
Abstract
Aim
The aim of this study was to determine risk factors for the incidence of frailty in patients with distal radius fractures (DRFs).
Methods
In total, 116 patients (mean age, 66.3 ± 7.7 years) with DRFs were recruited. The participants were categorized into two groups, “frail” and “non-frail,” according to the presence or absence of frailty, respectively. The areal bone mineral densities (aBMDs) of the total hip, femoral neck, and lumbar spine were measured using dual-energy x-ray absorptiometry. The participants’ levels of resilience, depression, anxiety, nutritional intake, oral health-related quality of life, and social support were evaluated by self-reported questionnaires. The participants’ grip strength, gait speed, number of teeth present in their oral cavities, circumference of their upper arms and calves, and serum levels of vitamin D were also assessed.
Results
The participants in the “frail” group seemed to have lower aBMDs and muscle function and mass than those in the “non-frail” group. There were significant differences in grip strength, calf circumference, gait speed, and aBMD of the total hip, femoral neck, and lumbar spine between the groups. There were also significant differences in the levels of resilience and depression between the groups. A multivariate logistic regression analyses demonstrated that levels of sarcopenia, malnutritional status, and aBMDs of the total hip and femoral neck had significant relationships with the development of frailty in patients with DRFs.
Conclusions
An interdisciplinary approach involving the management of osteoporosis, sarcopenia, oral health, social relationships, and psychological support would be required for the proper management of DRF patients in preventing frailty.
Introduction
Frailty is commonly regarded as a type of geriatric syndrome featuring age-associated declines in physiological reserves and function across multi-organ systems, leading to increased vulnerabilities to adverse health outcomes. 1 In aged societies, the increasing numbers of frail elderly have become major issues owing to high social and medical costs. Therefore, identifying the risk factors for frailty and facilitating proper interventions to minimize frailty in elder populations are the main concerns of clinicians and policy makers of aged societies.
Fractures are considered to be important issues in geriatric medicine as they may lead to frailty, which, in turn, may increase the potential for falls and subsequent fractures. 2 Osteoporosis is one of the most common diseases in elderly populations and strongly correlates with an increased incidence of fractures owing to low bone mass and the microarchitectural deterioration of bone tissues.3-5 Frailty, osteoporosis, and sarcopenia share various risk factors and pathophysiological pathways such as aging, low body mass, decreased physical activities, low muscle mass, inflammation, and vitamin D deficiencies.2,6-8 Many previous reports have focused on the increased probability of frailty in patients with osteoporotic fractures,9,10 and other studies have suggested that frailty itself could cause an increased prevalence of osteoporotic fractures.11-16 Therefore, determining the risk factors of frailty in patients with osteoporotic fractures and the confounding factors correlating with the occurrence of osteoporotic fractures in the frail elderly is an important consideration of geriatric medicine in order to reduce the social and medical burdens of elderly populations.
Distal radius fractures (DRFs) are the most common upper extremity fractures in women and represent 17.5% of all types of fractures.17,18 Patients with DRFs showed an increased risk of subsequent fractures including hip and spine fractures, which could lead to locomotive problems, functional declines, and frailty.19,20 There are a limited number of studies that have investigated the comprehensive and interdisciplinary relationship between DRFs and frailty. One study examined the incidence rate of frailty in DRF patients, but this reports included only a small number of samples, which inevitably compromised the validity of the results. 21 Another study suggested the value of frailty evaluation criteria as predictive factors of preoperative complications and increased lengths of hospital stay for DRF patients who underwent surgical procedures. 22 However, this study utilized retrospective data and simplified frailty evaluation criteria which could have undermined the study’s value. Hence, the aim of the present study was to reveal the relationships between DRFs and frailty and determine the risk factors for the incidence of frailty in DRF patients.
Materials and Methods
Participants
In total, 116 patients (mean age, 66.3 ± 7.7 years; age range: 55–93) with DRFs were recruited from a tertiary care hospital from September, 2020 to December, 2021. A single orthopedic surgeon interviewed all the participants and gathered information regarding the participants’ underlying diseases, number of teeth present in their oral cavity, and current and past medications. Participants with histories of taking bone active medications including bisphosphonates, denosumab, and hormone modulating agents, and participants who were uncommunicative were excluded. Body mass index (BMI), upper arm circumference, and calf circumference were measured by a trained nurse. The research protocol was approved by the Institutional Review Board of the University Hospital. Informed consents were obtained from all participants.
Assessment of Frailty
Frailty was assessed in accordance with the criteria suggested by Fried. 23 The Fried frailty index is comprised of five criteria: weight loss, exhaustion, low physical activity, decreased walking speed, and grip strength. Unintentional weight loss and exhaustion were assessed by self-administered questionnaires. Walking speed over 4 m was measured using a timer with acceleration and deceleration phases of 1.5 m. The mean values were selected from three independent measurements. The lowest 20% of gait speed adjusted by sex and height based on the Korean frailty and aging cohort study was used to determine cut-off values. 24 Handgrip strength was measured by a hand dynamometer (Jamar® 5030J1 hydraulic hand dynamometer, Sammons Preston Rolyan, Bolingbrook, IL, USA) on the uninjured contralateral hand during the patient’s initial hospital visit. Handgrip strength was taken in a sitting position with a 90° elbow flexion and a neutral forearm position. The cut-off values of grip strength were determined from 20th percentile of grip strength stratified by sex and BMI quartiles based on the Korean frailty and aging cohort study. 24 Measurement of walking speed and grip strength were conducted by a trained orthopedic surgeon. Energy expenditure estimates (kcal/week) were calculated using the international physical activity questionnaire and metabolic equivalent scores were derived from vigorous, moderate, and mild activities from the self-administered questionnaires. A low physical activity level was defined as less than 495 kcal for men and 283.50 kcal for women. 25 If a participant showed three positive criteria on the Fried’s index, this participant was classified as “frail,” if a participant showed 1-2 positive criteria, the participant was classified as “pre-frail,” and finally, if a participant showed no positive criteria, the participant was classified as “robust.” We categorized participants into two groups, “frail” (N = 40, mean age = 71.5 ± 8.5 years) and “non-frail” (N = 76, mean age = 63.5 ± 5.5 years) including pre-frail and robust participants.
We also used the Kihon checklist to investigate the frailty status, which consist of seven domains including instrumental activities of daily living, physical function, nutritional status, oral function, homebound status, cognitive function, and mood. 26 The Kihon checklist is a self-administered questionnaire, consisting of 25 items concerning 7 domains.
Although not a disease, frailty is a multifactorial condition involving multi-organs and is related with to the general mental and physical health of the elderly. 1 Therefore, concerning diverse aspects of the elderly’s lives such as psychological status, social relationships, resilience, nutritional status, oral health status, and physical function are essential to reveal the risk factors for frailty. We adopted the Brief Resilience Scale (BRS), 27 the short form Geriatric Depression Scale (GDS), 28 the Geriatric Anxiety Inventory (GAI), 29 the Mini-nutritional Assessment (MNA), 30 the Oral Health Impact Profile-14 (OHIP-14),31,32 the Enhancing Recovery in Coronary Heart Disease (ENRICHD), 33 and SARC-F 34 to assess levels of resilience, depression, anxiety, nutritional intake, oral health-related quality of life, and social support and sarcopenia screening, respectively.
Evaluation of Bone Mineral Density
The areal bone mineral densities (aBMDs, in grams per square centimeter) of the total hip, femoral neck, and lumbar spine (L1-L4) were measured using dual-energy x-ray absorptiometry (DEXA) with a Hologic device (Horizon-W; Hologic Inc., Bedford, MA, USA). T scores of the aBMDs of the total hip, femoral neck, and lumbar spine were evaluated based on the value of aBMDs.
Biochemical Evaluation
Peripheral venous blood samples from each participant were collected between 8:00 a.m. and 11:00 a.m. after overnight fasting, to minimize circadian rhythm variabilities. The concentrations of serum 25-hydroxyvitamine D was assessed by high-performance liquid chromatography.
Statistical Analysis
Based on the Shapiro–Wilk normality test, data from the present study were normally distributed, and thus parametric tests were utilized. To compare the participants’ demographic characteristics, including age, sex distribution, BMI, and history of underlying diseases with the presence of frailty, independent T-tests, and chi-square tests were applied for continuous and categorical variables, respectively. Differences in the parameters, including grip strength, circumferences of the upper arm and calf, total Kihon checklist score, walking speed, energy expenditure estimates, SARC-F, ENRICHD, BRS, GDS, GAI, OHIP-14, number of teeth present, serum vitamin D levels, and aBMDs and T scores of the total hip, femur neck, and total lumbar were also compared between the two groups by independent T-tests and chi-square tests for continuous and categorical variables, respectively. A multivariate logistic regression analysis was used to analyze the potential risk factors of frailty in DRF patients adjusted for the potential confounders. Each variable with a significant outcome in the univariate analysis was integrated into the multivariate logistic regression analysis to identify interdependent contributions after adjusting for the presence of all variables to the dependent variable, the presence of frailty. Owing to the high collinearity among aBMDs of the total hip, femur neck, and lumbar spine, separate analyses of aBMDs of the total hip, femur neck, and lumbar spine were conducted. Gait speed and energy expenditure estimates were excluded from the logistic regression analysis because these two factors were already part of Fried’s frailty index for determining frailty.
Results
Demographic Characteristic of the Participants.

BMI, body mass index
Data obtained from independent T-test and descriptive values are shown as mean ± SE.
aData obtained from chi-square test.
*P < .05, **P < .001 by chi-square test or independent T-test.
Status of Frailty, Frailty Related Factors, and Bone Mineral Density of the Participants.
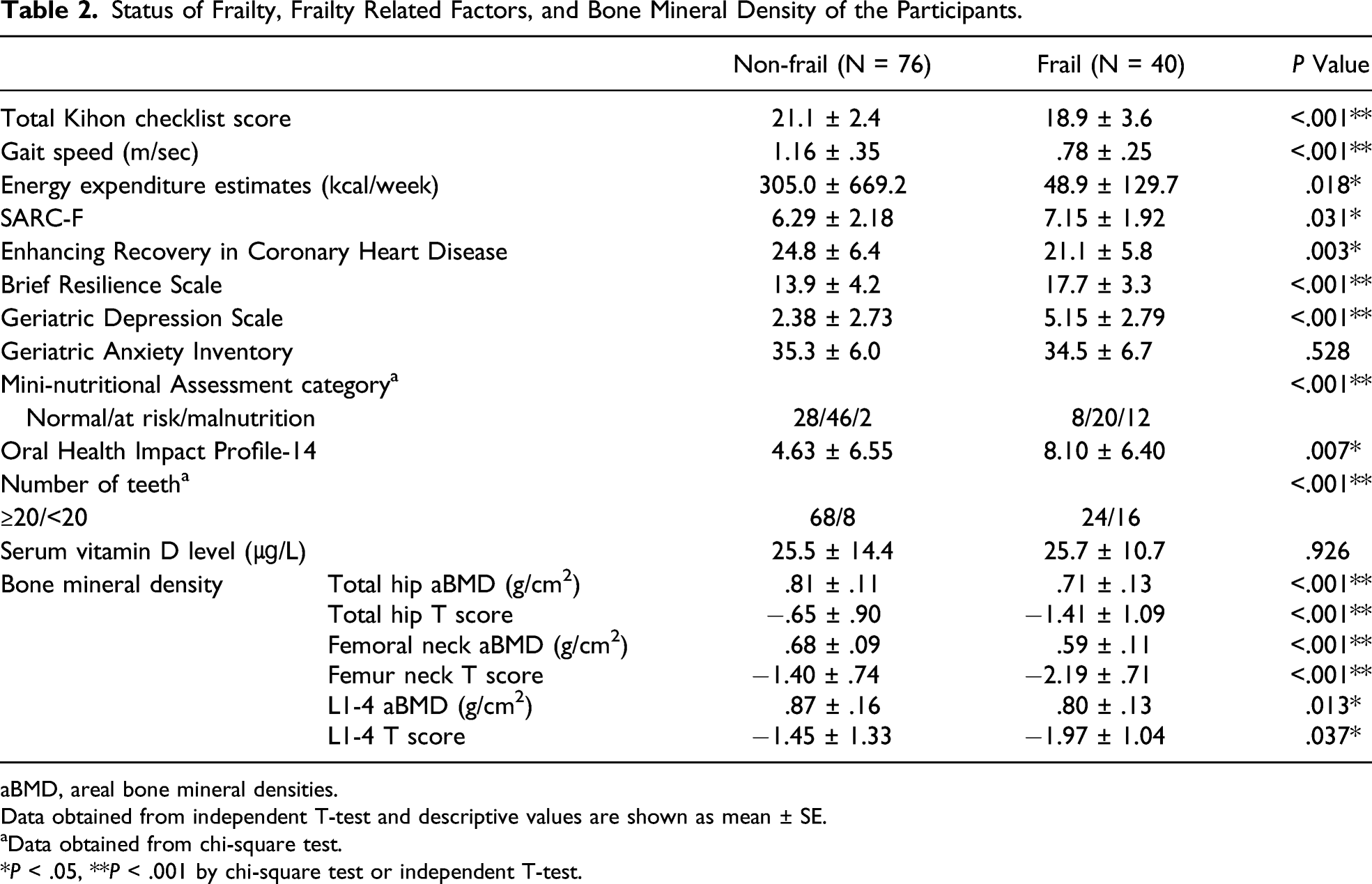
aBMD, areal bone mineral densities.
Data obtained from independent T-test and descriptive values are shown as mean ± SE.
aData obtained from chi-square test.
*P < .05, **P < .001 by chi-square test or independent T-test.
Adjusted Association Between Incidence of Frailty and Related Risk Factors.
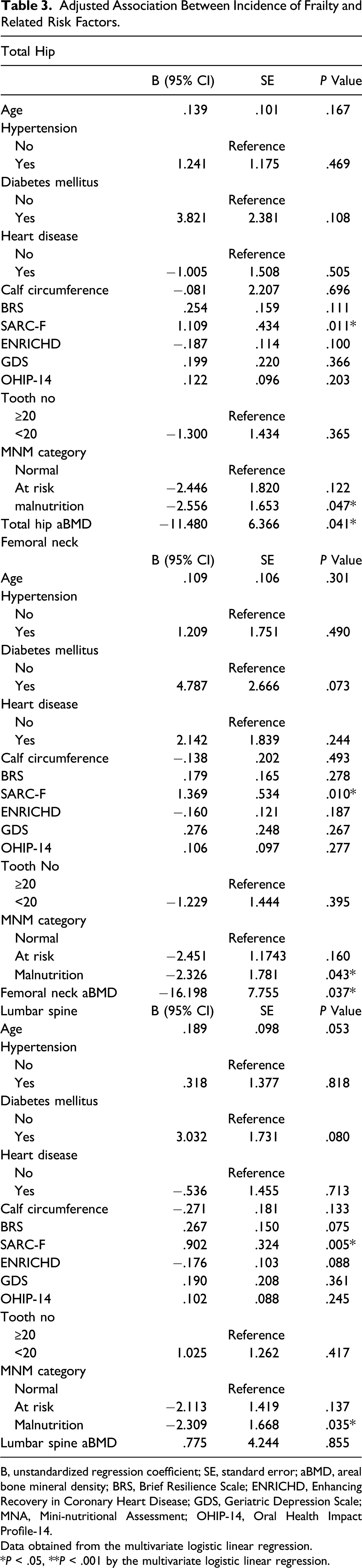
B, unstandardized regression coefficient; SE, standard error; aBMD, areal bone mineral density; BRS, Brief Resilience Scale; ENRICHD, Enhancing Recovery in Coronary Heart Disease; GDS, Geriatric Depression Scale; MNA, Mini-nutritional Assessment; OHIP-14, Oral Health Impact Profile-14.
Data obtained from the multivariate logistic linear regression.
*P < .05, **P < .001 by the multivariate logistic linear regression.
Discussion
The relationship between osteoporotic fractures and frailty has been discussed in previous literature. Several studies revealed the increased probability of frailty in patients with osteoporotic fractures9,10 and other reports have proposed that frailty itself has impacts on increased occurrence of osteoporotic fractures also.11-16 However, majority of these studies included patients with hip and spine fractures, which might directly correlate with locomotive problems and functional declines. Even though, DRF is not directly associated with locomotive problems and functional disabilities, it has a significant relationship with decreased bone microstructures and bone density, the main indicators of osteoporosis, and DRF patients showed increased risks for subsequent fractures including fractures of the hip and spine.19,20 To the best of our knowledge, there have been spares studies that have presented thorough and multidimensional insights into the relationship between DRF and frailty. Therefore, the aim of the present study was to reveal the relationships between DRF and frailty and determine the risk factors for the incidence of frailty in DRF patients.
In general, the elderly’s medical conditions may not be the result of a single disorder but instead may be the results of chronic conditions involving multiple organs. 1 Frailty is multidimensional, involving not only physical factors but social and psychological factors, as well. In the present study, we included factors related with BMD, and muscle mass as well as nutritional uptake, oral health, underlying diseases, anxiety, depression, resilience, and social supports to reveal the risk factors for frailty. Aforementioned results showed that decreased BMD and muscle function showed significant relationships with the development of frailty as previous reports have suggested.35,36 Interestingly, resilience, social support, and depression also showed significant associations with frailty in DRF patients. Despite previous reports revealing the importance of management of oral health37,38 and psychological problems39,40 in the prevention of frailty in community-dwelling elderly, the significance of these factors’ contribution to frailty in osteoporotic fracture patients has not yet been determined. Social isolation, depression, and poor oral health may lead to physical inactivity and malnutrition, which then can result in decreased bone mass and muscle atrophy41-44 and subsequently DRF. Hence, for the prevention of frailty in patients with osteoporotic fractures and, DRFs, monitoring bone density and muscle mass as well as the encouragement of social relationships, proper oral healthcare, and psychological support should be recommended.
Adequate nutritional intake is important for improving frailty, osteoporosis, and sarcopenia.45-47 The results from present study demonstrated the potential contribution of proper nutritional uptake in DRF patients for preventing frailty. Nutrition plays a critical role in the pathophysiology of frailty and the maintenance of bone 47 and muscle health.45,48 One study suggested that malnutrition could play a role as a mediator of osteosarcopenia and sarcopenia in the development of frailty. 45 Furthermore, sufficient protein and vitamin D uptake in the elderly has been recommended for the prevention of muscle and bone loss as well as the maintenance of sufficient leg and grip strength. 49 Associations between nutritional uptake, especially protein and the occurrence of post-operative surgical complications in patients with hip fractures50,51 and the importance of nutritional status for the improvement of activities of daily living and the incidence of subsequent fracture in DRF patients 52 have been proposed. However, the potential role of active nutritional intervention in terms of preventing frailty in DRF patients has not been suggested. Even though serum vitamin D levels did not show significant associations with frailty in aforementioned results, the role of proper nutritional uptake cannot be discounted in the management of DRF patients.
To the best of our knowledge, the present study is the first trial to reveal the risk factors of frailty in DRF patients with consideration of frailty’s multidimensional nature. However, there are still several limitations of this study. First, owing to the cross-sectional study design, causal relationships could not be derived. Second, due to the relatively, small sample size, the significance of the results could be inevitably compromised. Finally, because of the predominance of females with osteoporotic fractures, this study could not provide sufficient information about the risk factors for frailty in male DRF patients. Future prospective study with large sample numbers including adequate numbers of both male and female participants are warranted.
Frailty is a chronic and multidimensional condition in elderly and a comprehensive understanding of its features could be important for managing frail elderly population to develop strategies for preventing frailty. An interdisciplinary approach including psychology, dentistry, orthopedics, and endocrinology is essential for the proper management of DRF patients in order to prevent frailty.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by National Research Foundation of Korea (2020R1I1A1A01071537).