
Abstract
Background:
Little is known about the effect of preinjury residence on inpatient mortality following hip fracture. This study addressed whether (1) admission from a nursing home residence and (2) admission from another hospital were associated with higher inpatient mortality after a hip fracture.
Methods:
Using the National Hospital Discharge Survey database, we analyzed an estimated 2 124 388 hip fractures discharges, from 2001 to 2007. Multivariable logistic regression analysis was performed to identify whether admission from a nursing home and admission from another hospital were independent risk factors for inpatient mortality. Our primary null hypothesis is that there is no difference in inpatient mortality rates after hip fracture in patients admitted from a nursing home, compared to other forms of admission. The secondary null hypothesis is that there is no difference in inpatient mortality after hip fracture in patients whose source of admission was another hospital, compared to other sources of admission.
Results:
Almost 4% of the patients were admitted from a nursing home and 6% from another hospital. The mean age was 79 years and 71% were women. The majority of patients were treated with internal fixation. Admission from a nursing home residence (odds ratio [OR] of 2.1, confidence interval [CI] 1.9-2.3) and prior hospital stay (OR 3.4, CI 3.2-3.7) were associated with a higher risk of inpatient mortality after accounting for other comorbidities and type of treatment.
Conclusions:
Patients transferred to an acute care hospital from a long-term care facility or another acute care hospital are at particularly high risk of inpatient death. This subset of patients should be considered separately from patients admitted from other sources.
Level of Evidence:
Prognostic level II.
Introduction
Hip fractures are prevalent in the geriatric population and are associated with increased utilization of health care resources and high rates of mortality and disability. 1 –3 Hip fracture risk increases exponentially with age 4 and the number of fractures and their associated expenditure is projected to increase 3- to 8-fold in the next 20 years. 5,6
Most nursing home residents are older adults with multiple medical conditions that have trouble living independently. 7 Previous research showed that the risk of hip fracture in nursing home residents 3,8 –10 is at least 2 to 3 times higher than in community dwellers of the same age and sex. 2 This higher incidence may partly be explained by a higher number of falls in institutionalized elderly patients. 11 An Australian study 12 of 666 patients compared mortality rates in patients with hip fractures who were nursing home residents at the time of the injury to community dwellers and concluded that nursing home residence conferred greater odds of mortality in the postinjury period. 12 On the other hand, a study conducted by Poor and colleagues 13 concluded that residential status prior to sustaining a hip fracture was not a predictor for increased in-hospital mortality. However, this study was conducted in 1989 (study time period 1978-1989) with a cohort of only 131 patients. 13
This study addressed whether (1) preinjury source of admission from a nursing home residence and (2) admission from another hospital were associated with higher inpatient mortality after a hip fracture.
Methods
Data for this study were obtained from the National Hospital Discharge Survey (NHDS) database. 14 The NHDS is a national probability survey conducted by the National Center for Health Statistics (NCHS), Centers for Disease Control and Prevention and collects annually medical and demographic information since 1965. 14 The data are collected from inpatients discharge records from more than 500 general and children’s hospitals in the United States, excluding exclusive federal, military, and Veterans Administrations hospitals. All of the hospitals were nonfederal and short stay (less than 30 days on average) or with a general specialty, and the hospitals had 6 or more beds staffed for patient use.
Medical information was based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) of the NHDS database. 15,16 The deidentified NHDS data are free and available online. Therefore, no institutional review board approval was necessary for this study.
Baseline Statistics.
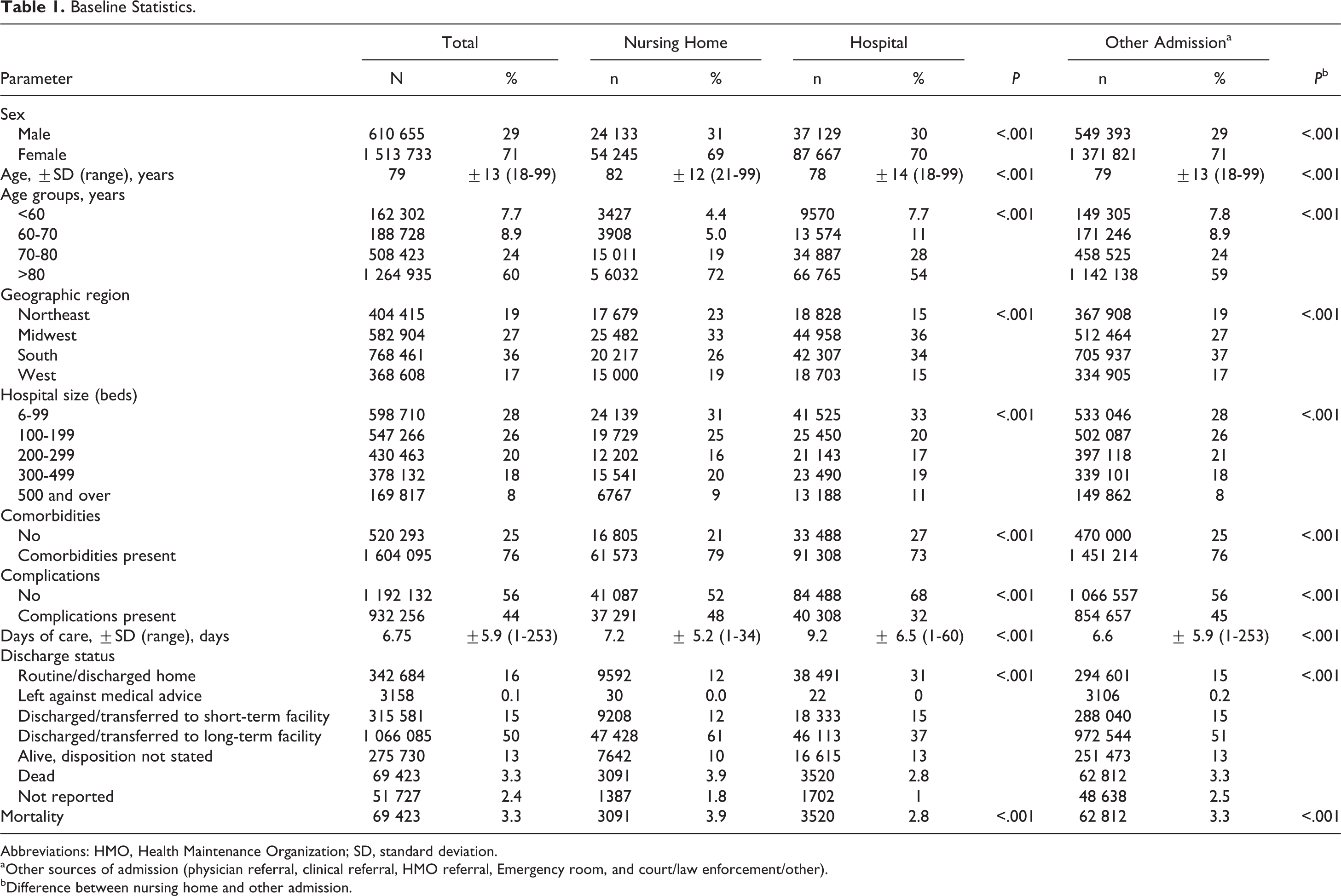
Abbreviations: HMO, Health Maintenance Organization; SD, standard deviation.
aOther sources of admission (physician referral, clinical referral, HMO referral, Emergency room, and court/law enforcement/other).
bDifference between nursing home and other admission.
We divided the patients into 3 groups, based on their source of admission: admission from a nursing home, admission from a hospital, and a rest group including all other sources of admission (physician referral, clinical referral, Health Maintenance Organization referral, emergency department [ED], and court/law enforcement).
Comorbidities.

Abbreviation: HMO, Health Maintenance Organization.
aOther sources of admission (physician referral, clinical referral, HMO referral, emergency department, and court/law enforcement/other).
bDifference between nursing home and other admission.
Additional Injuries.
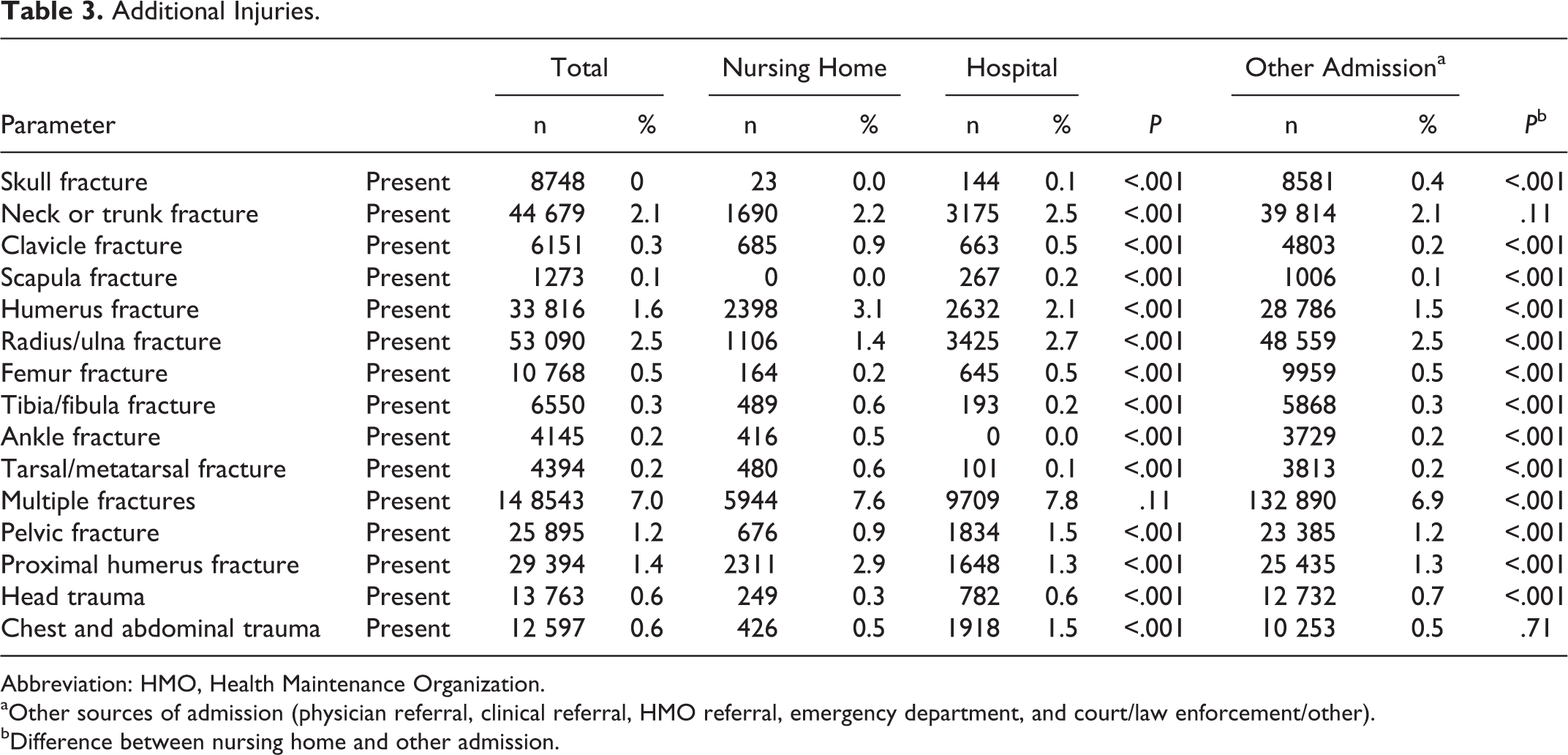
Abbreviation: HMO, Health Maintenance Organization.
aOther sources of admission (physician referral, clinical referral, HMO referral, emergency department, and court/law enforcement/other).
bDifference between nursing home and other admission.
Treatment and Complications.

Abbreviation: HMO, Health Maintenance Organization.
aOther sources of admission (physician referral, clinical referral, HMO referral, emergency department, and court/law enforcement/other)
bDifference between nursing home and other admission
We reported means and standard deviations of continuous baseline variables. Frequencies and percentages were used for baseline categorical variables and presence of comorbidities or complications in baseline, comorbidities for the entire cohort.
Based on the sample size, we assumed normality of the data. We compared patients admitted from a nursing home with patients admitted from another hospital (comparison 1) and patients admitted from a nursing home with patients admitted from other sources (comparison 2). We used independent samples t test for both comparisons for continuous outcomes and chi-square test (or Fisher exact test when applicable) for categorical parameters.
In order to find whether admission from a nursing home was an independent risk factor for death when corrected for confounders, we entered all variables that were significantly (P < .001) different in bivariate analysis and were present in at least 2% of the population 17 in a backward likelihood ratio multivariable logistic regression.
Results
The cohort consisted of an estimated number of 2 124 388 patients. Seventy-one percent were female, and the mean age was 79 years (range 18-99). Nearly 4% of the patients were admitted from a nursing home and 6% from a hospital (Table 1).
Patients admitted from a nursing home were older and had fewer days of inpatient care compared to patients admitted from a hospital, but more days of care compared to patients admitted from another source.
The inpatient mortality rate was 3.3% in the total cohort, but the inpatient mortality of patients admitted from a nursing home (3.9%) was significantly greater than for patients transferred from a hospital (P < .001) or another source (P < .001; Table 1).
Comorbidities were present in 76% of the patients with a hip fracture. Patients admitted from a nursing home had significantly more comorbidities than patients admitted from another hospital (P < .001) and from another source (P < .001; Table 2).
Patients admitted from another hospital had significantly more additional injuries compared to patients admitted from another hospital or patients admitted from other sources (Table 3).
Most of the patients with a hip fracture were surgically treated with internal fixation (54%) or prosthetic arthroplasty (32%). The remainder 14% had nonoperative treatment of the hip fracture. Patients admitted from a nursing home had more adverse events compared to patients transferred from a hospital or other source of admission. Transfusion and acute postoperative anemia were the most common adverse events in all 3 groups. Patients from a nursing home also had more acute renal failure, pulmonary embolism, and inducedmental disorder, acquired during the admission compared to both the patients admitted from another hospital and the patients with other sources of admission.
Admission from a nursing home (β = 0.74, P < .001, odds ratio [OR] 2.1, confidence interval [CI] 1.9-2.3) or from a hospital resulted in an increased risk of death (β = 1.2, P < .001, OR 3.4, CI 3.2-3.7), when controlling for demographics, comorbidities, treatment, and adverse events (model fit: Omnibus test of model coefficients: chi-square = 511 943, P < .001, Nagelkerke R 2 = 0.86).
Both internal fixation (β = −1.7, P < .001, OR 0.18, CI 0.18-0.19) and prosthetic arthroplasty (β = −1.5, P < .001, OR 0.23, CI 0.22-0.24) were associated with decreased risk of inpatient mortality in comparison to nonoperative treatment.
Logistic Regression for Predictors of Mortality After Hip Fractures.a
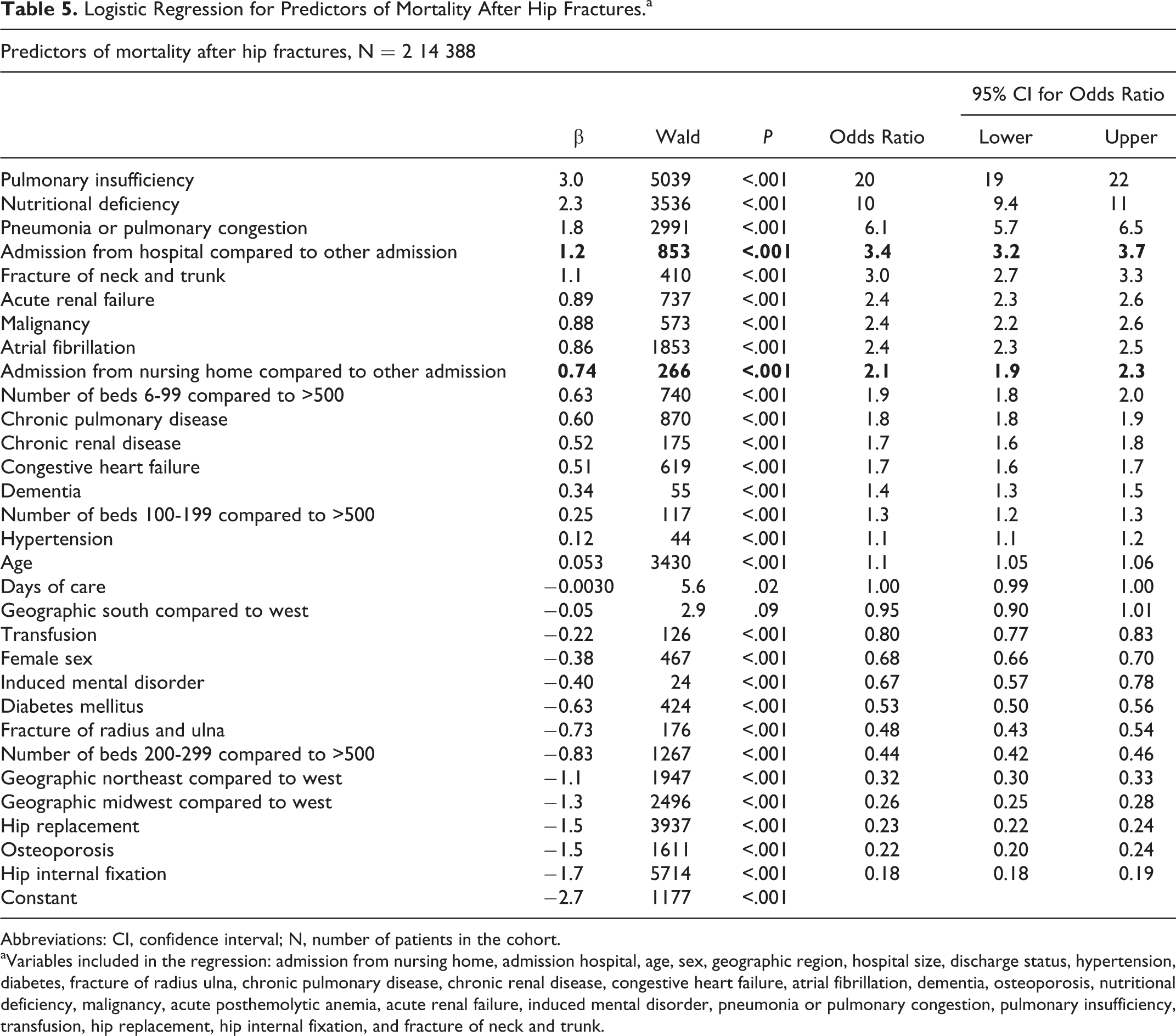
Abbreviations: CI, confidence interval; N, number of patients in the cohort.
aVariables included in the regression: admission from nursing home, admission hospital, age, sex, geographic region, hospital size, discharge status, hypertension, diabetes, fracture of radius ulna, chronic pulmonary disease, chronic renal disease, congestive heart failure, atrial fibrillation, dementia, osteoporosis, nutritional deficiency, malignancy, acute posthemolytic anemia, acute renal failure, induced mental disorder, pneumonia or pulmonary congestion, pulmonary insufficiency, transfusion, hip replacement, hip internal fixation, and fracture of neck and trunk.
Discussion
A considerable number of patients sustaining a hip fracture are admitted from either a nursing home or another acute care hospital, but the influence of preinjury residency on in-hospital outcomes is incompletely understood. Given the growing geriatric population and corresponding rise in the independent nursing home market, 18 there is interest in addressing the impact of preoperative residential status on inpatient mortality following hip fractures. 19 –22 This study addressed whether (1) admission from a nursing home residence and (2) admission from another hospital were associated with higher mortality after a hip fracture.
The present study has several limitations associated with the utilization of administrative databases. 23 First, ICD-9 codes were used to retrieve hip fracture discharges, as well as the correspondent treatment and subsequent adverse events. Because of the extensive sample size of our study, we cannot exclude the possibility of misclassification of the codes—as provided by the NHDS—examined in this study. Miscoding could potentially lead to an under- or overestimation of the importance of risk factors. 15 Nonetheless, misclassification errors take place in similar frequency in all comparison groups in large-scale studies. 24 There is an assumption that the database codes “transfer from nursing home” will be applied whether or not the patient goes through the ED. Second, this study was limited to inpatient outcomes after hip fracture; therefore, information regarding complications and mortality rates following hospital discharge, as well as readmission rates due to an adverse event, remains undetected. In addition, the NHDS does not measure functional status, which is another limitation.
The influence of hospital size to mortality stays unclear, hospitals up to 200 beds compared with >500 increase the risk of mortality, while hospitals with 200 to 300 beds compared with >500 beds decrease the risk of inpatient mortality.
The percentage of patients with dementia (3.3%) in the group of patients admitted from a nursing home seems relatively low, this could be underreported. Therefore, the only conclusions that can be drawn from this study are those concerning inpatient mortality.
Our finding that hip replacement or internal fixation is associated with a lower risk of mortality compared to nonoperative treatment is likely due to the fact that nonoperative treatment corresponded with end-of-life care, but it was not possible to determine this from the database. The present study indicates that hip fracture-related mortality rates were significantly higher among patients admitted to US hospitals from nursing homes compared to a non-nursing home preinjury residential status. The overall mortality rate was 3.3% for the entire study cohort, which is consistent with the findings of Bhattacharyya et al, 15 who noted a 3.1% inpatient mortality rate for patients treated for a hip fracture between 1995 and 1997. Particularly, the baseline mortality rate for patients admitted from a nursing home was 3.9%, compared to 3.3% and 2.8% mortality rates for patients admitted from other sources (ie, from home) or from a hospital, respectively.
In a study conducted by Roche et al, 25 13% of all patients admitted to hospital with a hip fracture between 1999 and 2003 were nursing home residents. A recent study from Neuman et al 26 found an 8.3% of patients admitted from a long-term nursing home among patients with a hip fracture. The overall percentage of hospitalized patients admitted from a nursing home in our study was nearly 4%. This difference in the percentage of nursing home residents admitted to hospital might be explained because the aforementioned authors excluded patients aged less than 60 years old, while we did not (which formed 7.6% of our cohort). Admission from a nursing home was deemed an independent risk factor for in-hospital death in our 7-year cohort. A prior hospital stay in another facility immediately before hospital admission for the hip fracture was also associated with an increased risk of inpatient death, and this risk was higher than that of patients admitted from nursing homes.
In conclusion, a source of hospital admission other than home prior to sustaining a hip fracture was found to be a reliable predictor for increased inpatient mortality while controlling for other factors, such as comorbidities, sex, and age. Therefore, preinjury residential status, including not only admissions from a nursing home but also from other hospitals, should be taken into account when assessing outcomes following hip fractures. Patients transferred to an acute care hospital from a long-term care facility or another acute care hospital are at higher risk of inpatient death. This subset of patients should be considered separately from patients admitted from other sources.
Footnotes
Authors’ Note
This study was approved by the institutional review board of the Massachusetts General Hospital. The IRB reviewed our protocol and decided that this study was exempt from IRB approval because we worked with deidentified data. The study was performed at the Orthopaedic Hand and Upper Extremity Service, Massachusetts General Hospital, Boston, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Arjan G.J. Bot: “AnnaFonds Travel grant” (Dutch Orthopaedic travel grant); “VSB-fonds” a nonmedical study grant; “Prins Bernhard Cultuurfonds, Banning-de Jong fonds” a nonmedical study grant for excellent Dutch students. Valentin Neuhaus: Gottfried und Julia Bangerter-Rhyner-Stiftung, Switzerland. David Ring: Consultant, Wright Medical, Skeletal Dynamics, and Biomet. Mark E. Vrahas: Expert testimony: Law firms, no current, Stock options: Dividends; Travel/accommodations/meeting expenses unrelated to activities listed: CME teaching. David Ring: Study Specific Grants; Skeletal Dynamics (pending); Honoraria: AO North America, AO International; Royalties Received: Wright Medical; Royalties Contracted; Biomet: Skeletal Dynamics; Stock Options: Illuminos. Mark E. Vrahas: Grants: Aona: OREF: NIH; Funding for Hand Surgery Fellowship: AO North America.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.