
Abstract
Background:
Despite the alleviation of osteoarthritis (OA) symptoms that total knee arthroplasty (TKA) provides for patients with end-stage knee OA, recent studies have suggested that TKA may not increase physical activity levels. In this study, we compare the physical activity levels of patients with OA treated nonoperatively (non-TKA) with both patients who had received TKA (post-TKA) and patients who received TKA within 3 years of data collection (pre-TKA).
Methods:
Utilizing the Osteoarthritis Initiative database, accelerometry data were collected from non-TKA, pre-TKA, and post-TKA patients. Accelerometry data were subdivided by physical activity intensity levels, yielding daily minutes of each level of activity. Physical activity levels were then compared between non-TKA and pre-TKA/post-TKA patients. Physical activity levels for each patient were also compared to the Department of Health and Human Services (DHHS) guidelines for physical activity.
Results:
There was no difference in physical activity between non-TKA and pre-TKA patients, with the exception of non-TKA patients achieving more daily minutes of vigorous activity (P < .001). There was no difference in physical activity between non-TKA and post-TKA patients. Although 11.6% of non-TKA patients met DHHS guidelines, only 4.8% of pre-TKA and 5.3% of post-TKA patients met guidelines.
Conclusion:
Despite the improvements in patient-reported outcome measures following TKA, we found that TKA alone does not improve physical activity levels beyond those seen in the average patient with OA. In our study, the vast majority of patients with OA, treated nonoperatively or operatively, did not meet current DHHS guidelines for physical activity.
Introduction
Total knee arthroplasty (TKA) is associated with increased patient-reported function, decreased pain, and improved quality of life 1 –6 for patients with end-stage osteoarthritis (OA) of the knee. It is also considered to be a cost-effective treatment when considering life-years gained. 6 –12
However, despite the aforementioned benefits of TKA, its effects on physical activity levels are a matter of debate. There are conflicting results in the literature regarding the relationship between TKA and physical activity levels, 13 –17 though more recent studies indicate that physical activity levels may not increase following TKA. 13–14 A previous study by Kahn and Schwarzkopf demonstrated that there was no difference in objective physical activity levels between patients who would soon receive a TKA and those who had already received a TKA. 14 The implications of these findings are important as an outcome and public health issue. 18 –20 Patients tend to associate increased physical activity following TKA with a good overall outcome, 21 while several randomized, controlled trials have also demonstrated the numerous benefits of exercise for patients with OA, including increased objective function and decreased pain and stiffness. 22,23 Furthermore, patients who continue to achieve poor levels of physical activity are at increased risk of cardiovascular comorbidities known to be associated with a sedentary lifestyle. 24,25
One of the difficulties in measuring physical activity levels in patients is the unreliability of patient-reported activity levels. 13,17,26 One solution to this problem has been found with the use of accelerometers to objectively measure physical activity levels. The accelerometer measures vertical acceleration and deceleration of the patient, yielding data regarding the intensity, duration, and frequency of physical activity in the patient. 27 –29
Complicating the process of utilizing the physical activity data in TKA patients is the difficulty in deciding what levels of physical activity are optimal for these patients. There is currently little consensus on what level of activity should be achieved or what levels are even realistic for patients. Although the obvious comparison of preoperative patient activity levels to postoperative activity levels has been accomplished in several studies, 13 –15,17 no studies thus far have evaluated the activity levels of TKA patients in comparison to other patients with OA who do not receive TKA.
In this study, we utilize accelerometry data to compare the physical activity levels of both pre-TKA and post-TKA patients to patients with OA who have not received TKA. Secondary objectives of this study include comparing patient-reported outcomes, including pain, function, and quality of life scores, between TKA patients and non-TKA patients with OA. Our hypothesis is that while patient-reported outcomes in post-TKA patients may be equivalent or better than non-TKA patients, both pre-TKA and post-TKA physical activity levels will be significantly less than those of non-TKA patients with OA.
Methods
All data were obtained from the Osteoarthritis Initiative (OAI), a multicenter, prospective cohort study of patients with or at risk for OA. 30 At the beginning of the OAI study, the 4796 participating patients were divided into a progression subcohort (1389 patients), which represented patients who already had clinically significant OA, an incidence subcohort (3285 patients), which represented patients at high risk of developing clinically significant OA, and a control cohort (122 patients). Each patient was required to attend a baseline visit as well as subsequent annual visits over the course of the study, where clinical, radiological, and biomarker data were obtained. Currently, annual visits have been performed with publically released data up through an 84-month visit. All data, including radiographic images and biomarkers, can be obtained at http://www.oai.ucsf.edu.
At the 48-month visit of the OAI study, 2712 patients were invited to participate in an ancillary study of physical activity utilizing an accelerometer; 2127 patients consented and participated in this portion of the study. Patients were instructed to wear an ActiGraph GT1M uniaxial accelerometer (ActiGraph; Pensacola, Florida) for 7 consecutive days. Participating patients were instructed by trained OAI staff on how to wear and use the accelerometer; patients were to wear the accelerometer from waking in the morning to retiring at night. The accelerometer was only to be removed during water activities. Patients were also instructed to maintain a daily log of either water activity or cycling, as both of these activities are not accurately measured by the accelerometer. Upon return of the accelerometer to the respective study center, the data were analyzed for days of valid data collection—a valid day consisted of greater than 10 hours of recorded wear time. Of the 2127 participants, 2001 patients had 1 or more valid days of recording, and 1927 patients had 4 to 7 valid days recorded.
In our study, we divided the 1927 patients with 4 or more valid days of data into a pre-TKA group, a post-TKA group, and a non-TKA group. The pre-TKA group consisted of patients who underwent TKA between the 48-month visit where accelerometry data were recorded and the 84-month visit (the last OAI visit publically released thus far). The post-TKA group consisted of patients who underwent TKA between the initial baseline visit (0-month visit) and the 48-month visit—consequently, these patients had already undergone TKA (unilateral or bilateral) by the time of the accelerometry data collection. For both the pre-TKA and the post-TKA group, patients were only included if they had an adjudicated TKA (either unilateral or bilateral) and had at least 4 valid days of accelerometry data. The inclusion criteria for valid days were based on previous studies demonstrating that at least 3 to 5 days of wear time is necessary to accurately predict overall physical activity of the patient. 29 Any patient with partial knee arthroplasty was excluded from both the pre-TKA and post-TKA groups. The non-TKA OA group consisted of patients from the progression subcohort of the OAI study who had at least 4 days of valid accelerometry data and did not have any partial or TKA procedures performed during the course of the OAI study (up to 84 months). As the non-TKA OA group only included patients from the progression subcohort of the OAI study, all non-TKA patients with OA were found at the baseline OAI visit to have both frequent knee symptoms, defined as “pain, aching, or stiffness in or around the knee on most days,” for at least 1 month of the past 12 months, and radiographic tibiofemoral knee OA, which was defined by the presence of tibiofemoral osteophytes on the fixed flexion radiograph (Osteoarthritis Research Society International grades 1-3). 30
All accelerometry data were analyzed using cut points, which are a means of dividing activity counts (units of accelerometry data that integrate accelerations and decelerations) over time into categories of physical activity intensity. Previous established cut points in the literature have been designed to correlate physical activity levels with energy expenditure, with light activity corresponding to 1.5 to <3 metabolic equivalents (METs), moderate activity to 3 to 6 METs, and vigorous activity to >6 METs. 31 –33 In this study, we utilize cut points established by Troiano et al, which were previously utilized to study the general adult population in the National Health and Nutrition Examination Study. 31 Using these cut points, the accelerometry data are presented as minutes above a certain physical activity threshold.
Each patient’s accelerometry data were compared to the 2008 Physical Activity Guidelines published by the Department of Health and Human Services, which recommends 150 bout minutes of moderate-intensity exercise (minutes must be accumulated in 10-minute bouts) and 75 bout minutes of vigorous exercise each week. 25 Accelerometry data were also compared to 2008 DHHS guidelines for adults with arthritis, which recommends 150 bout minutes of moderate to vigorous exercise weekly. 25
To compare patient-reported outcome measures between the non-TKA and the pre- or post-TKA groups, the Western Ontario and McMaster Osteoarthritis Index (WOMAC) scores at the 48-month visit (the time of accelerometry data collection) were compared across the groups. As WOMAC scores pertain only to one knee, the scores from bilateral knees were averaged in order to give greater correspondence to physical activity levels.
Statistics were performed using SPSS software (version 22; SPSS Inc, Chicago, Illinois). In comparing the accelerometry data between the non-TKA group and the pre-TKA or post-TKA group, an independent samples t test was performed with a Levene test to assess for equal variances in the patient groups. To compare percentages of patients meeting the 2008 DHHS guidelines, a Pearson χ2 test was performed for each comparison.
Results
Baseline Characteristics
Patients in the pre-TKA and post-TKA groups were significantly older than the patients in the non-TKA OA group (P < .001; P = .009, respectively; Table 1). The average body mass index (BMI) was significantly higher in the post-TKA group compared to the non-TKA OA group (post-TKA: BMI = 31.1, standard deviation [SD] = 5.3; non-TKA: BMI = 29.4, SD = 4.8; P = .012; Table 1). More patients were currently employed in the non-TKA OA group compared to the pre- and post-TKA groups (P = .029; P = .039, respectively). Further baseline characteristics are presented in Table 1.
Baseline Characteristics of Patients.
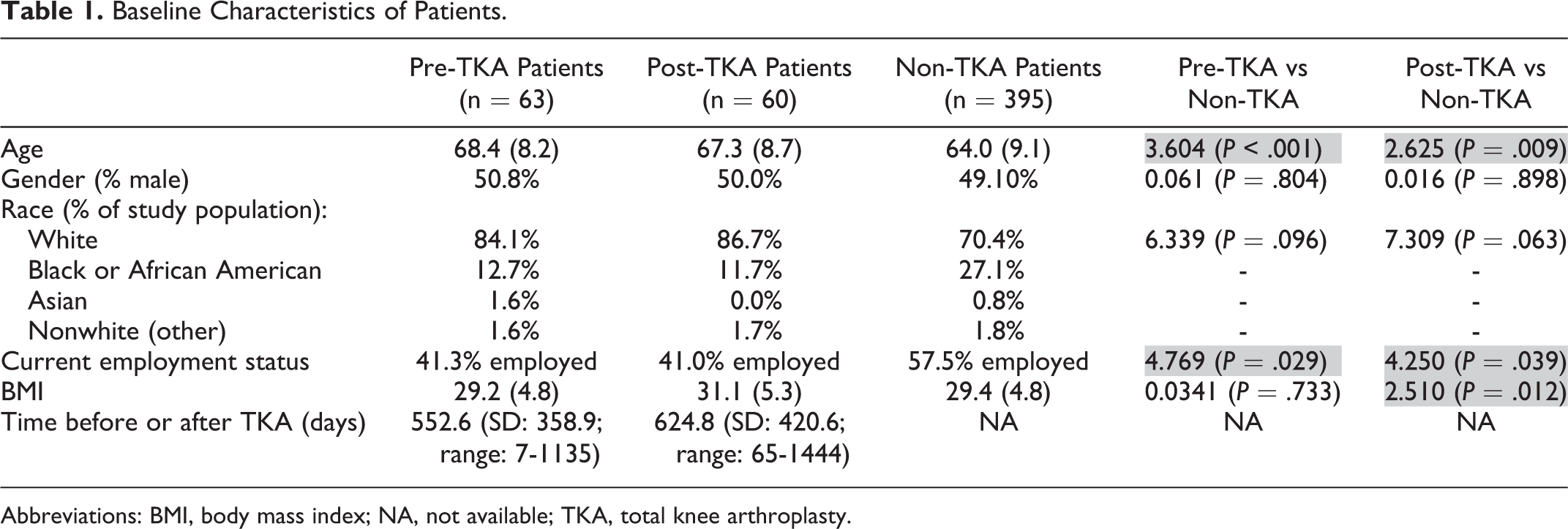
Abbreviations: BMI, body mass index; NA, not available; TKA, total knee arthroplasty.
The average time between accelerometry data collection and TKA in the pre-TKA group was 552.6 days (SD: ±358.9). The average time following TKA that accelerometry data were collected in the post-TKA group was 624.8 days (SD: ±420.6).
Accelerometry Data
In comparing the accelerometry data between pre-TKA and non-TKA patients with OA, the non-TKA patients with OA had significantly higher average daily minutes (as well as bout minutes) of vigorous activity (0.72 vs 0.07 minutes, P < .001). There was no significant difference in average daily activity count (186,878.75 vs 214,461.09, P = .06), average daily minutes of light activity, average daily minutes of moderate activity, or average daily minutes of moderate-to-vigorous activity (Table 2).
Comparison of Accelerometry Data Between Pre-TKA Patients and Non-TKA OA Patients.

Abbreviations: OA, osteoarthritis; TKA, total knee arthroplasty.
Comparing the accelerometry data between post-TKA and non-TKA patients with OA, there was no significant difference in the average daily count between the two groups (197 376.85 vs 214 461.09, P = .26). There was also no difference in average daily minutes of light activity, moderate activity, moderate-to-vigorous activity, or vigorous activity (Table 3).
Comparison of Accelerometry Data Between Post-TKA and Non-TKA Patients.

Abbreviation: TKA, total knee arthroplasty.
Department of Health and Human Services Guidelines
In the pre-TKA group, 4.8% of patients were meeting DHHS guidelines for physical activity (or guidelines for individuals with arthritis) based on accelerometry data. In the post-TKA group, 5.3% of patients were meeting general DHHS guidelines (these same patients also met DHHS guidelines specific for those with arthritis). In the non-TKA group, 11.6% of patients were meeting DHHS guidelines and 11.1% were meeting guidelines specific for arthritis patients. There was no significant difference between pre-TKA and non-TKA or post-TKA and non-TKA patients in regard to the percentage of patients who were meeting the general DHHS guidelines or the DHHS guidelines for patients with arthritis (Table 4).
Comparison of WOMAC Scores between Pre-TKA and Post-TKA Versus Non-TKA OA Patients.

Abbreviations: TKA, total knee arthroplasty; WOMAC, Western Ontario and McMaster Osteoarthritis Index.
Patient-Reported Outcome Measures
The average WOMAC total score in the pre-TKA group was significantly higher (more symptomatic) than the non-TKA group (20.8 vs 15.9, P = .019). Likewise, the WOMAC disability and pain scores in the pre-TKA group were significantly higher than those of the non-TKA group (Table 5). There were no significant differences in WOMAC scores between the post-TKA and non-TKA groups.
Percentages of Patients Meeting DHHS Guidelines.

Abbreviations: DHHS, Department of Health and Human Services; TKA, total knee arthroplasty.
Discussion
Although the overall average daily counts of physical activity were not significantly different between pre-TKA and non-TKA patients with OA, pre-TKA patients achieved significantly less minutes of high-intensity activity/exercise (avg. minutes or bout minutes of vigorous activity) when compared to other patients with OA. This finding is to be expected given that TKA is usually reserved for patients with severe, end-stage OA of the knee.
There was no significant difference between the post-TKA group and the non-TKA OA group in any of the measures of physical activity, whether in total activity counts or even just the more vigorous activity. This indicates that the patients with OA and the post-TKA patients in the OAI study had similar levels of overall physical activity. However, it should be noted that very few patients in either the post-TKA or the non-TKA OA group achieved the recommended level of physical activity according to DHHS guidelines (Table 4).
In our previous study using this same population of pre-TKA and post-TKA patients, we demonstrated that there was no significant difference in physical activity levels (as measured by accelerometry) between the pre-TKA and post-TKA patients. 14 In this study, although no direct comparisons are made between the pre-TKA and the post-TKA groups, we found that the comparison of each group to the non-TKA OA group yielded different results. The reason for this finding is that although the pre-TKA and post-TKA groups were not significantly different from each other in terms of accelerometry data, there was enough difference in accelerometry data to yield variable results when compared to the non-TKA OA group.
Several studies have sought to measure the objective physical activity levels in patients with OA. 34,35,36 Using accelerometry data from the OAI study, Dunlop et al studied patients with radiographic knee OA at baseline and found that only 12.9% of men and 7.7% of women were meeting the 2008 DHHS guidelines for physical activity in adults with arthritis. 34 Furthermore, they found that 40.1% of men and 56.5% of women in the study population were inactive, having done no moderate-to-vigorous activity that lasted at least 10 minutes over the course of a single week. 34 Another study by Holsgaard-Larsen et al compared physical activity levels in patients with OA compared to a control population—they found that while patients with OA did not expend less energy than the control population, patients with OA did walk 29% fewer steps daily. 35 These findings demonstrate significantly less physical activity levels in patients with OA than previously estimated with patient-reported physical activity outcome measures 37 —this is likely due to the overestimation that commonly accompanies self-reported activity levels. 36 Although our study does not compare patients with OA to healthy controls, it can be reasonably inferred from the literature that patients with OA generally perform less physical activity than adults without arthritis. 35,38 In our study, we demonstrate that those patients who are either awaiting TKA or have already undergone TKA continue to demonstrate similar physical activity levels to other patients with OA, contrary to general belief that patients after TKA will have an increased activity level.
There are several limitations to this study. First, as the accelerometry data were collected at a specific visit during the OAI study regardless of the timing of TKA for patients, the timing before or after TKA is highly variable in the pre-TKA and post-TKA groups. Although this would likely affect the physical activity data (those patients closest to TKA would likely be less active), the overall effect is minimal as the average time before or after TKA at the time of accelerometry data collection was over 1.5 years for both the pre-TKA and post-TKA groups. Second, as the non-TKA group represents a large cohort of patients with varying severities of knee OA, it might decrease the statistical power of the study in comparing pre- and post-TKA patients to this group. Third, as some of the non-TKA patients may receive a TKA after the last recorded OAI visit (84-month visit), the distinction between pre-TKA patients and non-TKA patients is somewhat blurred. However, at least in terms of patient-reported outcome measures, these two patient groups proved to be significantly different from each other overall (total WOMAC scores were significantly higher/more symptomatic in the pre-TKA group). Fourth, as the pre-TKA and post-TKA patients were significantly older (averaged about 3-4 years) than the non-TKA patients, this could plausibly serve as a confounding factor that could counteract the potential benefits in physical activity of TKA. Likewise, as less patients were employed in the pre- and post-TKA groups compared to the non-TKA OA group, this could affect physical activity levels as well. Finally, as the OAI study does not collect information regarding the specific implant or technique used for TKA, our results only pertain to the general effects of TKA.
Conclusion
Although pre-TKA patients achieve less vigorous activity levels than non-TKA patients, there is no significant difference in physical activity levels between post-TKA and non-TKA patients with OA. Very few patients in the pre-TKA, post-TKA, or non-TKA patient groups with OA achieve the physical activity levels recommended by the DHHS. Therefore, although TKA provides patients with significant improvements in pain and quality of life, TKA alone does not help patients improve physical activity levels beyond those of the average patient with OA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Consultant for Smith&Nephew, Intellijoint.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.