
Abstract
Introduction:
As a result of increasing longevity, we are seeing more elderly patients with complex medical co-morbidities who sustain hip fractures requiring surgical management. The aim of this study is to understand and analyze the effect of preoperative medical comorbidities and associated low physiological reserve status on functional rehabilitation outcomes following surgical management of hip fractures.
Materials and methods:
This study conducted a retrospective analysis of 73 patients who fulfilled the inclusion criteria .We utilized the de Morton Mobility Index (DEMMI) scores pre surgery and at the time of discharge from hospital following a period of rehabilitation as a measure of their pre and post-surgery functional status. The Physiological and Operative Score (POSSUM) was used as our tool to objectively quantify medical co-morbidities including but not limited to cardiovascular and pulmonary conditions.
Results:
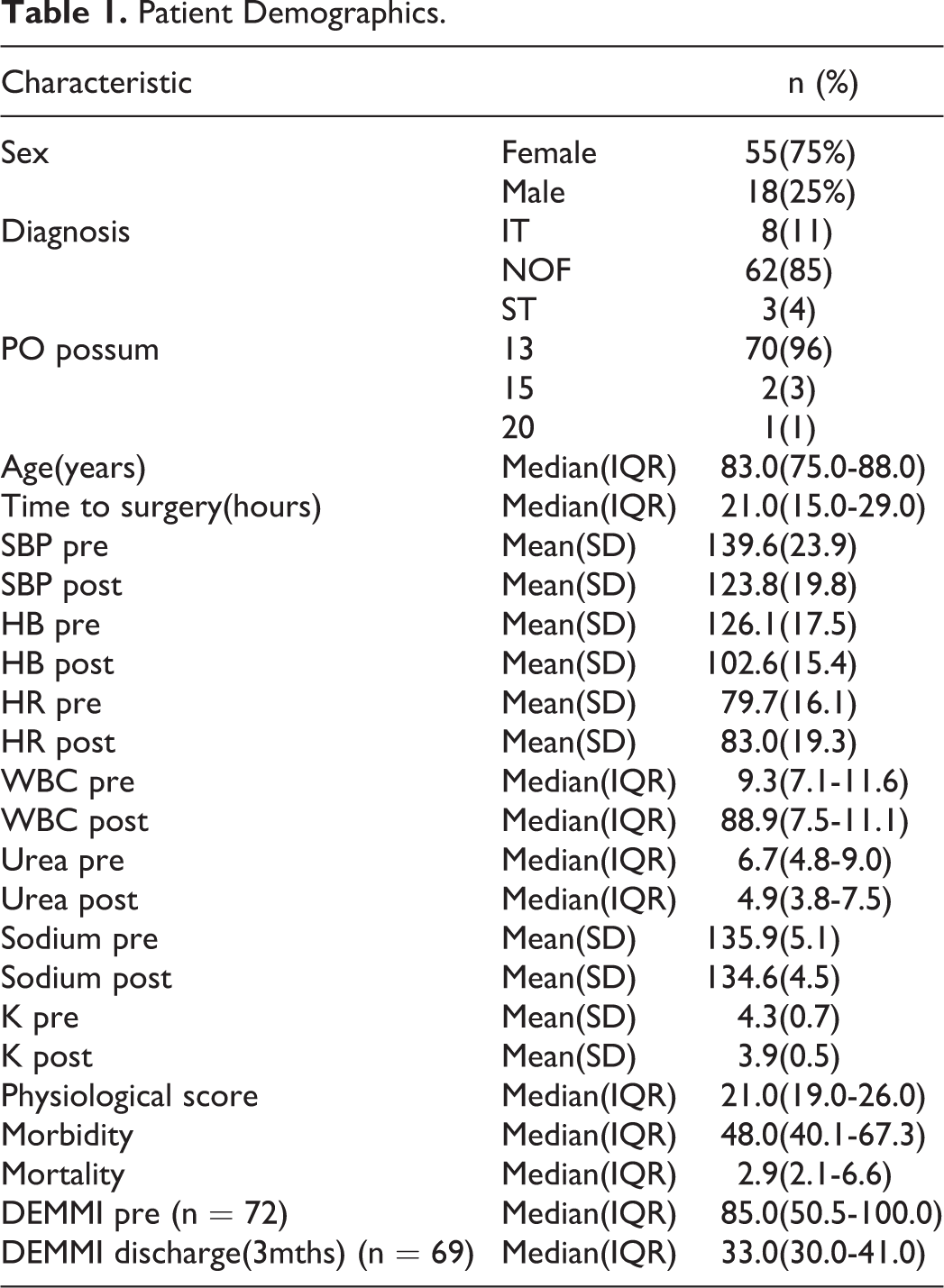
The median age of our study population was 83 years of which 55(75%) were female. Time to surgery was a median of 21.0 hours, IQR (15.0-29.0), with a median physiological score of 21.0, IQR (19.0-26.0), the median pre surgery DEMMI was 85.0, IQR (55.5- 100.0) and the median DEMMI at discharge was 33.0, IQR (30.0-41.0).There is a moderate correlation between DEMMI pre and DEMMI at 3 months, 0.38 that is statistically significant, p = 0.001.
Discussion:
The effect of medical co- morbidities which causes the patient to have a poor physiological reserve even when coupled with the effect of the operative stress have no significant negative impact on the 90-day functional outcome of these patients.
Conclusion:
This study demonstrated that the presence of medical comorbidities in patients who require surgical management of hip fractures would not adversely affect their rehabilitation outcomes. The preinjury functional status of a patient is a significant factor in predicting functional rehabilitation outcomes.
Keywords
Introduction
The prevalence of hip fractures is rising and can be attributed to the increase in our aging population. ANZ Registry Data analysis have shown that we will be dealing with approximately 6.3 million hip fractures per year by 2050. 1 71% of the patients with hip fractures live at their own house and the rest are residents of aged care services. Studies have shown that at the 6 month mark following surgery for hip fractures only 50% of the patients were able to regain independence with activities of daily living(ADL). 2,3 The 1-year mortality for hip fractures ranges from 8.4% to 36%. This imposes a heavy burden on the health care system as well as the community.
Patients who sustained hip fractures with multiple medical co-morbidities on admission had a greater risk of postoperative complications and increased mortality. 4 The patients who sustain hip fractures are associated with significant loss of mobility, independence and quality of life. 5 Beringer et al showed that only about 40% of hip fracture patients returned to pre-injury level of mobilization. 6 The high mortality and morbidity associated with fragility fractures of hip could be attributed to an interplay of multiple factors including intensity of trauma, time and type of surgery, presence of medical co-morbidities along with a low physiological reserve status. 7 However there seems to be a deficiency of data around the effect of these co-morbidities on functional rehabilitation outcomes.
Early identification of the positive and negative predictors of outcome after hip fractures will not only help improve outcomes for patients but also assist in planning and utilizing our resources to provide the best care. Copeland et al 8 developed the Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity (POSSUM) scoring system, in which 12 physiological and 6 operative factors are scored. These scores are further used for logistic regression analysis to generate 2 equations to predict mortality and morbidity. Wright et al 9 further concluded that POSSUM scores could be employed to accurately predict the morbidity in patients with hip fractures and also be used to predict the probability of complications after surgical management of hip fractures.
The Physiological component of POSSUM consists of various parameters like age, cardiac risk factors, systolic blood pressure, heart rate, Glasgow Coma Scale (GCS), Hemoglobin levels, white cell counts, urea, sodium, potassium and ECG changes. 8 Hence, we employed this tool to provide us an objective quantification of the patients’ comorbidities.
Aim of the Study
From the literature review conducted we formulated our hypothesis that patients with medical co-morbidities could be at high risk during and after hip fracture surgery and so their morbidity and mortality rates are high which in turn would naturally reflect adversely on functional rehabilitation outcomes.
Our aim is to put this hypothesis to test using retrospective analysis of data to study the effects of pre-injury medical co-morbidities which tend to categorize certain patients as high risk for hip fracture surgery and their functional rehabilitation outcomes. The secondary aim of the study is to identify the role of other factors if any that may be affecting functional rehabilitation outcomes in patients following hip fracture surgery.
Material and Methods
The present study was approved by the institutional review board for the local hospital. Patients admitted to the local hospital were initially assessed and screened for the neck of femur (NOF) pathway. This included a detailed assessment of their medical history, pre-injury functional status using the de Morton Mobility Index (DEMMI)scores and relevant investigations. The DEMMI scores were calculated by the allied health professionals who were trained to accurately score the patients. The data was retrospectively analyzed for patients who were admitted to the hospital with hip fractures between the years, 2014 to 2016.
The inclusion criteria employed included age > 60 years, non-pathological fractures without radiological features of osteoarthritis in the hip and underwent cemented hemiarthroplasty and undisplaced stable neck of femur fracture fixed with DHS.
The exclusion criteria was age <60 years, patients who were bed ridden prior to sustaining the fracture, patients with cognitive impairment as they could not effectively participate in rehabilitation, those with pathological fractures, subtrochanteric fractures and unstable intertrochanteric fractures with intramedullary nailing as a method of fixation.
In this study we used POSSUM score (Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity) to establish the patients physiological reserve status and medical co-morbidities. Statistical analysis was performed using STATA 15. Categorical variables were summarized by frequencies and percentages and continuous variables by means and standard deviations or median and interquartile range for non-normally distributed variables. Pearson’s correlation coefficient, or Spearman for non-normally distributed variables was used to assess for associations between DEMMI at 3months and physiological score/ DEMMI pre op. Weak correlation was defined <=0.3, moderate >0.3 and <=0.6, strong >0.6.
Results
The study population consisted of 73 patients with a median age of 83.0 years, IQR (75.0-88.0) of which 55(75%) were female. Two male patients died. Time to surgery was a median of 21.0 hours, IQR (15.0-29.0), with a median physiological score of 21.0, IQR (19.0-26.0) and median DEMMI at 3 months post-surgery 33.0, IQR (30.0-41.0). Results are displayed in Table 1.
Patient Demographics.
There is a moderate correlation between DEMMI pre op and DEMMI at 3 months, 0.38 that is statistically significant, p = 0.001. There is a very weak correlation between physiological score and DEMMI at 3 months post-surgery, not statistically significant. Results are displayed in Table 2.
Correlation with DEMMI Discharge, n = 69.

Discussion
To our knowledge this is the first study that has been conducted to objectively analyze the effect of medical co-morbidities on the functional outcomes of patients after sustaining a hip fracture. We found that a patient’s pre-injury functional status is the best predictor for the functional outcome following the treatment of the fracture which includes surgery and inpatient rehabilitation. The effect of medical co- morbidities which causes the patient to have a poor physiological reserve even when coupled with the effect of the operative stress have no significant negative impact on the 90-day functional outcome of these patients. This observational study sought factors that could independently predict the functional outcomes after hip fracture and shows that timely peri-operative management of patients categorized as high risk is vital for good functional outcomes.
The most important predictor of survival after geriatric hip fracture is shown to be the ASA score. 10 Dawe et al 11 has shown that ASA scores of 4 and 5 are independent predictor of survival. But the predictive power of ASA is low in patients with ASA 2 and 3. 10 Their study 11 has also shown that Creatinine level is a significant parameter that could predict mortality. This is not considered in the ASA scoring system. The POSSUM score has been validated to be a predictor of mortality and morbidity 12 in patients with hip fractures. The POSSUM system accounts for the physiological reserve of the patient and also considers BUN (Blood Urea and Nitrogen) levels while calculating the scores, so we used this to evaluate the physiological reserve status of our patients and also as a prediction toll for morbidity and mortality in them. The study has shown that neither the physiological score nor the operative score has any effect on the rehabilitation outcomes of these patients.
Cognitive impairment is a key indicator for mortality after hip fractures. 13 It has been demonstrated that mild to moderate impairment of cognition is associated with increased nursing home admission and mortality after hip fractures. 14 In our study we excluded patients with preinjury cognitive impairment as this can skew the data and an accurate analysis of medical co-morbidities cannot be interpreted. Pre-operative identification of patients at high risk followed by early involvement and management of those patients by the ortho-geriatric team was associated with a lessened risk of development of delirium post operatively which also allowed early and active participation in rehabilitation. Early intervention by the ortho-geriatric team has shown to have a positive effect on the general outcome of patients including but not limited to improved mobility. 15 All our patients where managed by ortho-geriatric team during the peri-operative period.
There are various instruments that can be used to assess mobility in geriatric patients. In patients with hip fractures a uni-dimensional measure of mobility is often used, however the Functional independence measure(FIM) and Barthel Index scores can provide multidimensional assessments. 5 The de Morton Mobility Index (DEMMI) is a uni-dimensional measurement instrument which is validated for measuring mobility of patients with hip fractures during or following rehabilitation. The DEMMI scores were recently validated and it has shown sufficient psychometric properties to be used in patients with delirium. 16 The DEMMI score has a greater advantage in confirming the interval nature of the scale when compared to the Barthel index as it can demonstrate the improvement in rehabilitation outcomes with nominal data. 5 This helped us to accurately analyze the preinjury status and rehabilitation outcomes following hip fracture management across all patients without confounding effect from any possible delirium.
In this study we excluded patients who had significant dementia as they would not have been able to actively participate in the rehabilitation program. This results in a lack of generalizability among patients admitted with hip fractures however it proves that despite poor pre-operative physiological reserves due to medical co-morbidities, patients who have a high level of function prior to injury can have good functional outcomes after surgery and appropriate rehabilitation.
Conclusion
To summarize, the preinjury level of functioning is one of the most significant predictors of rehabilitation outcomes after surgical management of hip fractures and is independent of their pre-operative comorbidities and level of physiological reserve.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.