
Abstract
Introduction
Non-attendance with scheduled postoperative follow-up visits remains a common issue in orthopaedic clinical research. The objective of this study was to identify the risk factors associated with loss to follow-up among elderly patients with hip-fracture postoperatively.
Methods
A retrospective analysis of 1-year post-surgery was performed on patients aged over 60 years who underwent hip-fracture surgery from January 2017 to March 2019. Based on their completion of the appointed follow-up schedule, the patients were classified into 2 groups: the Loss to Follow-up (LTFU) Group and the Follow-up (FU) Group. Clinical outcomes were evaluated by Functional Recovery Score (FRS) questionnaires. Telephone interviews were conducted with patients lost to follow-up to determine the reasons for non-attendance. A comparative analysis of baseline characteristics between the 2 groups was implemented, with further exploration of statistical differences through logistic regression.
Results
A total of 992 patients met the inclusion criteria were included in this study, of which 189 patients, accounting for 19.1%, were lost to follow-up 1 year postoperatively. The mean age of the patients in the LTFU Group was 82.0 years, significantly higher than the 76.0 years observed in the FU Group (P < 0.001). The FRS for the LTFU Group was marginally higher than that of the FU group (84.0 vs 81.0), with no significant difference (P = 0.060). Logistic regression analysis identified several significant predictors of noncompliance, including advanced age at surgery, femoral neck fracture, hip arthroplasty, long distance from residence to hospital, and the reliance on urban-rural public transportation for reaching the hospital.
Conclusion
Postoperative follow-up loss was prevalent among elderly patients with hip fractures. Our study indicated a constellation of risk factors contributing to noncompliance, including advanced age, transportation difficulties, long travel distance, femoral neck fracture and hip arthroplasty surgery.
Introduction
Due to the acceleration of population aging, there is a global increase in the prevalence of osteoporotic fractures. The population of hip fractures per-year is expected to increase to 2.6 million in 2025 and to 6.3 million by 2050. 1 Many studies have reported high mortality rates following hip fracture, with cumulative 1-year mortality ranging from 20% to 40%.2-4 Moreover, only 30%–40% of these patients can recover their previous functional status, while approximately 22% transition from independent living to long-term care.5,6 To minimize complications and promote rehabilitation, postoperative management after hip fracture surgery is commonly regarded as an essential component of care for optimal outcomes.7-10 As an integral part of postoperative management, regular postoperative follow-up is conducted to monitor patient progress and identify potential complications, which commonly occur within the first year after surgery. 11 The American Academy of Orthopaedic Surgeons (AAOS) guideline highlights poor coordination among providers is attributed as the primary factor compromising quality care for patients with hip fractures. 12
Previous studies have reported differences in surgical outcomes between patients with complete and incomplete follow-up, suggesting that those lost to follow-up may be associated with poorer outcomes. 13 In a prospective study of 224 patients with rotator cuff tear, 102 (46%) patients were classified as loss to follow-up. Compared to those with regular follow-up, patients lost to follow-up exhibited worse shoulder functions in their last functional assessment questionnaires. 13 Loss to follow-up (LTFU) in clinical researches can also lead to reduced sample size and potentially generate inaccurate conclusions if the postoperative status of LTFU patients remains unknown.13,14 Moreover, a high rate of loss to follow-up may generate study response bias and undermine statistic validity. 15
A prospective study involving 136 patients with intertrochanteric hip fractures, revealed that a substantial 28.3% of the participants failed to complete the 1-year follow-up after surgery. 16 Additionally, a multicenter trial concerning femoral neck fracture reported a 24% loss to follow-up among elderly patients (aged ≥70 year). 17 In a retrospective review analysis of 2165 patients, which included a total of 8766 clinic visits across a 1-year period, Whiting PS et al discovered that patients who underwent surgery for hip or pelvis injury were more inclined to non-compliance with the first post-operative follow-up appointment. 18 In short, the attrition of patients during the postoperative recovery is a common challenge faced by elderly patients undergoing hip fracture surgery. The purpose of this study was to identify the demographic and clinical characteristics associated with an increased risk of patients being lost to follow-up in elderly population.
Materials and methods
With the approval of our hospital’s Ethical Committee, a retrospective analysis was conducted using Electronic Medical Records (EMR) to review patients aged over 60 years who underwent surgical treatment for hip fractures (femoral neck fracture or intertrochanteric fracture) between January 2017 and March 2019 at our urban level I trauma center. Patients who died during the 1-year postoperative follow-up period and those with incomplete data were excluded from the study. Upon discharge, comprehensive discharge instructions including information on follow-up appointments, attending physicians’ names, contact details, and directions to our clinic were provided to patients and their family members. All patients were required to adhere to a scheduled postoperative follow-up in our clinic at 1, 3, 6 months and 1 year after surgery. As there is no universally accepted definition of loss to follow-up in orthopaedic trauma research, we referred to previous definition of loss to follow-up in our trial.19-21 Loss to follow-up was defined as failure to complete follow-up appointments for orthopaedic evaluation before their final 1-year follow-up visit after surgery. Patients who missed their scheduled follow-up appointment were proactively contacted via phone calls and the WeChat application to remind them of their appointments and to reschedule their appointments. These patients were also flagged as loss to follow-up. Moreover, at each interaction, we meticulously updated and verified the patients’ contact information, including their current locations, phone numbers, and health statuses. Despite exhaustive measures taken, patients’ withdrawal from further follow-ups was beyond our control.
Based on the follow-up status, all patients were divided into 2 distinct groups: the Loss to Follow-up (LTFU) Group, comprising those who did not complete the follow-up schedule, and the Follow-up (FU) Group, consisting of patients who adhered to all follow-up appointments as prescribed. The baseline characteristics of patients and potential predictors for LTFU (eg, gender, employment status, living situation, and payment type for medical expenses) were analyzed. Payment types were classified as Medicare (Employee Basic Medical Insurance), Medicaid (Resident Basic Medical Insurance), other insurances (eg, commercial insurance and worker’s compensation), and self-pay. The distances between the participants’ residences and our clinic were determined by Google Maps, while the mode of transportation to the hospital was recorded. Additionally, fracture type and surgical methods were recorded. Moreover, the Functional Recovery Score (FRS) was utilized to assess the clinical outcomes of these patients by telephone interview and/or mailed questionnaires (Table I, Supporting Information). 22 Telephone interviews were conducted with patients who were lost to follow-up or their family members for investigating their main reasons for non-attendance and obtaining their current contact information. To ensure accuracy and consistency of patients’ questionnaires, all non-attenders received at least 2 telephone surveys or electronic questionnaires sent by WeChat app. Patients with incomplete information or inconsistent questionnaire answers and those who could not be contacted successfully twice were excluded. All participants or their legal guardians provided written informed consent to participate in the study and to have their information obtained from their treating physicians.
Statistical Analysis
The statistical analysis was conducted with SPSS software (ver. 18.0; SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was utilized to assess the normal distribution of quantitative variables. The Mann-Whitney U test was utilized for comparing quantitative variables. The Chi-square test or Fisher’s exact test was used to compare the qualitative variables as appropriate. Logistic regression models were employed to identify risk factors associated with loss to follow-up. Confidence intervals (CIs) were presented at the 95% level and the significance level was α = 0.05. P < 0.05 were considered as statistically significant.
Results
Baseline Characteristics of the 2 Groups.
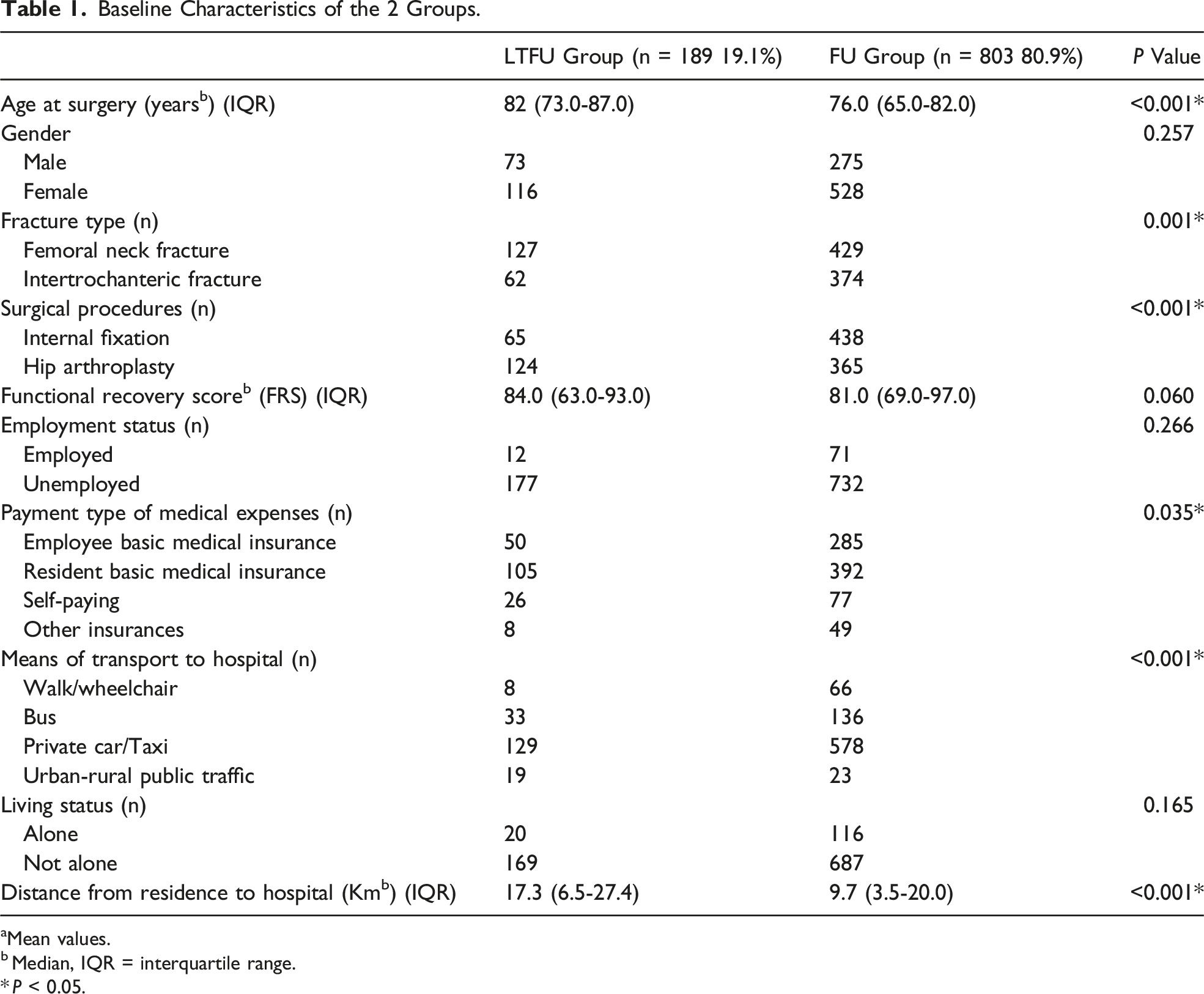
aMean values.
b Median, IQR = interquartile range.
* P < 0.05.
Potential Predictors of Loss to Follow-up one Year Postoperatively.

CI, Confidence Interval; OR, Odds Ratio; S.E., Standard Deviation; B, Beta.
* P < 0.05.
Primary Reasons for Follow-up Loss.

aAll patients stated 1 main reason.
Discussion
Lack of routine postoperative follow-up remains a persistent issue for orthopaedic surgeons, potentially imposing significant costs on the health care system and posing potential risks to individual patients.13,23,24 A standardized hip fracture program for geriatric patients has been reported to effectively reduce the 30-day mortality risk among high-risk individuals. 25 Conversely, patients who discontinued follow-up might have worse function and poorer prognosis.13,26 In addition, loss of follow-up would potentially bring about bias, reduce statistical power,14,27,28 and result in underestimation or overestimation of therapeutic effects. 29 A systematic review based on an analysis of 235 published reports concluded that the outcomes of patients lost to follow-up could alter the interpretation of results in randomized controlled trials. 30 Our findings revealed that loss to follow-up was a prevalent issue among our cohort of surgically treated hip fracture geriatrics. The rate of patient attrition in postoperative follow-up appointments displayed a gradual ascent, initially recording a 2.6% non-attendance rate for the first 1-month follow-up visit. This figure escalated to a significant 19.1% within the 1 year post-surgery, correlating closely with previously reported LTFU rates.31,32 In a prospective cohort study involving 1083 patients who underwent hip-fracture surgery one year postoperatively, 270 patients were found lost follow-up due to organizational issues and 69 patients could not be contacted anymore, resulting in a loss to follow-up rate of 31.3%. 33 It has been suggested that a loss to follow-up rate lower than 5% was associated with minimal bias, whereas a rate greater than 20% might potentially pose serious threats to the sensitivity and validity of research data. 34 Nevertheless, 1 simulation-based study indicated that a 20% loss to follow-up could substantially influence study outcomes, indicating that this rate might not be universally acceptable for orthopedic trauma studies. 35 In view of this, our research merely documented the loss to follow-up rate without predefining a significance threshold. However, our findings disclosed a rate that nearly approached the critical 20% threshold. This finding emphasized the crucial role of regular follow-up appointments and the necessity to intensify interventions aimed at improving patient compliance with their postoperative follow-up visits.
Several factors, including socio-economic demographic features as well as patient-related factors, might impact patients’ adherence to follow-up after surgery. The binary logistic regression analysis revealed that advanced age, femoral neck fracture, hip arthroplasty, long distance between residence and hospital, urban-rural public transportation for hospital visits were significant predictors for loss to follow-up 1 year postoperatively. In the present study, the average age of the LTFU group was higher than that of the FU group. Compared with the elderly, younger patients might be more likely to attend follow-up visits independently without relying on family members. Berg et al identified unmarried or unemployed status as independent predictors of loss to follow-up in a cohort study of 335 patients treated for metacarpal fractures, 10 which was attributed to social deprivation.10,36 However, there were no differences between the 2 groups in our study regarding employment or living status. The significant differences in patient age and living situation between our study and Berg’s series suggest a reduced impact of social deprivation on follow-up rates. Additional risk factors for loss to follow-up were found related to fracture type and surgical method. Specifically, patients with femoral neck fracture who underwent hip arthroplasty were more likely to be loss to follow-up in our study. Consistent with our observations, a secondary analysis of a cohort involving 2520 hip fracture patients revealed that patients who received arthroplasty for femoral neck fractures were more prone to LTFU than those subjected to internal fixation. 37 This disparity may stem from the fact that hip arthroplasty is perceived as a more definitive treatment, whereas individuals with internal fixation require ongoing surveillance to confirm fracture healing, which in turn fosters greater compliance with postoperative follow-up visits. 37
It has been suggested that loss to follow-up might be associated with poor clinical outcomes as dissatisfied patients seek further care elsewhere. However, our study demonstrated that the Functional Recovery Scores among the LTFU cohort were not significantly different from those of the FU group. Additionally, 71 (37.6%) patients in the LTFU group responded symptomatic improvement and voluntarily discontinued their scheduled clinic visits, citing this as the reason for their noncompliance with clinic attendance. A systematic meta-analysis of 8 prospective randomized trials, which included a total of 2206 patients, compared the effectiveness of arthroplasty and internal fixation in treatment of geriatric femoral neck fracture. The findings underscored that patients who underwent arthroplasty reported better function, fewer complications and less postoperative pain. 38 Patients with reduced postoperative discomfort may have considered subsequent follow-up appointments to be non-essential, thus potentially increasing their risk of becoming LTFU, which was emerged as the predominant cause for patient attrition in the study of Casp et al. 39 Joshi et al 40 reported a noteworthy finding of reduced failure in revision surgery and higher satisfaction results among those classified as LTFU subsequent to total knee arthroplasty, as opposed to patients who fully engaged in their postoperative follow-up. This observation posited that the absence of continued engagement in follow-up appointments did not invariably signal suboptimal clinical outcomes. Additionally, a national multicenter follow-up study had illuminated that patients’ perception of symptom improvement during the follow-up period could engender a perception that further follow-up may be deemed unnecessary. 41
Previous studies in the field of traumatic surgery and emergency medicine had indicated that distance to hospital and transportation expenses played significant roles in noncompliance with postoperative follow-up.42,43 Geng et al. concluded that inconvenient transportation and long distance to clinic were the most commonly reported reasons for discontinuing follow-up appointments. 44 Our findings also revealed a correlation between distance to hospital and noncompliance among our patients, as those from the LTFU group tended to reside farther away from the medical facility. However, a retrospective analysis of 307 patients who underwent surgical treatment after orthopedic trauma found no association between distance to the hospital and noncompliance. 45 It is worth noting that their trauma center served a relatively larger geographic area than ours, potentially leading to additional impact on patients’ transportation arrangements and resulting in more patients being loss to follow-up. Due to the challenges in accurately calculating transportation costs, our analysis was limited to analyzing the chosen mode of transport for accessing hospital. It was found that the convenience of patients' follow-up visits was a primary factor, as individuals in the LTFU group were more likely to rely on public transportation such as urban-rural coaches. This finding was consistent with the results obtained from the questionnaire survey, highlighting that 20.1% of patients in the LTFU group identified geographical distance to the hospital and transportation difficulties as primary factors contributing to discontinuation of follow-up.
Geriatric patients, often termed “transportation disadvantaged patients”, face unique challenges due to their complex medical needs and chronic physical ailments, making them less suited for public transport. 46 Furthermore, a great proportion of elderly patients with infirmity or at an advanced age, specifically 30.2% of those in the LTFU group, reported a lack of capability to continue their follow-up appointments. This finding underscored the pivotal role that the inconvenience of attending clinic visits played in this context. Additionally, 18 patients in the LTFU group, accounting for 9.5%, stated that they had opted for an alternate health care institution, due to inconvenience of accessing our hospital. Finally, the payment type of patients’ medical expenses was analyzed. Although the proportion of patients with resident basic medical insurance or at their own expense was higher in the LTFU group, no statistic differences were found in the logistic regression analysis. The public medical insurance system in our country, which covers the majority of the population, ensures that medical services are readily accessible to patients at a low cost. 47
Our study had several potential limitations that warrant acknowledgment. Firstly, it was dependent on accurate entry of databases. The absence of comprehensive information precluded us from analyzing additional factors such as life style, household income, and education level, which had been also reported to be associated non-compliance. Secondly, the study encountered challenges in addressing the socioeconomic and geographic disparities that undeniably influenced patients’ ability to adhere to follow-up appointments. Another issue was the potential for interviewer bias, as the survey outcomes hinged on the patients’ responses to telephone contact. To mitigate this, we simplified the questionnaires to enhance response rates and endeavored to ensure that all non-attenders received at least twice telephone surveys. We also excluded the incomplete or inconsistent information to minimize bias in our findings. Lastly, our study was initiated prior to the COVID-19 pandemic’s emergence, which resulted in substantial change in orthopedic clinical and surgical activity, as well as postoperative follow-up due to the implementation of social distancing policies. 48 To mitigate any potential confounding effects that the pandemic and its associated restrictions might have had on patient follow-up behaviors and clinical outcomes, we excluded patients who were part of the study during the pandemic period. Despite the inherent limitations, our research successfully identified elderly patients at an elevated risk of being lost to follow-up following hip fracture surgery.
Conclusions
Loss to follow-up was a prevalent issue among elder patients underwent surgery for hip fractures. Our research findings indicated that there were multiple factors contributing to noncompliance. Advanced age, femoral neck fracture, hip arthroplasty, long distance, and inconvenience to hospital were identified as risk factors of loss to follow-up within 1 year postoperatively. Furthermore, our study suggested that patients who were lost to follow-up after surgery were more likely satisfied with their clinical outcomes and perceived further follow-up as unnecessary.
Supplemental Material
Supplemental Material - Risk Factors for Loss to Follow-up of Elderly Patients After Hip Fracture Surgery: A Retrospective Cohort Study
Supplemental Material for Risk Factors for Loss to Follow-up of Elderly Patients After Hip Fracture Surgery: A Retrospective Cohort Study by Min Rui, Yujian Hui, Jiannan Mao, Tao Ma, and Xin Zheng in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Author Contributions
All authors participated in the design, interpretation of the studies, analysis of the data and review of the manuscript. M.R. and X.Z. designed the study and drafted the manuscript. Y.H. and J.M. reviewed the patients. T.M. analyzed the data. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has received the financial support from the National Natural Science Foundation of China (82272523, 81902244), Outstanding Youth Project of Anhui University natural science (2023AH020050), Wuxi Municipal Health Commission scientific research major project (Z202008) and Youth Scientific Research Project of Jiangyin Health Commission (Q202301).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.