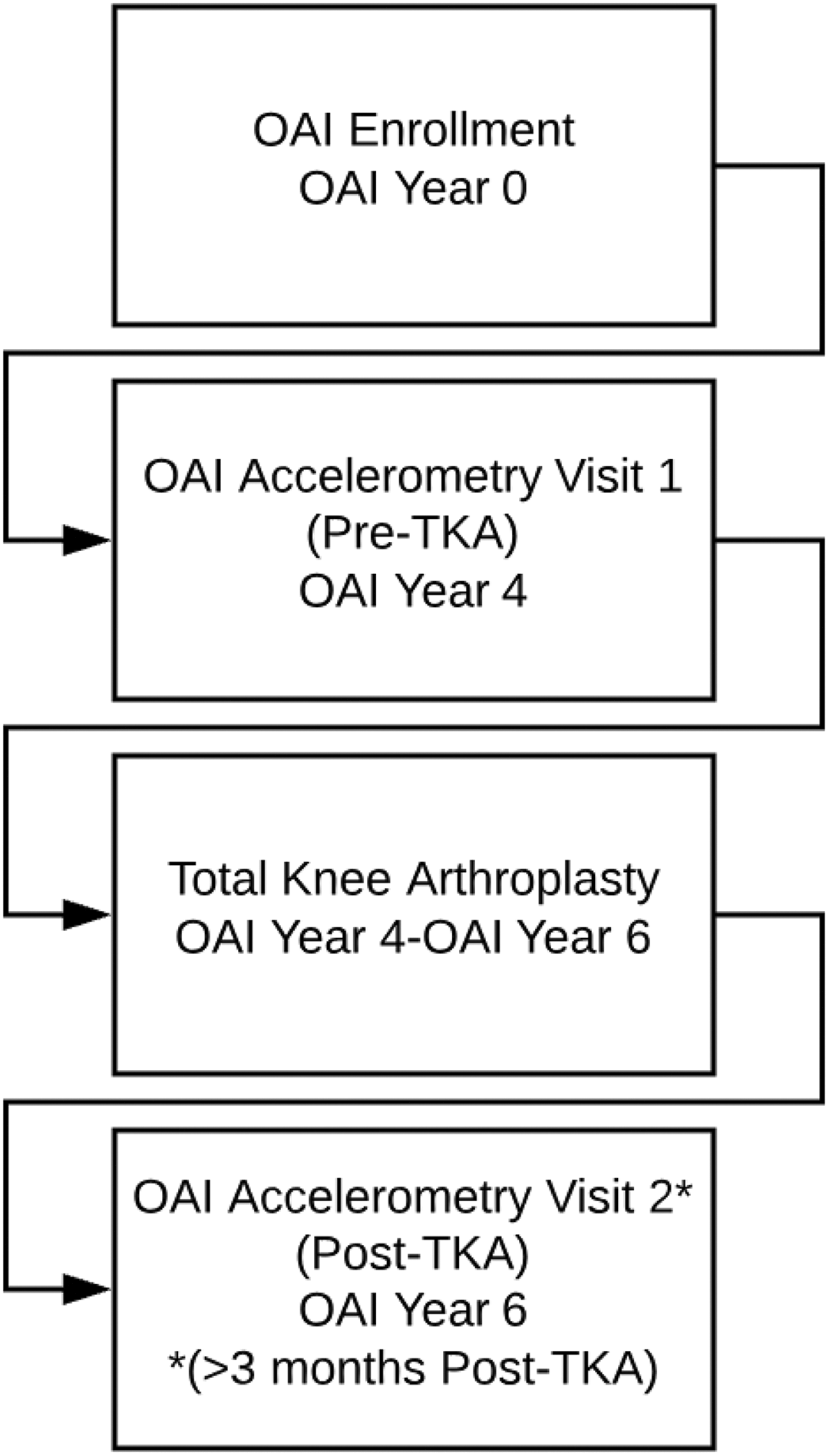
Study design. Patients were enrolled in the OAI study (OAI year 0). Four years later, they completed their first accelerometry visit, the preTKA visit. They had TKA between their first and second OAI visits, anytime from OAI year 4 to OAI year 6. Six years after OAI enrollment, patients had their second accelerometry visit, the post-TKA visit. Patients included in this study had their post-TKA visit at least 3 months after TKA. OAI indicates Osteoarthritis Initiative; TKA, total knee arthroplasty.
Independent Variables
Age, gender, race, employment, BMI, time before or after TKA, Charlson Comorbidity Index Score, 20 history of heart failure, history of stroke, and history of lung disease were also available and compared between the 2 accelerometry visits. The accelerometer worn by patients recorded activity counts, a weighted sum of the number of accelerations measured per minute in which a higher measured acceleration resulted in a higher count. Accelerometry data were categorized using cut points published by Troiano et al. 21 These cut points divided activity counts into different physical activity levels such as light activity, moderate activity, and vigorous activity. Survey scores related to difficulty walking, pain while walking, modification of quality of life to avoid potentially damaging knees, Western Ontario and McMaster osteoarthritis index (WOMAC) disability score, and WOMAC pain score were also evaluated.
Statistical Analysis
Analysis was completed for the primary paired analysis cohort comprised of patients whose activity levels and BMI were documented in their post-TKA accelerometry visit at least 3 months after surgery. This analysis was repeated for a subcohort of patients who had their post-TKA accelerometry visit at least 6 months after surgery. All analysis was completed using Statistical Packaging Software (Version 22; SPSS Inc, Armonk, New York). Categorical patient demographics before and after surgery were compared using McNemar test. Accelerometry measurements, BMI, and survey scores of the post-TKA cohort were compared to those of the pre-TKA cohort using paired samples t tests. An α of .05 was determined to be the P value of statistical significance.
Results
The paired analysis cohort studied was comprised of the same 23 patients at 2 OAI accelerometry visits that collected accelerometry data, BMI, and survey scores. These patients had TKA at least 3 months before their post-TKA accelerometry visit. At study onset, the average patient age was 66.2 years (standard deviation [SD]: 8.9). The average patient BMI was 28.9 (SD 4.3). The patient cohort studied was 52.2% male. The patients in this cohort had post-TKA accelerometry measures of activity levels gathered 457.4 days (SD: 209.7) postoperatively on average. The rest of the patient demographics at enrollment can be found in Table 1. There were no significant differences in patient demographics between the pre-TKA accelerometry visit and the post-TKA accelerometry visit (Table 2).
Post-TKA Visit ≥3 Months After TKA: Patient Demographics at Enrollment in Study.

Abbreviations: BMI, body mass index; TKA, total knee arthroplasty.
Post-TKA Visit ≥3 Months After TKA: Patient Demographics at Accelerometry Visit 1 (Pre-TKA), 4 Years After Enrollment, and at Accelerometry Visit 2 (Post-TKA), 6 Years After Enrollment in Study.

Abbreviation: TKA, total knee arthroplasty.
The cohort of patients at least 3 months from surgery (15.0 months postoperative on average; SD 6.9 months) at post-TKA accelerometry demonstrated no significant difference between physical activity and BMI after TKA. Pre-TKA patients had a 20 meter walk pace of 1.19 meters per second (m/sec; SD: 0.15), while the post-TKA patients had a walk pace of 1.17 m/sec (SD: 0.18) with no significant difference between the 2 groups (P = .670). The mean daily activity count was 156 151.1 counts per day (SD: 89148.0) for the pre-TKA group and 150 482.5 counts per day (SD: 108291.7) for the post-TKA group (P = .628). There were no significant differences between the patients before and after TKA for daily minutes of light activity (238.9 [SD: 70.3] vs 231.7 [SD: 85.4]), daily minutes of moderate activity (11.0 [SD: 13.4] vs 9.9 [SD: 14.2]), daily minutes of vigorous activity (0.00 [SD: 0.00] vs 0.07 [SD: 0.07]), daily bout minutes of moderate-vigorous activity (5.2 [SD: 7.8] vs 4.6 [SD: 10.0]), and daily bout minutes of vigorous activity (0.00 [SD: 0.00] vs 0.00 [SD: 0.00]). Average BMI in the patient cohort was 29.2 (SD: 4.8) before TKA and 28.8 (SD: 4.9) after TKA (P = .282). Additional information about this group can be found in Table 3. Survey scores demonstrated statistically significant improvements in difficulty walking (1.4 [SD: 1.4] vs 0.35 [SD:0.65]), pain while walking (1.9 [SD: 1.3] vs 0.48 [SD: 0.79]), modification of quality of life to avoid potentially damaging knees (1.7 [1.0] vs 1.0 [0.9]), WOMAC disability (32.1 [SD: 21.6] vs 11.0 [SD: 13.2]), and WOMAC pain (9.7 [SD: 6.4] vs 2.8 [SD: 3.8]; Table 4).
Post-TKA Visit ≥3 Months After TKA: Tracking Change in Physical Activity and BMI from Before TKA to After TKA.
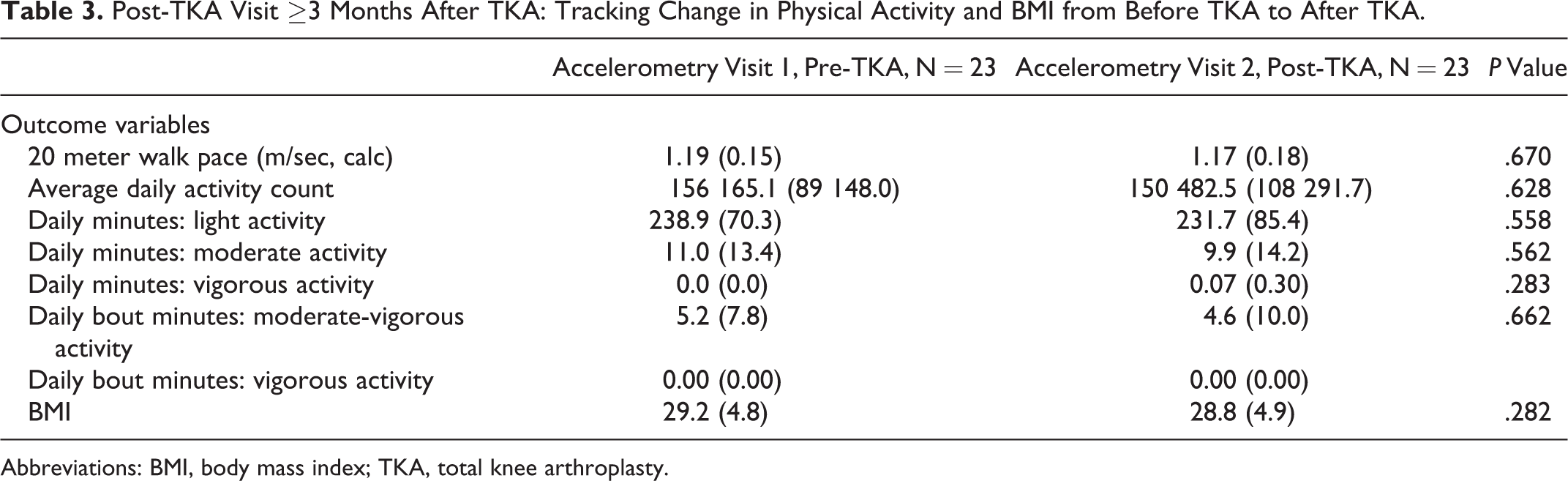
Abbreviations: BMI, body mass index; TKA, total knee arthroplasty.
Post-TKA Visit ≥3 Months After TKA: Tracking Change in Survey Scores Before and After TKA.

Abbreviations: TKA, total knee arthroplasty; WOMAC, Western Ontario and McMaster osteoarthritis index.
A subcohort of 18 patients who had TKA at least 6 months before their post-TKA accelerometry visit was also studied. These patients had TKA an average of 17.9 months (SD: 4.7 months) before post-TKA accelerometry measurements. This subcohort’s enrollment data can be found in Table 5. There were no significant changes in this subcohort’s demographics from the pre-TKA accelerometry visit to the post-TKA accelerometry visit (Table 6). Mirroring the larger cohort’s results, there were no significant changes in this subcohort’s physical activity levels and BMI after TKA (Table 7). Survey scores demonstrated statistically significant improvement in every parameter assessed (Table 8). In summary, the patients included in this study experienced no significant differences after TKA in physical activity accelerometer measurements and BMI, while subjective knee functionality and pain relief improved significantly after knee surgery.
Post-TKA Visit ≥6 Months After TKA: Patient Demographics at Enrollment in Study.

Abbreviations: BMI, body mass index; TKA, total knee arthroplasty.
Post-TKA Visit ≥6 Months After TKA: Patient Demographics at Accelerometry Visit 1 (Pre-TKA), 4 Years After Enrollment, and at Accelerometry Visit 2 (Post-TKA), 6 Years After Enrollment in Study.

Abbreviation: TKA, total knee arthroplasty.
Post-TKA Visit ≥6 Months After TKA: Tracking Change in Physical Activity and BMI From Before TKA to After TKA.
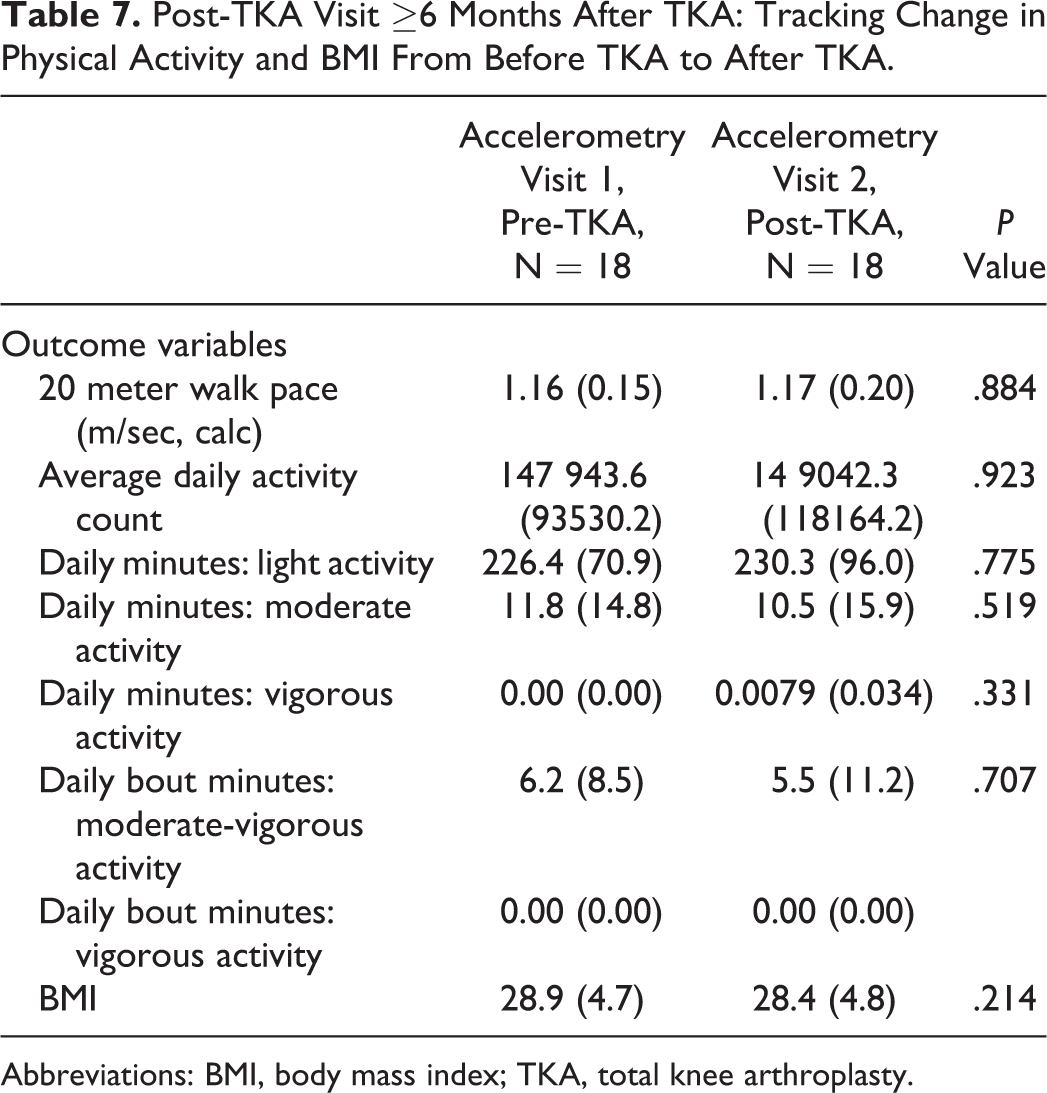
Abbreviations: BMI, body mass index; TKA, total knee arthroplasty.
Post-TKA Visit ≥6 Months After TKA: Tracking Change in Survey Scores Before and After TKA.

Abbreviations: TKA, total knee arthroplasty; WOMAC, Western Ontario and McMaster osteoarthritis index.
Discussion
Despite patient self-reported improvements in pain and function from pre- to post-TKA in the literature, 2,3,8 surgery did not improve accelerometry-measured activity levels postoperatively in this study. The results of our analysis confirm our hypothesis that there is no difference in activity levels or BMI when comparing pre-TKA patients to those post-TKA.
The findings of this study are consistent with a number of others that evaluated activity levels using accelerometry. 5 -8,16 Moreover, even some self-reported survey studies suggest patient activity decreases post-TKA 22 or show mixed results regarding the effect of TKA on patient activity. 23
Because accelerometry was only recently incorporated in research evaluating TKA, there are fewer studies evaluating physical activity using this method than there are survey studies. Additionally, of the accelerometry studies that do exist, only some are paired accelerometry studies using the same patients pre-and post-TKA. This study contributes to the growing body of research conducted on paired patients to measure activity level before and after TKA. Body mass index was also incorporated into this analysis because of its association with physical activity in the literature and its clinical relevance as a risk factor for disease. 18,24,25 Previous studies have shown that patients undergoing TKA do not experience a significant change in BMI. 26 -29 Our study also found no significant change in BMI before and after TKA. This finding, in addition with previous studies, suggests that the improvements in knee function and pain that can result from TKA may not translate to any significant weight loss in patients.
The authors of this article acknowledge that there are previous studies using the OAI database to evaluate physical activity or BMI changes after TKA; however, these studies did not use paired cohorts of OAI patients before and after TKA. 5,6,30 There was also a systematic review of physical activity levels pre- and post-TKA completed in 2015. 31 This systematic review, being comprised of mostly survey studies on physical activity, called for further study of the relationship between TKA and accelerometry-measured activity levels. Our study contributes to the relatively limited evidence in existing literature that TKA may not have an effect on accelerometry-measured physical activity levels.
Our results, showing neither physical activity nor BMI change postoperatively, prompt further investigation into the interplay between physical activity and BMI. A better understanding of the relationship between these 2 variables could inform comprehensive lifestyle modifications in patients who would allow them to better take advantage of their improved mobility post-TKA as well as help educate patients as to what to expect after TKA and thus improve satisfaction after TKA.
In fact, a recent study showed that BMI and physical activity are the 2 most important predictors of post-TKA outcomes as measured by the Knee injury and Osteoarthritis Outcome Score. 32 The study concluded that patient goals postoperatively should be benchmarked against their preoperative lifestyles, and customized goals for each patient could drive increases in physical activity and superior outcomes postoperatively. Previous studies using the OAI database have shown that the majority of patients in the pre-TKA and post-TKA groups do not meet the Department of Health and Human Services guidelines for physical activity, 5 -7 even when the guidelines are adjusted for arthritis as a comorbidity. These findings suggest that these guidelines may represent unrealistic expectations for patients before and after TKA. Another possibility is that patients may be able to meet these current guidelines with modifications in physical therapy regimens and goals after surgery. While there are studies showing significant differences between pre-TKA and post-TKA group activity levels as measured by accelerometry, 17 they were limited by the shorter length of accelerometry recording periods. The differences in these patients’ increased activity levels post-TKA may largely be attributed to physical rehabilitation practices postoperatively. 33,34
Numerous accelerometry studies 5 -8,16 demonstrating that physical activity may not significantly change post-TKA could call into question the importance of change in physical activity level as a measure of success post-TKA when compared to other parameters such as improvements in pain and patient quality of life. 35 In this study, we confirmed a dramatic improvement in subjective measures evaluating knee functionality and pain after TKA, which is likely more pertinent to postoperative satisfaction than objective physical activity alone.
The primary limitation of this study is that patients within the paired analysis cohort received their TKAs at different time points within the 2-year span between the accelerometry visits. Patients who received TKA less than 3 months before their post-TKA accelerometry visit were excluded in the larger cohort, with patients in this group being 15 months postoperative on average at the time of accelerometry collection. The subcohort of patients who were at least 6 months post-TKA at their post-TKA accelerometry visit were about 18 months postoperative on average at the time of accelerometry collection. Earlier studies recording self-reported physical activity changes and pedometry before and after TKA have reported changes in activity levels as soon as 3 months post-TKA, which prompted the inclusion of the 3-month lower limit of time between TKA and the post-TKA accelerometry revisit in this study. 36,37 Another study had showed a small statistically significant increase in patient activity levels at 6 months postoperatively, 25 with other similarly designed studies published in the last few years showing no significant difference in patient physical activity as measured by accelerometry when patients are at least 6 months post-TKA. 7,16 Acknowledging this discrepancy, the authors of this study chose to analyze the subcohort of patients in this study who had surgery at least 6 months prior to post-TKA accelerometry measures of activity level.
Another limitation of this study was the small sample size of patients in the paired cohort. Although thousands of patients were enrolled in the OAI study, only a fraction of these patients received TKAs between the 2 accelerometry visits. The authors of this article chose to conduct a paired analysis, despite the smaller sample size in this study, to limit demographic differences between the pre- and post-TKA groups.
Conclusion
Analysis of physical activity as measured by accelerometry and BMI showed no significant difference between postoperative patients and preoperative patients. Although TKA is widely successful in restoring function and relieving pain and disability from knee osteoarthritis, there remains no good evidence that patient daily physical activity measured by accelerometry or BMI improve postoperatively.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.