
Abstract
Objectives:
To report the incidence and risk factors for prolonged hospitalization, discharge to a facility, and postoperative complications in geriatric patients who underwent surgery for patella fracture.
Design:
Retrospective database review.
Setting:
The American College of Surgeons—National Surgical Quality Improvement Program (NSQIP) collects data from 600 hospitals across the United States.
Patients/Participants:
NSQIP patients over 65 years of age with patella fractures.
Intervention:
Surgical fixation of patella fracture including extensor mechanism repair.
Main Outcome Measurements:
Prolonged hospitalization, discharge to a facility, and 30-day post-operative complications.
Results:
1721 patients were included in the study. The average age was 74.9 years. 358 (20.8%) patients were male. 122 (7.1%) patients had a length of stay greater than 7 days. Factors associated with prolonged length of stay include pre-existing renal failure, need for emergent surgery, and time to surgery greater than 24 hours from admission. 640 patients (37.2%) of patients were discharged to a facility after surgery. Discharge to facility was associated with age >77 years, obesity, anemia, thrombocytopenia, pre-operative SIRS, and CCI > 0.5. Admission from home decreased the odds of discharge to a facility. The most common postoperative complications in this population were unplanned readmission (3.4%), unplanned reoperation (2.7%), surgical site infection (1.1%), mortality (1.0%), venous thromboembolism (0.8%), and wound dehiscence (0.2%). Complication rates increased with anemia and ASA class IV-V.
Conclusions:
Geriatric patients undergoing operative intervention for patella fractures are at high risk for prolonged hospitalization, discharge to facility, unplanned readmission or reoperation, and surgical site complications in the first 30 days following surgery. This study highlights modifiable and non-modifiable risk factors associated with adverse events. Early recognition of these factors can allow for close monitoring and multidisciplinary intervention in the perioperative period to improve outcomes.
Level of Evidence:
Prognostic level III.
Keywords
Introduction
The incidence of patella fractures is reported to be 1.2 to 6.1 per 100,000 person-years. 1,2 Younger patients typically sustain patella fractures during high energy trauma or eccentric muscle contraction, while older patients are more susceptible to low energy mechanisms commonly referred to as fragility fractures. 2,3 Prior studies report that the incidence of patellar fragility fractures in geriatric patients is 13.1/100,000 person-years. 1 This represents a significant cause of morbidity that will likely increase with the aging population.
Although some patella fractures can be treated non-operatively, surgical intervention is indicated when the extensor mechanism is disrupted or there is an articular step-off greater than 2 mm. 4 A wide variety of surgical constructs have been implemented including open reduction internal fixation with screws, plate fixation, tension band construct, and extensor mechanism repair in the setting of a small, irreparable bone fragment. 1,2 Prior studies stress the importance of operative fixation of patella fractures in order to produce optimal functional outcomes, particularly in the geriatric population. 5 Shabat et al looked specifically at function after geriatric patella fractures and found that 91% of patients treated operatively returned to their pre-injury mobility status, whereas only 50% of patients treated non-operatively achieved the same functional results. 5 This is particularly important in geriatric patients who may have difficulty with mobility prior to their injury. Although previous studies have addressed functional results and mortality after patella fracture repair in geriatric patients, there is a paucity of research examining early postoperative complications and factors that predispose patients to poor outcomes. 5,6
The primary aim of this study was to report the length of stay, discharge location, and rate of 30-day post-operative complications and mortality in geriatric patients who underwent operative intervention for patella fractures. The secondary aim was to identify patient factors associated with an increased rate of adverse events.
Methods
Study Design
This study uses de-identified data and was exempt from Institutional Review Board review. The American College of Surgeons-National Surgical Quality Improvement Program (NSQIP) is a national surgical registry that prospectively collects 30-day perioperative data from more than 600 sites across the United States. The data collection and quality control methodologies for NSQIP have been previously described and shown to be reliable. 7,8
Patient Selection and Exclusion Criteria
International Classification of Diseases, 9th (ICD-9) and 10th (ICD-10) diagnostic codes 822.0, 822.1, and S82.0-S82.099 were used to identify patients with patella fractures. Current Procedural Terminology (CPT) codes indicating patella fracture open-reduction internal fixation (ORIF) or extensor mechanism repair were used to complete the initial cohort. Between 2005 and 2018, 4,941 patella fractures were identified. Patients under age 65 and those with multiple injuries, periprosthetic, osteochondral, open, and pathologic fractures, or undergoing revision surgery due to hardware failure or malunion were excluded. The final cohort included 1,721 patients (Figure 1).

Flow Diagram of Study Population Selection.
Patient Variables and Outcomes
Patient demographics such as age, sex, smoking history, and pre-operative functional status are reported in the NSQIP database. Pre-operative function is defined by NSQIP as a patient’s peak level of function in activities of daily living during the 30-days prior to admission. Charlson Comorbidity Index (CCI) was calculated for each patient using available information as detailed in prior publications. 9 Other perioperative variables such as time from admission to surgery, need for emergent surgery, duration of stay, and American Society of Anesthesiologists (ASA) classification were included in the analysis. For the purposes of this study, need for emergent surgery is defined by NSQIP at a case where the patient’s well-being or postoperative outcome is threatened by delay in treatment.
There were 3 outcomes of interest in this study: (1) hospital stay greater than 7 days, (2) discharge to a facility after operative intervention, and (3) one or more complications within the 30-day post-operative period. Complications included surgical site infection or dehiscence, venous thromboembolism, unplanned readmission, unplanned reoperation, and death.
Statistical Analysis
Patient factors were reported using descriptive statistics. Continuous variables were reported using average and standard deviation (SD), while categorical variables were described using frequency and percentage. Bivariate comparisons between continuous variables were performed using Student t test or Mann-Whitney U test when appropriate, and categorical variables were compared using contingency table analyses such as χ2 test of independence. Potential factors related to the outcomes of interest were evaluated using multivariate logistic regression models. Variable selection was performed using stepwise regression with forward and backward selection. The selected variables were then assessed for significant collinearity which was defined as a variation inflation factor coefficient of 5.0 or greater. Adjusted odds ratios (aOR) and 95% confidence intervals (CI) were determined using the β coefficients from the logistic regression. In order to calculate odds ratios for numerical factors, ideal cutoff values were calculated by receiver operating characteristic (ROC) curve analysis to convert continuous variables to categorical variables. The α value was set at 0.05 as the threshold for statistical significance. All statistical analysis was performed using the statistics programming language R version 3.5.1 (Vienna, Austria). 10
Results
Patient Characteristics
One thousand seven hundred twenty-one patients were included in this study. The population was composed of 79.2% (1363) females and 20.8% (358) males with an average age of 74.9 (SD 8.1) years, and average body-mass index (BMI) of 27.9 (SD 6.2) kg/m2. Most patients were admitted from home (92.0%) and functionally independent (92.0%) (Table 1). Hypertension was the most common comorbidity (61.2%) followed by diabetes (23.2%), end stage renal failure (15.9%), and impaired coagulation (7.0%). The average CCI was 0.3 (SD 0.6) (Table 2). Eighty-five patients (4.9%) were ASA class IV or V. Two hundred eighty-eight (16.7%) cases were designated as requiring emergent surgery, and the average time from admission to surgery was 0.9 (SD 8.8) days (Table 3).
Characteristics of Patients Treated for Non-periprosthetic Patella Fractures.
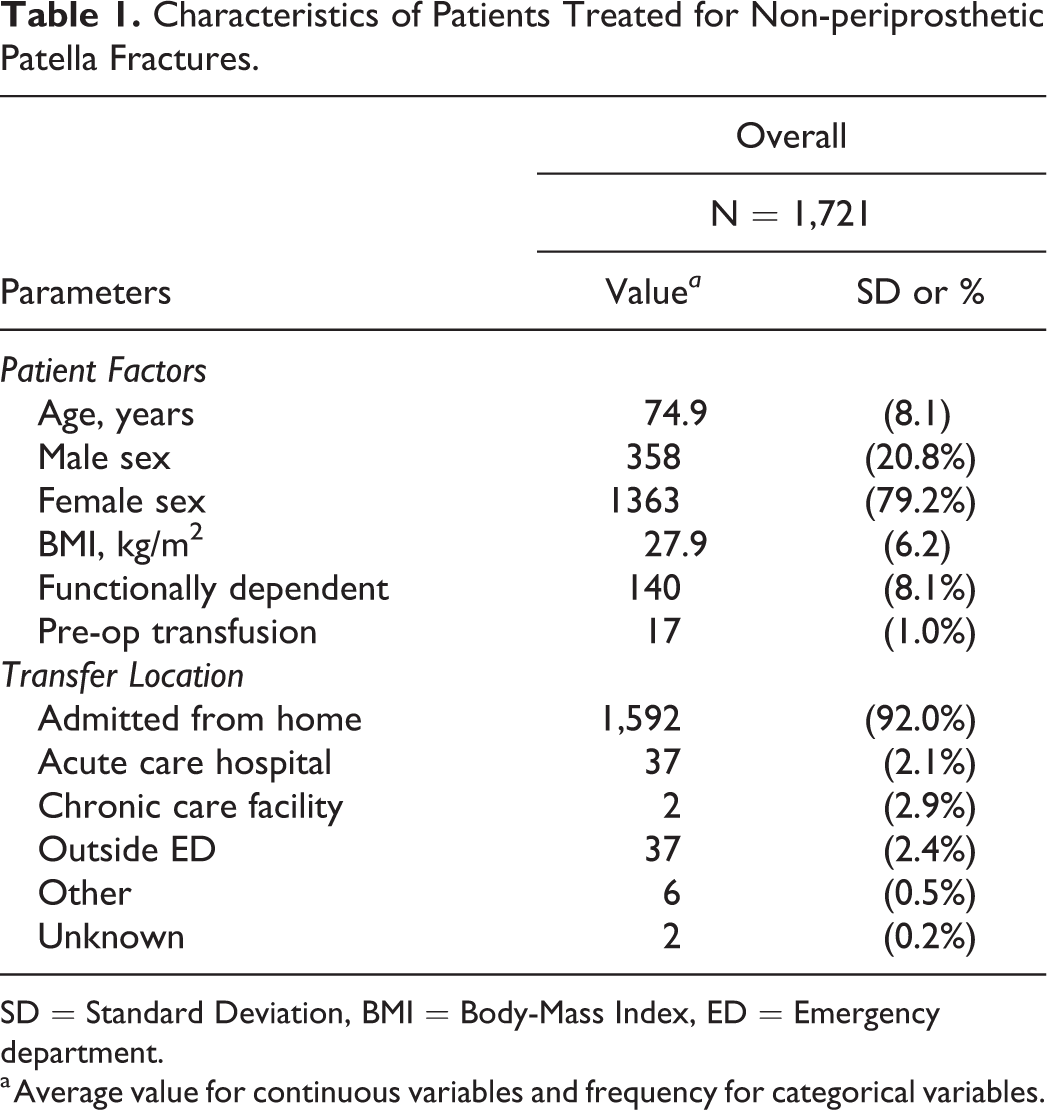
SD = Standard Deviation, BMI = Body-Mass Index, ED = Emergency department.
a Average value for continuous variables and frequency for categorical variables.
Pre-Operative Laboratory Values and Comorbidities.

SD = Standard Deviation, BUN = Blood Urea Nitrogen, WBC = White Blood Cell Count, HCT = Hematocrit, CHF = Congestive Heart Failure, SIRS = Systemic Inflammatory Response Syndrome, COPD = Chronic Obstructive Pulmonary Disease, CKD = Chronic Kidney Disease, CCI = Charlson Comorbidity Index.
Operative Characteristics and Post-Operative Outcomes.
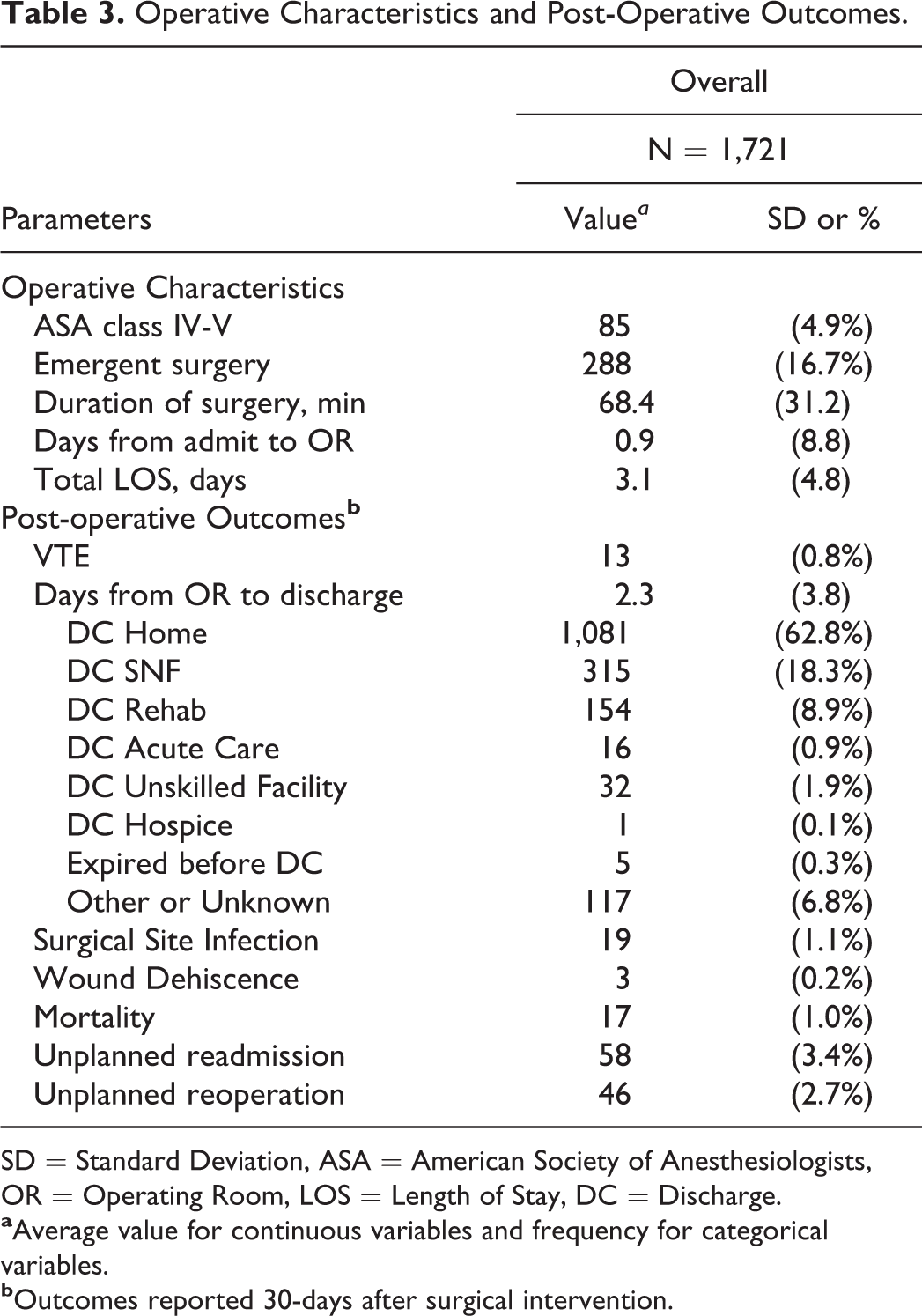
SD = Standard Deviation, ASA = American Society of Anesthesiologists, OR = Operating Room, LOS = Length of Stay, DC = Discharge.
Length of Stay
The average length of stay (LOS) was 3.1 (4.8) days. One hundred twenty-two (7.1%) patients had a length of stay greater than 7 days. Length of stay greater than 7 days was of particular interest as Medicare does not consider open reduction internal fixation of patella fractures to be an inpatient only procedure allowing for day surgery. Similarly in a study by Nikkel et al looking at 180,844 patients with hip fractures, the average length of stay was 5.6 in 2011. 11 Patients with renal failure requiring dialysis (aOR 14.5, 95% CI 2.55-90.4), emergent surgery (aOR 2.82, 95% CI 1.16-6.61), or time from admission to surgery >24 hours (aOR 14.6, 95% CI 6.67-34.3) had a statistically independent increased odds of LOS greater than 7 days. No factors were significantly associated with decreased odds of prolonged hospitalization (Table 4).
Adjusted Odds Ratios for Hospital Length of Stay >7 Days After Treatment of Patella Fractures in Geriatric Population.

aOR = Adjusted Odds Ratio; CI = Confidence Interval; SIRS = Systemic Inflammatory Response Syndrome; ASA = American Society of Anesthesiologists.
Discharge to a Facility
Six hundred forty (37.2%) were discharged to a facility after surgery. Age >77 years (aOR 2.89, 95% CI 2.21-3.79), BMI >30 kg/m2 (aOR 1.42, 95% CI 1.06 - 1.89), hematocrit <35% (aOR 2.27, 95% CI 1.73-2.97), platelet count <217,000/mL (aOR 1.39, 95% CI 1.08 -1.80), and presence of pre-operative systemic inflammatory response syndrome (SIRS) criteria/sepsis (aOR 2.36, 95% CI 1.16-4.91), and CCI >0.5 (aOR 1.67, 95% CI 1.26 - 2.21) were identified as statistically independent factors associated with discharge to a facility after surgery. Admission from home was associated with a statistically independent decreased odds of discharge to a facility (aOR 0.52, 95% CI 0.33 - 0.83) (Table 5).
Adjusted Odds Ratios for Discharge to Facility After Treatment of Patella Fractures in Geriatric Population.

aOR = Adjusted Odds Ratio; CI = Confidence Interval; BMI = Body-Mass Index; BUN = Blood Urea Nitrogen; SIRS = Systemic Inflammatory Response Syndrome; CKD = Chronic Kidney Disease; ASA = American Society of Anesthesiologists.
Postoperative Complications
The most common postoperative complications were unplanned readmission (3.4%), unplanned reoperation (2.7%), surgical site infection (1.1%), mortality (1.0%), thromboembolic events (0.8%), and wound dehiscence (0.3%) (Table 3). Statistically independent factors associated with post-operative complications were hematocrit <34% (aOR 2.14, 95% CI 1.26-3.59) and ASA class IV-V (aOR 2.58, 95% CI 1.13-5.50) (Table 6).
Adjusted Odds Ratios for Surgical Site Complications, Venous Thromboembolism, Reoperation, and Readmission After Treatment of Patella Fractures in Geriatric Population.

aOR = Adjusted Odds Ratio; CI = Confidence Interval; BMI = Body-Mass Index; CHF = Congestive Heart Failure; ASA = American Society of Anesthesiologists, WBC = White Blood Cell.
Discussion
Geriatric patients undergoing operative intervention for patella fractures are at high risk for prolonged hospital stay, discharge to a facility, surgical site complications, unplanned readmission, unplanned reoperation, and mortality in the first 30 days following surgery. Factors associated with prolonged hospitalization include pre-existing renal failure, need for emergent surgery, and time to surgery >24 hours from admission. Discharge to a facility was associated with advanced age (>77 years), obesity, anemia, thrombocytopenia, presence of pre-operative SIRS (whether due to trauma or underlying infection), and CCI > 0.5. Risk of post-operative complications increased with anemia and ASA class IV-V.
Complications after operative treatment of patella fractures is something that has been previously examined due to the relatively superficial anatomic location of the patella and the frequency of symptomatic hardware. Although the study was not limited to the geriatric population, a meta-analysis by Dy et al. found that the estimated rate of re-operative was 33.6%, infection 3.2%, and non-union 1.9%. 1 It is important to note that in this study there was no significant difference in risk found in age, gender, or operative technique, so these are not complications limited to geriatric patients. 1 In another study looking at geriatric patella fractures, by Matthews et al. it was found that age >65 and comminuted fracture patterns were risk factors for failure of fixation and leading to repeat operative intervention. 12 Due to the nature of our database study, however, fracture type was unable to be ascertained and so the implications of this on our study population cannot be determined.
Other Risk factors identified in this study can be divided into modifiable and non-modifiable risk factors. Delayed surgical intervention is a potentially modifiable risk factor associated with total length of stay greater than 7 days. Prolonged hospitalization increases the risk of exposure to nosocomial infections that can lead to serious complications or the need for revision surgery. Furthermore, each additional day in the hospital increases the financial burden incurred by the patient and the healthcare system. The association between delayed intervention and prolonged hospitalization has been observed in other orthopedic studies. A 2015 paper by Ricci et al considered geriatric patients with hip fractures and found that day of admission, comorbidities, ASA class, and the need for cardiac clearance led to delays to the OR, which ultimately resulted in an increased length of stay. 13 Despite optimization of preoperative factors and prolonged hospitalization, a 2018 study by Mitchell et al showed that there was no statistically significant difference in post-operative outcomes of geriatric hip fracture patients with delayed surgery. 14 Patella fractures appear to have a similar association between delayed surgery and prolonged hospitalization.
Non-modifiable risk factors such as advanced age, obesity, pre-operative SIRS, anemia, and ASA class were associated with poor outcomes. Advanced age increases both the risk for fractures and the risk for postoperative complications. One large population study in Japan found that for orthopaedic patients >80 years of age, mortality and major post-operative complications had an odds ratio of 5.88 and 1.51 respectively. 15 Another study by Fang et al 2015 looked specifically at age and its effect on post-operative outcomes after total joint replacement. 16 They found that length of stay, discharge to a skilled nursing facility, and post-operative complication rates all increased with age. 16
There has been much research on the effects of obesity on complications after orthopedic surgery. Many studies identify an increased risk of surgical site infections, particularly in joint and spine surgeries, which we did not find in our population. 17 -20 We did determine that obesity, or BMI > 30, increased the likelihood for discharge to a facility, consistent with other studies looking at obesity and orthopedic trauma patients. 21 -23
Anemia was associated with an increased risk of post-operative complications and discharge to a facility. Preoperative anemia has been shown to increase the risk of poor postoperative outcomes in prior studies. 24 -26 Up to one-third of anemia cases in the elderly are associated with malnutrition, especially in the context of a low BMI. 26 However, the etiology of anemia in NSQIP patients is unclear and may represent other factors such as polypharmacy and myelodysplasia, limiting the analysis.
Patients who met SIRS criteria during the pre-operative period were more likely to be discharged to a facility. We are unable to determine if the patients with SIRS ended up having an identifiable source, thereby meeting sepsis criteria, or if the SIRS was simply a response to trauma. Studies have been conducted to elucidate the inflammatory response after trauma and the “two-hit” phenomenon, where there is an initial traumatic event followed by physiologic derangements and operative intervention. 27 The effects of the “two-hit” phenomenon can be even more profound in the geriatric population. These patients have a decreased physiologic reserve and may have a more significant inflammatory response to trauma, even with relatively small injuries. 28,29
CCI and ASA classification are both used to stratify patient risk prior to surgery. Our study showed that increased CCI is associated with an in increased risk for discharge to a facility and ASA class IV or V also increased the risk of post-operative complications. Prior studies have shown that ASA is the strongest predictor of length of stay for orthopedic fracture patients. 30 However, research such as Lakomkin et al found that increased CCI is associated with increased length of stay in orthopedic trauma patients, and Voskuijl et al showed that every point increase in CCI was associated with an additional 0.63% risk for readmission in orthopedic trauma patients. 31,32 Although different studies focus on different outcomes associated with CCI and ASA, both metrics are associated with adverse postoperative outcomes.
The non-modifiable variables discussed above have been described in the geriatric literature as components of the frailty index. 33 The frailty index uses comorbidities, activity level, and functional status to estimate a patient’s physiologic reserve and ability to tolerate surgery and their risk of post-operative morbidity and mortality. 34,35 Many definitions of frailty also include nutrition variables such as albumin, hematocrit, BMI, and weight loss. 36,37 Recent studies in geriatric trauma found that the frailty index was an independent predictor of in-hospital complications and adverse discharge disposition, superior to that of age alone. 38 Despite the importance of frailty and malnutrition in geriatric surgery, these clinical states are difficult to assess using the variables available in NSQIP. Several components of malnutrition and frailty assessments are captured including functional status, medical comorbidities, anemia, BMI, and unintentional weight loss. Unfortunately, other important variables such as mental status, psychological comorbidities, activity level, and gait speed are not recorded, limiting the ability to use an existing malnutrition or frailty assessment tool.
Limitations
The current study has several limitations worth noting. The retrospective design introduces the possibility of selection bias. Additionally, NSQIP is a general surgery database which was not specifically designed for geriatric or orthopaedic trauma-related research. As such, many important variables such as fracture pattern and immediate post-operative mobility are not documented. Although the CCI was utilized in this study, it is important to note the limitations of the index in the context of the NSQIP database. Certain variables may have been reported inconsistently leading to possible changes to CCI. Many of the non-modifiable risk factors identified in this study such as age, anemia, and ASA class are described as components of the frailty index. 33,39,40 However, NSQIP fails to capture many datapoints related to frailty, which is important to assess in a geriatric population. Further study is needed to identify and validate NSQIP definitions of frailty that can be used to assess the impact of this on postoperative outcomes in geriatric orthopaedic surgery.
Finally, the 30-day follow-up period limits the comparability of the results of this study with those that evaluate outcomes beyond the first postoperative month.
Conclusion
The incidence of patella fractures is expected to increase with the aging population representing a potential source of morbidity and mortality in geriatric orthopaedic surgery. This study demonstrates several modifiable and non-modifiable risk factors associated with prolonged hospital stay, discharge to a facility, and postoperative complications. For the surgeon, prompt surgical intervention may decrease the total length of stay, yet efforts to optimize time to surgery may be limited by the fitness of the patient in this complex population. It is important that note that while there are risks and complications that can occur with operative treatment of patella fractures in a geriatric population, the functional benefits of treatment may out way most of the risks. Similarly, due to the significant impact on mobility, non-operatively treated patella fractures in this same population may also have similar complications coupled with decreased function which can be an area of further research. 5 Overall, frailty and its associated factors can be difficult to identify and optimize prior to surgery, particularly in the trauma setting, due to the multivariate nature and the inability to exact immediate change. However, recognition and risk stratification permit close monitoring and multidisciplinary intervention in the postoperative period.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.