
Abstract
Introduction:
Little research has examined postrehabilitation functional outcomes of periprosthetic hip fractures. Predicted functional deficits and acceptable rehabilitation outcomes for these patients are not established. This study aimed to compare functional outcomes of periprosthetic fractures to matched patients with total hip arthroplasty (THA).
Materials and Methods:
Cases with periprosthetic fracture (PPF) were matched for age, gender, and surgeon to primary THA cases. Only patients who had completed at least 1 year of rehabilitation were included. Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores were calculated for all surviving cases with PPF and primary THA. Secondary outcomes included length of stay and mortality. Statistical analysis was performed using Microsoft Excel and the 2-tailed Wilcoxon signed rank test. A P value of <.05 was accepted as indicative of statistical significance.
Results:
We identified 25 patients with PPF. Three patients were unsuitable for functional assessment. Of the cases with PPF suitable for functional assessment, 14 (14/22) were male. The median age of the PPF and the THA groups was 71 years and 68 years respectively. The median WOMAC score for the PPF group was 26 (interquartile range [IQR] 5.5-49.5) compared to that of the primary THA group, 3 (IQR 2.0-24.5; P < .05). In the PPF group, there were 7 deaths and 3 of the surviving patients had significant complications. The median length of stay in the PPF group was 13 days (IQR 10.5-35) compared to the matched group of 5 days (IQR 5-8.5; P < .05).
Conclusion:
Patients with PPF have markedly poorer functional outcomes than age-, gender-, and surgeon-matched patients with THA as well as prolonged length of stay. Future research should target the identification of factors that may improve functional outcomes in this growing cohort.
Introduction
With the ever-expanding volume of total hip arthroplasties (THAs) and aging populations worldwide, there is an increasing incidence of periprosthetic hip fractures (PPFs). 1,2,3 Patients with PPFs are time and resource intensive, and treatment varies according to patient physiology and the status of the implant. The status of the implant determines whether it is suitable for retention or requires revision. 4,5,6
Outline of Other Studies Reporting Functional Outcomes Following Periprosthetic Fracture About the Hip.
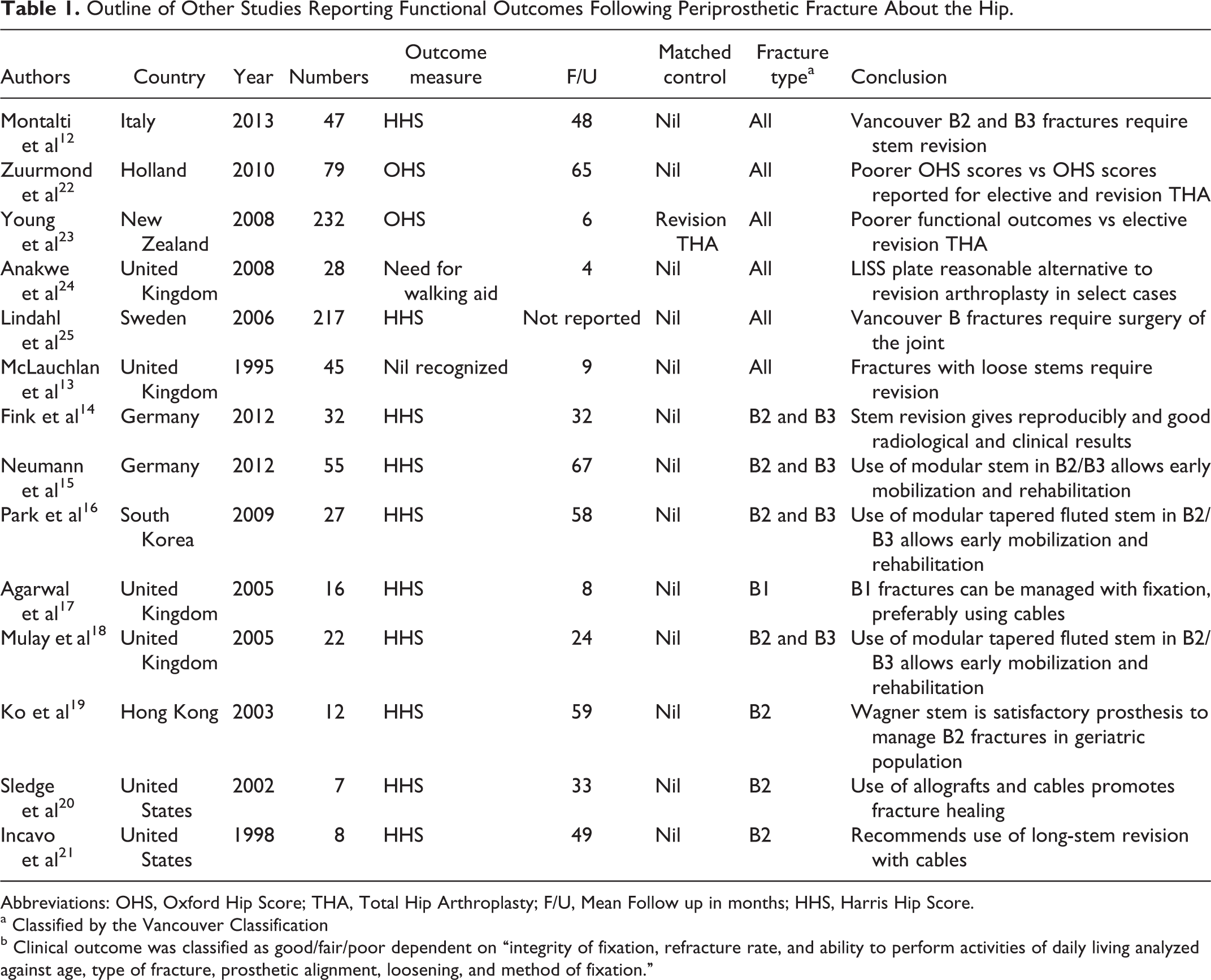
Abbreviations: OHS, Oxford Hip Score; THA, Total Hip Arthroplasty; F/U, Mean Follow up in months; HHS, Harris Hip Score.
a Classified by the Vancouver Classification
b Clinical outcome was classified as good/fair/poor dependent on “integrity of fixation, refracture rate, and ability to perform activities of daily living analyzed against age, type of fracture, prosthetic alignment, loosening, and method of fixation.”
It is known that periprosthetic fractures are notoriously difficult to treat and outcomes, for example, mortality, are generally considered poor. 26 The majority of deaths from PPFs have been shown to occur shortly after operative fixation. 10 This has left an unanswered question: What is the rehabilitation potential of patients who survive PPFs? Being a relatively new problem for surgeons, there is a paucity of data available which may be used to (1) measure the resulting decline in function following PPF and (2) provide a basis for realistic rehabilitation targets.
Our clinical observation is that patients who sustain PPF do not regain premorbid function and have significant functional deficit on completion of rehabilitation. This study aimed to investigate functional outcomes following periprosthetic fracture and quantify the persistent functional deficit caused specifically by the fracture episode. Therefore, patients were compared to controls matched for age, gender, and operating surgeon following primary THA. Secondary outcome measures include complications, morbidity, mortality, the need for reoperation, and the length of hospital stay.
Methods
Identification of Cases With PPFs and Matching to Joint Registry Cases
Details of the Periprosthetic Fracture Cohort Available for Follow Up.

Abbreviation: ASA, American Society of Anesthesiologists Score
a Age at time of surgery.
b Vancouver classification.
Collection and Collation of WOMAC Scores
Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores were calculated on both the surviving cases with PPF and the matched patients retrieved from the Joint Registry of the National Orthopaedic Hospital. 27 The WOMAC scores are routinely collected by the joint registry team. For the PPF cohort, the WOMAC scores were calculated on clinical review at follow-up by the lead author. Four patients did not attend the follow-up. In these cases, the WOMAC scores were obtained via telephone by the lead author. Patients who were too infirm to complete a functional assessment or were cognitively impaired were excluded from the analysis. For patients who died, official dates of death were sourced from the national registration body in the Republic of Ireland. 28
Collection of Biochemical, Radiological, and Descriptive Data
Other data sources included theater logbooks, medical records, and radiographic records. The variables recorded included age, sex, fracture type as classified by the Vancouver Classification, ASA score at time of fixation, medical comorbidities, presence of pre- and postoperative infection of prosthesis, and whether or not secondary surgery at the PPF site was required. 29,30 Fracture classification was extracted from the surgical notes and was confirmed in all cases by reexamination of the preoperative radiographs by 1 senior registrar (JFB).
Data management and statistical analysis were performed using Microsoft Excel (Health Service Executive, The Republic of Ireland), and the 2-tailed Wilcoxon signed rank test was used to test for statistical significance. A P value of <.05 was accepted as indicative of statistical significance. In the results, values reported are the median with interquartile ranges (IQR) in parentheses.
Results
Sample Description
There were 25 PPFs identified. No patient sustained more than 1 PPF. All 25 PPFs occurred greater than 30 days after insertion of original implant. One fracture was intraoperative, during revision of a primary prosthesis. Three patients were excluded from functional assessment due to either cognitive impairment or severe illness (advanced cognitive decline [2] and acute hospital admission for multiorgan dysfunction [1]). Of the 22 remaining cases with PPF, 14 were male (14 of 22). There were 7 mortalities in the PPF group (7 of 25) and no mortalities in the THA group. No patients were lost to follow-up. The median age at surgery for the died patients with PPFs was 81.3 (IQR 80.7-84.5) years compared to a 71.7 years (IQR 59.5-77.7) in those completing the functional assessment. The median age of the matched group was 68.0 years (IQR 59.5-77.0). The median ASA grade for the died group was 4 (IQR 3-4), while the median in those available for follow-up was 2 (IQR 2-2). Of the patients with PPFs, 2 were managed with revision of the implant with the 13 others undergoing open reduction and internal fixation around the in situ implant. Of the fractures, 11 were around the primary implants. Of these 11, 1 had the acetabular cup, but not the stem, revised previously.
Functional Outcomes and Length of Stay
Comparison of WOMAC Scores for Patients Matched For Age, Sex, and Consultant.a

Abbreviations: F/U, Follow up; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
a Age matched within 4 years with the exception of patient no. 11 where closest age was taken from registry.
Complications
Recorded Complications in the Periprosthetic Fracture Group.

a Deep infection requiring eventual removal of femoral plate
Mortality
Details of Patients Who Died From Periprosthetic Fracture.

Abbreviation: ASA, American Society of Anesthesiologists Score.
a Age at time of surgery.
b Vancouver classification.
Discussion
The aim of this study was to investigate functional outcome following PPFs about the hip using a recognized scoring system and compare the findings to a matched cohort of patients who had undergone primary THA. Using data from a standardized joint registry and a recognized mobility outcome score, it was possible to match patients with PPF to patients who underwent primary arthroplasty and control for age, sex, and operating surgeon. We found that when both the PPF group and the control THA group had completed a year of rehabilitation, patients post-PPF fixation had markedly poorer WOMAC scores. Patients with PPF also had a significantly longer length of stay compared to patients who underwent primary arthroplasty.
To our knowledge, this study is the first of its kind comparing functional outcome of patients with following fixation and match to this degree. Zuurmond et al compared functional outcomes of PPF versus reported elective primary and revision arthroplasty outcomes but did not match the cases to controls. Lindahl et al examined quality of life (as measured by the EQ-5D index) in patients postfixation of PPFs when compared to patients 1-year posthemiarthroplasty but did not compare functional outcomes. 22,23,25 Young et al performed a case series of patients undergoing revision arthroplasty following PPF matched to patients undergoing elective revision arthroplasty. However, patients undergoing open reduction and internal fixation without exchange of any prosthetic component were excluded from this study. With the inclusion of fractures in which the prosthesis is retained, and also by matching for operating surgeon as well as age and sex, we believe our study is novel.
Our finding that patients who sustain PPF have poorer functional outcomes is consistent with conclusions made by others. McLauchlan et al reported a decrease in activities of daily living in 17 of the 34 cases with PPF. 13 In this study, functional outcomes were classified into good, fair, and poor based upon having no decrease, some decrease, and marked decrease in activities of daily living, respectively, but no validated functional outcome score was used. Zuurmond et al reported a Oxford hip scores on 35 patients with a mean follow-up period of 64.9 months. 22 They found a significantly poorer Oxford hip score in patients who had a PPF around a revised implant compared to those who fractured around a primary implant. Young et al compared outcomes of 123 patients following PPF with patients undergoing elective revision THA (matched for age and sex) using the Oxford 12 hip score (OHS12). 23,31 They showed a statistically significant increase in mean OHS12 for cases with PPF compared to cases with elective revision THA (29 vs 24, respectively).
Kamineni et al published a series that focused on using plate and cable fixation to manage PPF. They reported on 15 patients and found slightly disparate results to our study—3 requiring further surgery and 13 having reached premorbid mobility at the time of discharge home. 32 Unfortunately, without the use of an objective functional outcome score, meaningful comparison with this study is difficult. Anakwe et al reported on using Less Invasive Stabilisation System in 28 patients with PPF all aged older than 70 years. 24 In this study, 5 patients died, 5 were discharged to rehabilitation prior to eventual return home, 2 discharged directly home, and 2 to long-term care. In total, 9 of the surviving patients required placement to long-term care. These findings for postoperative mortality and complications are very similar to the findings in our study. Four patients required reoperation and 1 developed a deep infection postoperatively. All 5 deaths occurred within 1 year, which is similar to our own findings where 5 of the 7 deaths occurred within 1 year.
At 7 of 25, our cumulative mortality was higher than that quoted by others in the literature and is markedly higher than observed mortality rates following primary THA. Bhattacharyya et al compared survival of PPFs to a matched cohort of both patients with hip fractures and elective hip or knee arthroplasties and quoted a 1-year mortality rate of 11%. 7 However, unlike Bhattacharyya et al, our study focused on PPF only about the hip. Interestingly, following Kaplan-Meier survival analysis Bhattacharyya et al concluded that patients with a PPF have an increased mortality rate compared with similar patients undergoing joint replacement and have a mortality rate similar to that of patients with hip fracture—this was despite the matched hip fracture cohort having a lower Charlson Comorbidity Index. This contrast in mortality rates for elective joint replacement and PPF is consistent with our study. It is worth noting that the median ASA in our mortalities was markedly higher than in the PPFs available for follow-up; therefore, the died group were much higher risk surgical candidates from the outset.
We acknowledge this study has some inherent limitations. With a total of 25 patients, our sample size was small; however, no patients were lost to follow-up. Periprosthetic fractures are a heterogeneous group of injuries with differing management strategies depending on whether the implant is loose; therefore, investigating PPFs as a single group may be seen as simplistic. We must also acknowledge that this is a retrospective study and we have relied on medical records being completed appropriately. As such, inherent to any study of this nature, it is possible that we have underestimated to incidence of complications in the postoperative course following PPF fixation. We also considered using a cohort of patients undergoing revision arthroplasty or hemiarthroplasty for intracapsular fracture as the control group. However, we concluded that using the primary arthroplasty group as a control made it more likely that only the PPF influenced changes in functional status from the original THA. Any identified difference in WOMAC score could then be better attributed to the PPF.
Conclusion
We found that following fixation of PPF, postrehabilitation functional outcomes were significantly poorer than an age-, surgeon- and gender-matched cohort who had undergone primary THA. Consistent with previous work, the median length of hospital stay was significantly longer in the fracture cohort reflecting the greater surgical complexity and cost associated with treating PPFs.
Footnotes
Authors note
The authors grant exclusive license to published the below material to Sage Publications on acceptance for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.