
Abstract
We investigate whether applying an internal radiocarpal-spanning plate with the wrist in slight extension affects the biomechanical stability of the construct. An unstable distal radius fracture was simulated in 10 cadaveric specimens and immobilized with a radiocarpal-spanning plate holding the wrist in a neutral position. This construct was then physiologically loaded through the wrist flexor and extensor tendons. The resulting motion at the fracture was captured with a displacement sensor. The plate was then extended using an in situ bending technique, placing the wrist in extension, and the experiment was repeated. No statistically significant difference in the biomechanical stability afforded by the radiocarpal-spanning plate was detected with the wrist in extension compared to that in the traditional neutral position. The radiocarpal-spanning plate fixation was more stable when loaded through the extensor tendons. We conclude that immobilizing a distal radius fracture with an internal radiocarpal-spanning plate that holds the wrist in extension does not compromise biomechanical stability.
Introduction
Fractures of the distal radius are common injuries and account for roughly 1 of 6 of all fractures. 1 Prior to the mid-1900s, most distal radius fractures, independent of fracture type, were treated without surgery. 2 Since that time, there has been considerable progress in the treatment of these injuries. However, high-energy distal radius fractures with articular surface comminution and extension into the radial diaphysis remain a challenge for the treating clinician. The treatment goals for these fractures are to restore and maintain the length and alignment of the radius and to reestablish the congruity of the radiocarpal and distal radioulnar joints. 2 These goals are not always easily achieved. Radiocarpal-spanning internal fixation can be an effective treatment modality for high-energy distal radius fractures, relying on the principles of ligamentotaxis 3 to obtain an indirect reduction in the fracture. Burke and Singer 4 and Becton et al 5 introduced radiocarpal-spanning internal fixation of distal radius fractures in 1998 in 2 separate articles. Ruch et al 6 and Hanel et al 7 further refined this technique. The radiocarpal-spanning plate is introduced through limited incisions on the dorsal surface of the hand and forearm. Screws secure the plate to the second or third metacarpal shaft and to the radial diaphysis proximal to the fracture site. 6,7 Advantages of this technique over external fixation include elimination of pin-related complications, dorsal buttressing of the fracture, and increased construct stability, which may allow greater patient participation in transfers and other activities in the early recovery period. 6,8,9 In addition, the elimination of a bulky, unsightly, metal frame attached to the patient’s wrist may significantly improve the quality of life during the treatment period. 10,11 This is of particular importance in the geriatric population, where healing can take longer. 12
Similar to external fixators, the radiocarpal-spanning plate is implanted with the intent of removing it. However, it must often remain in place for long periods of time, especially in the geriatric patient. In 2 recent studies, the plate was removed at an average of 4 months, and in some cases, it remained in place for as long as 9 months. 6,13 During this time of immobilization, many patients are returned to full activity. Heavy loading of the wrist is certainly discouraged as it may negatively affect fracture healing, however, light use of the wrist and hand is permissible. The issue of transfers in the elderly population has not been investigated. This long period of immobilization may make a functional wrist position desirable. In addition to patients being allowed to return to activities, in the elderly, multiply injured patient, the use of the hand may be essential for rehabilitation. Traditionally, the radiocarpal-spanning plate has been applied with the wrist in a neutral position. 4 –7,9 In this position, Wolf et al 9 and Chhabra et al 8 showed that the internal radiocarpal-spanning plate is a significantly more stable construct than the spanning external fixator. This wrist position, however, is not optimal for function. Literature from the fields of occupational therapy and orthotics suggests that, to maximize function in activities of daily living, the wrist should be immobilized in 10° to 30° of extension. 14 –16 This position also maximizes grip strength. 17 –20 We investigated whether or not the biomechanical stability of an internal fixation with a radiocarpal-spanning plate is affected by bending the plate in situ to place the wrist in 15° to 30° of extension. Our hypothesis was that wrist extension would not sacrifice the stability of the construct.
Materials and Methods
The experimental design and unstable distal radius fracture model were based on previously published protocols and models. 9,21 –23 The 2.4-mm straight wrist locking compression plate (LCP) (170 mm; Synthes, Paoli, Pennsylvania), often referred to as a “spanning wrist plate,” was used for internal fixation throughout all experiments. The stiffness of the fixation construct was tested by applying axially directed forces through the flexor and extensor tendons, thereby simulating physiological loading across the wrist. The magnitude of the force applied was based on previously published work on the physiologic load across the wrist. 21,22
Preparation of Specimens
Ten fresh frozen cadaver upper extremities, 4 males and 6 females, with an average age of 71.75 years (range: 66-77 years) were used in this experiment. The specimens were dissected to remove the skin and subcutaneous tissues from the forearm and hand. The flexors and extensors of the wrist (extensor carpi radialis longus [ECRL] and extensor carpi radialis brevis [ECRB], extensor carpi ulnaris [ECU], flexor carpi radialis [FCR], and flexor carpi ulnaris [FCU]) were identified. The interosseous ligament, wrist capsule, wrist ligaments, flexor and extensor retinaculae, and the ligaments of the elbow joint were all meticulously preserved. The wrist flexor and extensor tendons were transected at the midforearm as described by Wolf et al. 9 Using a whipstitch technique, the ECU, FCR, and FCU were individually sutured to themselves with a number 1 vicryl suture creating a loop for later load application. The ECRL and ECRB were sutured together, and then a loop was created using the aforementioned technique. We elected to use a well-published model of metaphyseal instability in our study to place the onus of demonstrating stability on our subtle change into extension. This model has been used elsewhere 9,21 –23 and is used to model the most unstable fractures of the radius when evaluated in cadaveric specimens. To model an unstable distal radius fracture, a 1-cm portion of corticocancellous bone was removed centered approximately 1 cm proximal to the Lister tubercle (Figure 1). This provided a discontinuity in the distal radius as in previously published work. 9,23,24 The 2.4-mm straight wrist LCP was passed distal to proximal along the floor of the second extensor compartment. While ensuring that the fracture gap was maintained, a total of eight 2.7-mm cortical screws were used to secure the plate to the second metacarpal shaft and distal radial diaphysis, the maximum allowed by the construct. We used bicortical fixation, achieving fixation in a total of 8 cortices on either side of the fracture model.

An unstable distal radius fracture was modeled by a 1-cm osteotomy centered approximately 1 cm proximal to the Lister tubercle.
Experimental Setup
A subminiature differential variable reluctance transducer (DVRT) from MicroStrain (Williston, Vermont) with a DEMOD-DC signal conditioner (MicroStrain) was fitted into plastic blocks allowing positioning of the displacement transducer securely on the bone. The transducer was connected to a power supply and to a digital multimeter as in the work by Wolf et al. 9 We mounted the specimens in our custom-built apparatus, holding the arm in a vertical position as described by Wolf et al 9 and Wolfe et al. 23 Metal hooks were placed in the tendon loops to enable loading of the fracture through the tendons. The DVRT was mounted across the fracture site and held in place with 2 Kirschner wires proximally and 2 distally (Figure 2).
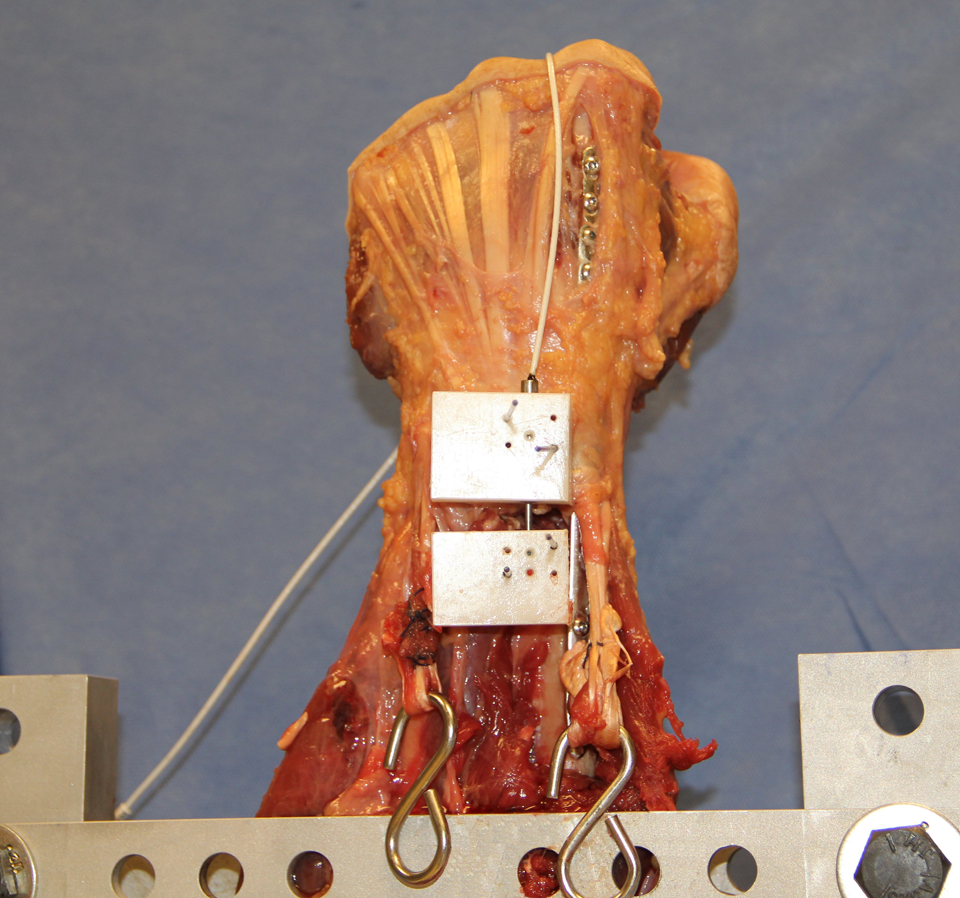
The 2.4-mm straight wrist plate was placed along the floor of the second extensor compartment. The specimens were placed in a custom-built apparatus, holding the arm in a vertical position. Hooks were placed in the tendon loops to enable loading through the tendons. The differential variable reluctance transducer (DVRT) was mounted across the fracture site and held in place with 2 Kirschner wires proximally and 2 distally. This enabled us to measure axial displacement across the fracture site.
The loading protocol was implemented as reported by Wolf et al 9 and Wolfe et al. 23 Each of the wrist flexor and extensor tendons was loaded by applying free weights to the tendons, attached via metal hooks and wires. To simulate the physiologic muscle tone across the wrist, a preload was applied to the wrist flexor and extensor tendons. 21,22 Preload consisted of 9.8 N applied to each of the ECU, FCR, and FCU tendons as well as to the ECRB/ECRL combined tendons. This created a baseline load of 39.2 N (9.8 N × 4) across the wrist joint. Once this load had stabilized, the specimen was subjected to a loading series consisting of 5 incremental loads applied through either the flexor (FCR and FCU) or the extensor (ECU and ECRB/ECRL) tendons. For each specimen, we randomized whether to start with the flexion or extension series to avoid any bias. 9 Random numbers were computer generated as described by Kernighan and Ritchie. 25 Once started, all 5 loads in the series were tested before switching. Following the completion of 1 loading series, all loads were removed from the specimen, and the model was allowed to stabilize for a duration of 10 minutes. A baseline load was again applied, and once stable, the opposite loading series was commenced. Each loading series consisted of incrementally increasing loads of 9.8 N applied to each of the flexor or extensor tendons, resulting in a total incremental increase of 19.6 N (9.8 N × 2). A loading series consisted of 5 loads, 19.6, 39.2, 58.8, 78.4, and 98 N. 9,23 Pilot testing determined that the sum force of 98 N was more than sufficient to allow maximum wrist flexion or extension.
Radiocarpal-spanning fixation with the wrist in extension can be accomplished by bending the plate to the desired degree of extension either prior to or after affixing it to the bone. We chose to bend the plate in situ because it enabled us to use standard fracture reduction and plate insertion techniques and allowed testing the same specimen with both the neutral and the extended plates. Thus, each specimen served as its own control. Large screwdrivers were used as bending irons and were placed in the screw holes adjacent to the plate segment that was to be contoured. This allowed us to be precise with regard to the anatomic location and degree of extension. In each case, the plate was contoured well distal to the fracture site, retaining the plate’s dorsal buttressing without affecting fracture reduction. At the conclusion of the experiment, the plates were straightened using the same technique and were not found to deform under 3-point bending with our greatest load of 98 N to any greater magnitude than unbent, unused plates.
Experimental Testing
First, the radiocarpal-spanning plate holding the wrist in a neutral position was tested. With the arm mounted and the DVRT in place, we proceeded following the steps outlined in the loading protocol. A baseline load was applied, resulting in an axial displacement at the fracture site. This displacement was captured by the DVRT and displayed as a voltage change in the multimeter. Once the model had stabilized, the initial voltage was recorded. We then continued with the loading protocol. After each load had been applied, the model was allowed to stabilize, and then, the resulting voltage output was recorded. Once both a flexion and extension series had been completed on 1 specimen, the plate was contoured using the in situ bending technique discussed previously. This placed the wrist in an average of 23° of extension (range: 15°-30°). The wrist extension was measured with a goniometer and verified to be within the proposed range. The specimen was then tested again, parameters and order of loading series being kept the same. The voltage output was again recorded.
Data Analysis
The protocol for this experiment was reviewed with a qualified biostatistician. A pre hoc power analysis was undertaken to detect a difference in the displacement of 0.09 mm based on the minimum detectable displacement reliably discerned radiographically. 9 With a detectable displacement of 0.09 mm between the neutral and extended positions and an α of .05, a sample size of 10 arms produced greater than 80% power. All computations and statistical analysis were performed using Microsoft Excel (Microsoft, Redmond, Washington) and were reviewed by the department statistician. The conversion, between the absolute value of the voltage difference at baseline and at each incremental load, to a metric displacement was calculated using the calibration equations for our specific displacement sensor. These equations were supplied by the manufacturer of the sensor (MicroStrain). The 2-tailed Student t test was used to compute P values. A standard 2-sided test was used to compute the true difference in displacement that would be detectable by this experiment after determination that our data points were normally distributed.
Results
As expected, based on prior studies of internal radiocarpal-spanning fixation, 9 we found a near linear relationship between fracture displacement and the amount of load applied (Figure 3). The mean fracture displacement measured over the 10 specimens with the wrist held in a neutral position was 0.23 ± 0.02 mm (mean ± standard error [SE]). With the wrist held in extension, the overall mean fracture displacement was 0.22 ± 0.02 mm (P = .75). In all tested loads, the mean fracture displacements were closely correlated, and we found no statistically significant difference between the neutral and extension plate positions (Figure 3). The average differences over all loads were 0.01 mm and were never greater than 0.02 mm for any individual load.

There was no statistically significant difference in fracture displacement with the wrist in a neutral position compared with extension for any of the loads tested. A near linear relationship exists between fracture displacement and the amount of load applied.
Comparing the neutral to the extension plate position in separate tests of flexion and extension loading revealed a similar pattern. There was again no statistically significant difference in the mean fracture displacement. Table 1 shows the mean fracture displacement for each load applied with the wrist held in neutral and in extension, separated by the type of loading. For flexion loading, the largest difference in mean fracture displacement detected was 0.03 mm and the average difference over all tested loads was 0.01 mm. For extension loading, the largest difference found was 0.01 mm and the average was less than 0.01 mm. There was no statistically significant difference detected (P = .77 and P = .88 for flexion and extension loading, respectively).
Fracture Displacement by Type of Load.a
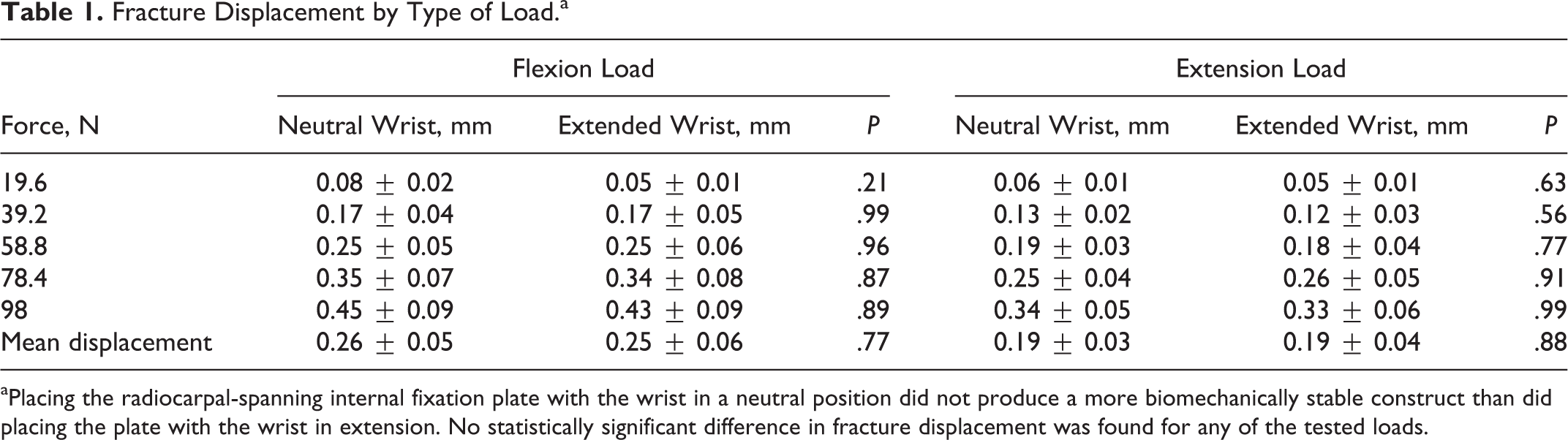
aPlacing the radiocarpal-spanning internal fixation plate with the wrist in a neutral position did not produce a more biomechanically stable construct than did placing the plate with the wrist in extension. No statistically significant difference in fracture displacement was found for any of the tested loads.
Analysis of the performance of the radiocarpal-spanning internal fixator in either flexion or extension loading, independent of the position of the wrist, revealed a greater stability with extension loading (Figure 4). This did reach statistical significance (P = .02) and was consistent with prior biomechanical studies of this type of fixation. 9
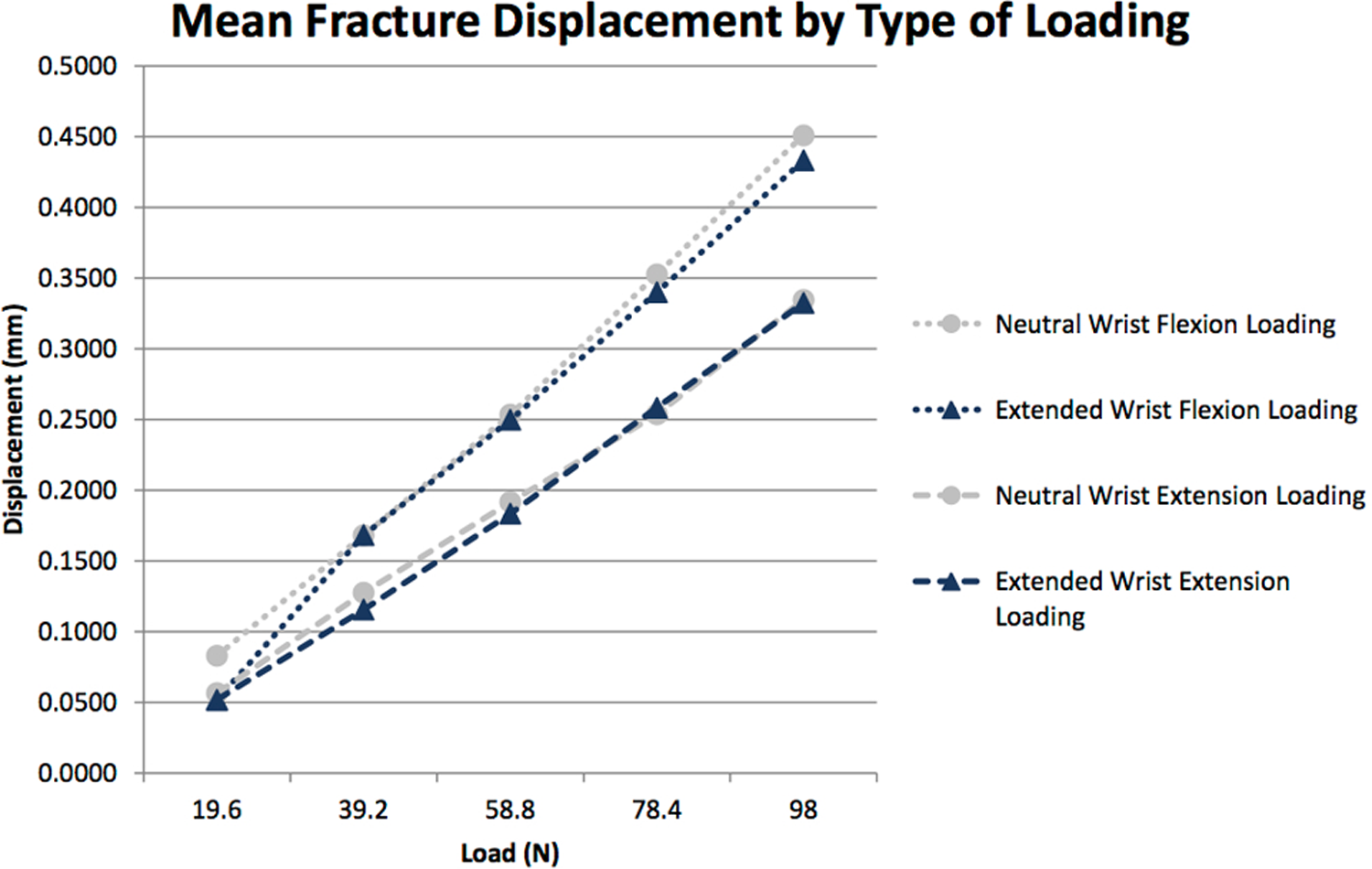
This graph shows our results with the neutral and extended wrist in either flexion or extension loading. When the wrist was loading through the extensor tendons, there was less displacement at the fracture site both with the wrist in neutral and extension.
Discussion
This cadaveric study shows no statistically significant difference in the biomechanical stability achieved with a radiocarpal-spanning plate applied with the wrist in neutral or in slight extension. To our knowledge, this is the first study examining the effects of wrist position on the stability of a distal radius fracture fixed with a radiocarpal-spanning plate.
Previous studies have shown that spanning internal fixation of distal radius fractures achieves greater rigidity than spanning external fixation. 9 This makes intuitive sense as the construct is closer to the bone. 26 The radiocarpal-spanning plate also has the advantage of providing a buttress that directly prevents dorsal displacement of distal radius fractures. 8 In this study and others, 7,9 the second metacarpal was used for the distal fixation. Other authors have used the third metacarpal citing improved stabilization of the lunate fossa by centralizing the distraction moment. 6 To our knowledge, there is no literature supporting the use of one metacarpal over the other. We used only cortical screws to hold the plate to the bone and secured bicortical fixation. Ruch et al 6 also reported using cortical screws, whereas Wolf et al 9 used locking screws. To our knowledge, there is no evidence that any one screw type is superior in radiocarpal-spanning fixation.
Decreased stability at the fracture site may lead to increased time required for fracture healing and remodeling. 27 Our findings reveal that even when the wrist is fixed in a neutral position, there is some fracture displacement under physiologic loads. Our results are significant because they show that fixation stability is not adversely affected by placing the wrist in slight extension. There are several reasons why placing the immobilized wrist in slight extension is desirable. This is a more functional position for most activities of daily living. 14 –16 It is also clear that grip strength is maximized in this position. 17 –20 In addition, many patients use keyboards or computer mice which are easier with wrist in extension. 28 –30 It stands to reason that patients with an immobilized wrist might be more productive if this wrist was held in slight extension rather than in neutral position. Finally, in the elderly, multiply injured population, the use and grip of a walker or other assistive devices may be easier with the wrist in extension.
There are many potential explanations for the increased gap motion in flexion relative to extension. The flexor tendons act at a greater distance from the center of wrist rotation. Therefore, the same weight or force acting through the flexor tendons should enact a greater flexion moment about the wrist than when exerted through the extensors. It should also be noted that the native wrist typically exhibits more flexion than extension even in the pathologic and arthritic state. It is also known that typically flexion outpaces extension in the individual bones of the carpus. Finally, the placement of the plate on the extensor surface of the bone may be the key factor in preventing some of the motion on the extensor side and relegating the greatest effect on the flexion side of the gap. Taken together, all of these factors may contribute to the greater effect of flexion than extension.
It may be argued that spanning plates need not be used in geriatric patients as permanent nonspanning fixation is both better tolerated and does not offer the additional risks associated with hardware removal. Although we agree with this argument, there are still at least some fractures for which permanent fixation is neither possible nor advisable. For some patients, the fracture pattern is not readily treatable with a permanent construct. These fractures have, in the past, been treated with external fixation or other forms of provisional fixation with the knowledge that removal of hardware may be necessary in the near future. Additionally, we have experienced, as is the case with the associated case report prepared as part of this article, patients for whom the healing of a distal radius fracture is not likely during their shortened life expectancy due to other illness. In these cases, where debilitating illness may lead to demise earlier than healing can be achieved in the radius with truly stable fixation, spanning wrist plates offer a reasonable alternative to current accepted fixation with volar or dorsal fixation. However, the placement of a spanning plate in these patients seems to be best in a more functional position, namely one of slight extension as opposed to the neutral position. Although relatively few patients warrant fixation in this extended position either temporarily or permanently, this possibility is reasonable to have at the ready.
This study has several strengths. Fresh frozen cadaveric specimens were used to closely mimic the in vivo mechanical milieu. The model of an unstable distal radius fracture used was based on previously published work. 9,23 This ensures, to the extent possible, that it accurately reflects important properties of an in vivo unstable distal radius fracture. A loading protocol was designed, also based on previously published work, to simulate physiological load across the wrist. 9,21 –23 There was enough power in the study to enable detection of a true difference in facture displacement as small as 0.09 mm. Each specimen served as its own control by being tested both with the wrist in neutral and in extension. This prevents bias from variation in specimen bone stock from being introduced into the study. The in situ bending technique used is well established in clinical practice, and instruments for this purpose were recently added to the AO Foundations list of approved products. 31 –34 The in situ bending technique is well established in the spine literature and has also been previously used in the treatment of distal radius fractures. 31,33,34 We acknowledge that bending the plate in situ will stress the bone-to-screw and bone-to-plate interfaces, which could potentially weaken the construct. However, this would only serve to refute our hypothesis and we therefore felt that it was safe to introduce this potential bias.
This study does have some limitations. No in vivo tests were performed, and only cadaveric specimens were used. The model used was that of an unstable extra-articular distal radius fracture. These results may therefore not be fully applicable to other fracture types. Although this fracture is relevant to the elderly population, no data were collected on the bone densitometric properties of our specimens that were entirely from an elderly cohort of cadavers. Bending the plate at the wrist ensured that the plate remained straight across the fracture site. This means that the buttressing effect of the plate, as well as the ability to obtain and maintain a reduction, should not have been compromised. However, these factors were not specifically evaluated in this study. The specimens were neither cyclically loaded nor loaded to failure, therefore, we cannot comment on the durability or strength of the hardware in either tested scenario. As in several previous biomechanical studies of distal radius fixation, this fixation construct was tested under physiologic loads through the wrist flexor and extensor tendons. 9,23,35
Similar to several previous studies, this study examines fixation stability in axial loading of an extra-articular distal radius fracture. 9,36,37 Other properties of reduction such as sagittal plane toggle or rotation of the distal fragment were not evaluated. Shortening of the radius has been shown to correlate with worse outcome. 38,39 As noted by Chhabra et al, 8 one of the main advantages of using a radiocarpal-spanning plate is the prevention of loss of reduction in the axial plane. For these reasons, we chose to examine our fixation constructs in axial loading through the wrist flexor and extensor tendons.
This study adds to the growing body of evidence showing the significant fracture stability that can be achieved with a radiocarpal-spanning plate. It further shows that applying the plate with the wrist in slight extension does not significantly compromise this stability. It is our opinion that having an immobilized wrist in a more functional position could greatly benefit patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health (Grant Number K08AR060164).