
Abstract
Introduction:
Life-threatening hemorrhage associated with low-energy pelvic fracture has been described in single cases in the literature. However, there is limited evidence available on the bleeding risk associated with hemodynamically stable osteoporotic pelvic fractures. The objective of this study was to estimate the bleeding risk associated with low-energy osteoporotic pelvic fractures in the elderly population.
Materials and Methods:
A retrospective review of patients aged > 65 years old with pelvic fractures admitted between 2015 and 2018 was performed. Eighty-two patients were identified: 12 males and 70 females with a median age of 86 years. The median Charlson comorbidity index was 6 (interquartile range = 5-7). Eighty-one fractures were classified as lateral compression I or Tile A2, and 1 fracture was classified as lateral compression II or Tile B2. Forty patients were on concurrent anticoagulation treatment. In 4 patients on warfarin, this treatment was reversed on admission.
Results:
The mean hemoglobin (Hb) level on arrival was 12.36 g/dL (±1.67 g/dL). There were significant drops in Hb levels on day 1 (Hb = 11.22 ± 1.86 g/dL, P < .001) and day 4 (Hb = 10.97 ± 1.6 g/dL, P < .001). Nine percent of patients required a blood transfusion. The mean baseline Hb level pre-transfusion was 8.33 g/dL (±1.15). Preexisting anticoagulation treatment did not predispose patients to greater decreases in Hb levels on day 1 (mean difference = 0.16 g/dL, P = .62) or day 4 (mean difference = 0.29 g/dL, P = .48) post-admission.
Discussion:
An observed mean decrease in Hb level of up to 1.4 g/dL can occur in hemodynamically stable elderly patients with osteoporotic pelvic fractures, reflecting an approximate loss of 1.4 units of packed red blood cells.
Conclusion:
This degree of decrease in Hb may be clinically significant in geriatric patients with chronic anemia and a history of cardiovascular disease.
Keywords
Introduction
Low-energy pelvic fracture is common in the elderly 1,2 and is 4 to 6 times more common in women than in men. 3 The incidence of these fractures is expected to increase with the growth in the proportion of the elderly population. 4 -7
The majority of research in this area has, so far, focused on epidemiology, overall outcomes, long-term morbidity, and mortality. 3 However, pelvic fractures are also inherently associated with bleeding risk. 8 At one end of the spectrum, unstable pelvic fractures following a high-energy trauma can be life-threatening. 8,9 On the other end, low-energy pelvic fractures are generally considered as low-risk injuries. 10 Nonetheless, the overall hemorrhage risk associated with a fragility fracture of the pelvis is not well known. Further knowledge in this area may be of value to streamlining of the care of this group of patients.
The primary aim of this study was to estimate the risk of bleeding associated with low-energy pelvic fractures in geriatric patients. We also hypothesized that concurrent anticoagulant medication increases bleeding risk and the need for blood transfusion in elderly patients with pelvic fragility fractures.
Materials and Methods
A retrospective study using data from a single center’s code-based patient database was performed. Institutional review board approval was granted for this study. We identified all patients with a pelvic fracture who were admitted to our institution between January 2015 and July 2018. The inclusion criteria were (1) age
Hospital medical records and patient imaging were reviewed. Information was collected on demographics, associated injuries, the Charlson comorbidity index, 12 anticoagulation treatment, Hb trend during the inpatient stay, need for blood transfusion, length of acute hospital stay, mobility status pre- and post-admission, place of residence before the injury, and discharge destination. All fractures were classified by a fellowship-trained orthopedic consultant according to the classifications of Tile 13 and Young-Burgess. 14 Patients were not routinely asked for a follow-up consultation. Follow-ups were based on social status and patients’ cognitive function.
Statistical Analysis
Statistical analysis was performed using SPSS version 20.0 software (SPSS, Chicago, Illinois). Simple descriptive and frequency analyses were performed on multiple variables. Shapiro–Wilk and Kolmogorov–Smirnov tests were used to test whether the data were normally distributed. Data are presented as medians and interquartile ranges (IQRs) when not normally distributed. Paired-sample t tests were used to compare the means of normally distributed variables. Mann–Whitney tests were used to compare the means of numeric data that were not normally distributed. The χ2 tests were used to test relationships between categorical variables. A P level of <.05 was considered statistically significant.
Results
After the review of medical records, 183 consecutive patients aged 65 years and older were identified. There were 101 patients excluded for the following reasons: no pelvic fracture (miscoded, n = 25), no Hb trend (n = 43), high-energy trauma (n = 13), non-acute fracture (n = 10), acetabular fractures (n = 8), associated tibia fracture (n = 1), and thigh hematoma (n = 1).
The remaining 82 patients met the inclusion criteria and became the focus of this study. There were 70 women and 12 men, with a median age of 86 years (IQR = 81-90 years old). The median Charlson score was 6 (IQR = 5-7). Thirty (37%) patients had cognitive impairment at the time of injury. Sixteen patients sustained associated injuries (Table 1).
Associated Injuries in Patients Presenting With Low Energy Pubic Rami Fracture.

Eighty-one fractures were classified as Lateral Compression I or Tile A2 pelvic fractures. One fracture was classified as Lateral Compression II or Tile B2 (Figure 1). Sixty-one (74%) patients also had pelvis CT-scans at the time of admission, of which 11 (18%) revealed posterior ring injuries. Most of the posterior ring injuries were ipsilateral sacral ala buckle or minimally displaced fractures (n = 10). There was one case of a posterior crescent fracture (Figure 2).

Plain radiograph of an 84-year-old female showing left anterior ring fracture and posterior iliac fracture.

Axial CT scan of the same patient in Figure 1 illustrating the posterior crescent fracture of the ilium.
All patients were hemodynamically stable on arrival and during admission. The mean Hb level on arrival was 12.36 g/dL (±1.67 g/dL). There were significant drops in Hb levels on day 1 (Hb = 11.22 ± 1.86 g/dL, p < 0.001) and day 4 (Hb = 10.97 ±1.6 g/dL, p < 0.001).
At the time of admission, 49% (n = 40) of patients were on concurrent anticoagulation treatment (Table 2). In 4 patients on warfarin, the anticoagulation treatment was reversed on admission. In the remainder of patients, anticoagulation treatment was continued during the inpatient stay. Compared to the rest of the cohort, patients who were given anticoagulation treatment before admission did not have greater reductions in their Hb levels at day 1 (mean difference: 0.16 g/dL, P = .62) or day 4 (mean difference 0.29 g/dL, P = .48). Seven patients required a blood transfusion. The mean baseline Hb before transfusion was 8.33 (±1.15). The mean number of transfused packed red blood cells was 1.1 units.
Concurrent Anticoagulation Treatment in Patients Admitted With Low Energy Pelvic Fracture.

All patients were allowed to mobilize and weight bear, as tolerated with walking aids. The median acute hospital stay was 6 days (IQR = 4-10 days). Table 3 outlines the inpatient complications profile. Nine patients had
Details of Inpatient Complications.

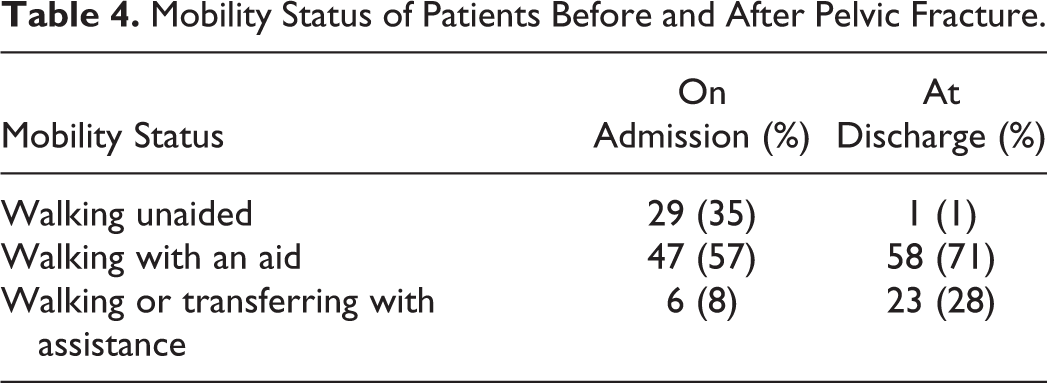
Mobility Status of Patients Before and After Pelvic Fracture.

Bar chart demonstrating the effect of pelvic fragility fracture on discharge destination in geriatric patients.
Discussion
Hemorrhage from cancellous bony surfaces, small caliper veins and muscles is common in patients with pelvic fragility fractures and is generally self-limiting. 15 Although there are a few case reports of life-threatening bleeding from low-energy pelvic fractures in the elderly, 15 -26 to our knowledge, this is the first study that has estimated blood loss in the setting of hemodynamic stability. The mean decrease in Hb level of 1.4 g/dL, corresponding to 1.4 units of a packed red cell, 27 can be expected in patients admitted with low-energy pelvic fractures. This amount of blood loss can be physiologically significant in the subgroup of geriatric patients with preexisting chronic anemia or cardiac comorbidities. 28
Some of the previous case reports indicate that elderly patients with pelvic fragility fractures might develop severe hemorrhage, especially when under anticoagulation therapy. 15,25,29 Nearly half of the patients in this series were receiving anticoagulation therapy at the time of injury, and 90% of them continued their anticoagulation medication during their inpatient stay. Receiving anticoagulation did not increase the bleeding risk associated with a low-energy pelvic fracture in this study cohort.
In this series, the vast majority of patients with osteoporosis-related pelvic fracture had a lateral compression injury that was rotationally stable. A computed tomography scan at the time of admission picked up coexisting posterior ring fractures in 1 in 5 patients. However, we did not find that performing a 3-dimensional imaging study would change the management of these fractures. This is in line with results published in the literature. 30 Conservative treatment consisting of analgesia and as-tolerated weight-bearing remains the mainstay of treatment in geriatric patients with pelvic fragility fracture. 30,31 Operative management is rarely indicated in this setting. 30
Reported incidences of life-threatening situations associated with osteoporotic pelvic fractures reach up to 2.4%. 19,26 However, we did not have to exclude cases of low-energy pelvic fractures with hemodynamic instability in our study. This can be explained by the fact that those rare cases might have been diagnosed early on in the emergency department and transferred to a tertiary referral center for angiography and embolization. Constant diligence and close monitoring are required for the prompt diagnosis of rare cases of hemodynamically unstable pelvic fractures in geriatric patients. 32
Elderly patients with low-energy pelvic fractures utilize substantial health-care resources. 33 The median length of stay in this study (6 days) is shorter than that reported in most previous studies, possibly as a result of the availability of rehabilitation beds and early transfer. 3,7,33,34 The significant negative impact of a pelvic fragility fracture on patients’ mobility, along with immobility-related complications, demands ongoing involvement of geriatricians and allied health services.
There were several weaknesses in the current study. It was a retrospective design, and such studies have certain shortcomings. Estimation of blood loss using the Hb dilution principle has some limitations. 35 It does not take into account gender, weight, and height. It also assumes normovolemic subjects. Although this is a widely used method, 27 it has never been validated. We did not find significantly greater blood loss in patients already on anticoagulation medication. We believe this result should be interpreted with a degree of caution as it can be subject to type II error. Nevertheless, this study determined the potential bleeding risks associated with a pelvic fracture in a reasonably sized cohort of geriatric patients in a general metropolitan hospital. This represents a realistic clinical environment, which is likely to exist in many institutions. To our knowledge, this is the first study in the English-language literature to estimate the hemorrhage risk associated with a low-energy pelvic fracture in the elderly population.
Conclusions
In a hemodynamically stable elderly population with fragility fractures of the pelvis, an average decrease in Hb level of 1.4 g/dL, corresponding to 1.4 units of packed red blood cells, can be expected. Concurrent anticoagulation therapy does not necessarily increase bleeding risk in this setting. This magnitude of the decline in Hb levels may be physiologically important in geriatric patients with preexisting chronic anemia or poor cardiovascular reserves.
Footnotes
Acknowledgment
The authors want to thank Vicky Kartsogiannis for administrative assistance.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.