
Abstract
Objectives:
A meta-analysis to compare complication rates following volar or dorsal surgical fixation of distal radius fracture.
Methods:
A detailed search of PubMed®/MEDLINE® was undertaken to identify randomized and nonrandomized controlled trials published before 25 August 2012 that compared volar with dorsal fixation, in patients with distal radius fracture.
Results:
A quantitative meta-analysis of 12 trials (952 patients) was performed. There was no between-group difference in the overall rate of complications. Volar fixation was associated with significant increases in neuropathy (relative risk [RR] 2.19; 95% confidence intervals [CI] 1.27, 3.76) and carpal tunnel syndrome (RR 4.56; 95% CI 1.02, 20.44), and a reduction in tendon irritation, compared with the dorsal approach (RR 0.38; 95% CI 0.17, 0.86).
Conclusions:
Dorsal fixation offers a lower risk of neuropathy and carpal tunnel syndrome than the volar approach, but a higher risk of tendon irritation. Patients with a distal radius fracture can expect similar outcomes after volar or dorsal surgery.
Introduction
Fractures of the distal radius are very common, comprising around 20% of all fractures. 1 A substantial proportion of people who experience injuries to the distal radius are otherwise healthy. 2 The goals of treatment are to restore articular surface congruency, including radial height, radial inclination and palmar tilt.3,4 Depending on the displacement of the distal fragment, there is an increasing use of locked plate fixation by either a dorsal or volar approach: such fixation provides better reduction and stability, allows earlier mobilization and greatly improves the outcome compared with conventional T-plate fixation. 5
Dorsal fixation allows direct exposure and reconstruction of the joint by a capsular incision, 6 but requires dissection of the extensor retinaculum and subsequent plate positioning beneath this tendon, which often leads to tendonitis or tendon rupture. 7 As an alternative, volar fixation provides biomechanical stability for dorsally displaced and comminuted fractures. The significant soft-tissue dissection required with this procedure results in a high incidence of neuropathy and carpal tunnel syndrome, however. 8
Open reduction and internal fixation is one of the most commonly used surgical techniques for distal radius fracture.9,10 The purpose of this meta-analysis was to investigate the benefits and complications of volar and dorsal surgical fixation of distal radius fracture.
Materials and methods
Search strategy
Searches of the PubMed® and MEDLINE® databases were independently performed by two investigators (J.W. and T-B.Y.) using the following search terms (palmar OR volar OR thenar) AND (dorsal) AND (Barton fracture OR Colles fracture OR Smith fracture OR distal radius fracture OR distal radial fracture OR fractures of distal radius). Databases were searched from the earliest records up to and including 25 August 2012, without language restrictions.
Inclusion and exclusion criteria
Studies were considered eligible if they met the following criteria: (i) patients had a diagnosis of distal radius fracture, irrespective of diagnostic criteria, aetiology, associated pathology, sex or age; (ii) comparison of volar and dorsal approaches; (iii) data regarding complication rate provided; (iv) study reported relative risk (RR) and corresponding 95% confidence intervals (CI) or data required to calculate them. Exclusion criteria were: (i) case reports; (ii) reviews; (iii) animal studies; (iv) cadaver studies; (v) data unavailable for meta-analysis.
Data extraction and quality assessment
The following data were independently extracted and recorded by two investigators (J.W. and T-B.Y.): study characteristics (first author, year of publication, country of origin); implant type; sample size; numbers of patients with volar approach and dorsal approach; mean age; sex distribution; duration of follow-up; study design; number of complications. A complication was defined as an adverse treatment event recorded by the author(s) of the study. The main outcome measure of the meta-analysis was the overall complication rate.
Methodological quality of the selected studies was independently assessed by two investigators (W.L. and J.W.) using the methodology quality assessment scale for randomized clinical trials 11 and the nonrandomized study methodology quality assessment scale for nonrandomized trials. 12
Statistical analyses
Data were summarized using RRs and their corresponding 95% CIs. Homogeneity of RRs across studies was tested by the Q statistic with significance set at P < 0.01. The I2 statistic was used as a second measure of heterogeneity, with 0% indicating no evidence of heterogeneity and 25%, 50% and 75% indicating low, moderate and high heterogeneity, respectively. A random-effects model was used in the case of significant heterogeneity (P < 0.10 or I2 > 50%); in all other cases, a fixed-effects model was used. Sensitivity analysis was used to examine the influence of various exclusion criteria on overall effect size. Publication bias was assessed using Begg’s test 13 and funnel plots. All statistical analyses were performed using RevMan software, version 5 (The Cochrane Collaboration, Oxford, UK). A P-value < 0.05 was considered statistically significant, unless otherwise specified.
Results
The literature search initially identified 388 citations, of which 12 were eligible for inclusion in the meta-analysis (total n = 952).3,4,8–10,14–20 A flow diagram indicating the results of the literature search and study selection procedure is presented in Figure 1; characteristics of included studies are presented in Table 1.
Flow diagram indicating results of the literature search and study selection procedure for a meta-analysis comparing complication rates following volar or dorsal surgical fixation of distal radius fracture. Principal characteristics of the studies included in a meta-analysis to compare the rate of complications following dorsal or volar fixation of distal radius fractur. M, male; F, female; RCT, randomized controlled trial; LCP, locking compression plate; DNP, dorsal nail plate; DVR®, DVR® anatomic plate (DePuy, Leeds, UK); LoCon-T™, LoCon-T™ distal radial plate system (Wright Medical Technology, Arlington, TN, USA); LoCon-VLS™, LoCon-VLS™ distal radial plate system (Wright Medical Technology), NA, not available. Nonrandomized study methodology quality assessment scale (0–12). RCT methodology quality assessment scale (0–11). Mean value of follow-up. Individual follow-up point. Range of follow-up period.

The overall rate of complications was reported in all 12 studies. Complications included neuropathy, carpal tunnel syndrome, tendon rupture, tendon irritation, tenosynovitis, complex regional pain syndrome, screw loosening, infection, loss of reduction, healing problems and other complications. Using a random-effects model, there was no significant difference between the volar and dorsal approaches in the overall rate of complications (Figure 2). Substantial heterogeneity was observed (P < 0.001; I2 72%), but sensitivity analyses indicated that the overall RR was not substantially influenced by any single study. Exclusion of Zettl et al.
14
resulted in decreased heterogeneity, however (P = 0.03; I2 49%).
Meta-analysis of 12 studies that investigated the overall risk of complications following dorsal or volar fixation of distal radius fracture. CI, confidence interval.
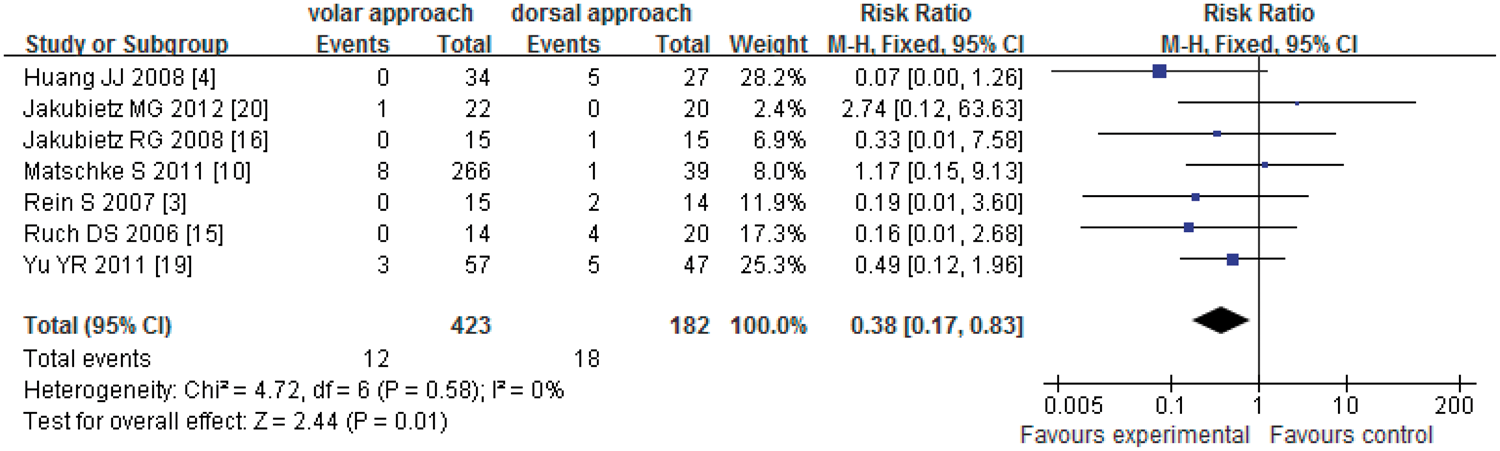
Subgroup analyses revealed that the volar approach was associated with a significantly increased risk of neuropathy (RR 2.19, 95% CI 1.27, 3.76; Figure 3)3,4,8,9,14–16,18–20 and carpal tunnel syndrome (RR 4.56, 95% CI 1.02, 20.44; Figure 4)4,8,10,18 compared with the dorsal approach. The risk of tendon irritation was significantly lower with the volar approach than the dorsal approach (RR 0.38, 95% CI 0.17, 0.86; Figure 5).3,4,10,15,16,19,20 There were no significant between-approach differences in the risks of tendon rupture (Figure 6),4,8,10,14,15,18–20 complex regional pain syndrome (Figure 7)3,9,18,20 or screw loosening (Figure 8).18,19,20
Meta-analysis of 10 studies that investigated the risk of neuropathy following dorsal or volar fixation of distal radius fracture. CI, confidence interval. Meta-analysis of four studies that investigated the risk of carpal tunnel syndrome following dorsal or volar fixation of distal radius fracture. CI, confidence interval. Meta-analysis of seven studies that investigated the risk of tendon irritation following dorsal or volar fixation of distal radius fracture. CI, confidence interval. Meta-analysis of eight studies that investigated the risk of tendon rupture following dorsal or volar fixation of distal radius fracture. CI, confidence interval. Meta-analysis of four studies that investigated the risk of complex regional pain syndrome following dorsal or volar fixation of distal radius fracture. 2CI, confidence interval. Meta-analysis of three studies that investigated the risk of screw loosening following dorsal or volar fixation of distal radius fracture. CI, confidence interval.




There was no evidence of publication bias (Figures 9 and 10).
Begg’s funnel plot for publication bias (with 95% pseudoconfidence limits) of 12 studies that investigated overall risk of complications following dorsal and volar fixation of distal radius fracture. RR, risk ratio; s.e., standard error. Begg’s funnel plot for publication bias (with 95% pseudoconfidence limits) of studies that investigated risk of complications following dorsal and volar fixation of distal radius fracture. RR, risk ratio; s.e., standard error.

Discussion
There are several treatment options for distal radial fracture, with anatomical reduction and stable fixation a choice for displaced and unstable fractures. 20 The desired fixation method is the one that can not only maintain satisfactory reduction, but also allow early motion to avoid joint stiffness and disuse atrophy. 5 Open reduction and internal fixation can be performed via either the dorsal or the volar approach, the choice of which is often based on the direction of fragment displacement and the extent of metaphyseal comminution. 21 Both approaches have disadvantages: the volar approach requires substantial soft tissue dissection and the dorsal approach is associated with extensor–tendon complications.22,23 Dorsal plating of distal radius fractures has been shown to have good results,21,24 and the functional outcome of volar plating has been reported.3,15 The majority of clinical studies have reported only the outcome of dorsal or volar plating, not the complications associated with each of these procedures.25,26
The different anatomical structures involved during volar and dorsal surgical approaches may have a role in the development of complications after plate application. A comparative study of the dorsal and volar approaches was unable to provide conclusive evidence to support a single, specific surgical technique. 3 Higher rates of volar collapse and late complications associated with dorsal plating were reported in a retrospective study of 34 patients with intra-articular fractures. 15 Contrary to this finding, improved outcomes were reported for 53 patients who received a T-plate via a dorsal approach. 1 The current meta-analysis revealed no statistically significant difference between dorsal or volar fixation in the overall risk of complications.
Anatomical differences (particularly the proximity of tendons and nerves to the volar or dorsal plate) can contribute to different complication rates. A volar approach was shown to be associated with median nerve compression and carpal tunnel syndrome, with some patients requiring carpal tunnel release during or after surgery. 3 This is because the volar approach involves retraction of the median nerve, which may directly (or indirectly) lead to neuropathy and carpal tunnel syndrome. 3 Others have suggested a correlation between the volar approach and a heightened incidence of postoperative neuropathy, although it was not possible to determine whether the incidence of carpal tunnel syndrome and major neuropathies was due to pre-existing carpal tunnel syndrome or to the volar approach itself. 19 As the volar approach fixes the plate within anatomical structures (including the median nerve), it is likely that this may contribute to increased incidence of carpal tunnel syndrome and neuropathic complications, compared with the dorsal approach.
The dorsal approach is associated with a high rate of local irritation or tenosynovitis of the extensor tendon,27,28 which is consistent with the findings of the current analysis where the risk of tendon irritation was significantly lower with the volar than the dorsal approach. This may be explained by the anatomy: the volar diaphyseal cortex is protected by muscle but the dorsal cortex is not, leaving the extensor tendons at risk from any screw protrusion.
In conclusion, the present meta-analysis indicates that dorsal fixation offers a lower risk of neuropathy and carpal tunnel syndrome than the volar approach, but a higher risk of tendon irritation. In terms of other complications, patients with distal radius fractures can expect similar outcomes after volar or dorsal surgery.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by the Young Teacher’s boosting project of the Fundamental Research Funds for the Central Universities in Central South University, China (2012QNZT095).