
Abstract
Introduction
Lumbar discectomy is a common and effective treatment for symptomatic disk herniation. It has been suggested that lumbar discectomy in older patients may result in poorer clinical outcomes and lesser satisfaction. The purpose of this study was to assess age-related difference in patient reported outcomes of patients undergoing lumbar discectomy for chronic low back and radicular pain.
Materials and methods
Patients with chronic lumbar radiculopathy without neurological deficit underwent non-urgent single level lumbar discectomy in our institution between 2014 and 2017. Pain level (using VAS score), Oswestry Disability Index, and SF-12 scores were retrospectively reviewed and compared between younger patients (<60 years, group 1) and older patients (>60 years, group 2).
Results
Seventy-three patients, aged between 34–76 years participated in this study. VAS, ODI, and SF-12 scores improved significantly after the surgery for each group (P < .01). When comparing between the groups, no significant differences in the outcomes measured were found after the surgery in both early post-operative follow-up and late post-operative follow-up (P > .05).
Discussion
Elderly patients undergoing lumbar discectomy report a significant reduction in VAS, ODI, and SF-12 scores justifying the procedure.
Conclusion
Lumbar discectomy improved function and decreased pain level to similar extent in both younger and older patients suffering from radicular symptoms related to lumbar disc herniation.
Introduction
Symptomatic lumbar disc herniation (LDH) contributes for only 5% of all low back pain (LBP) complaints. 1 However, it is the most common reason for spinal surgery.1,2 With increasing age of the population, LDH become more and more common and affect yet older patients. 3
When considering surgery, there is an instinctive hesitation toward operation on elderly patients due to co-morbidities and generally poorer physical performance. While some studies show worse outcomes, higher complication rate, and low satisfaction score following spinal surgery in the elderly,4-6 other studies provide results of relatively high satisfaction rate with no added complication rate nor lesser outcomes.7-9
Previous studies show a recurrence of back pain in about 25% of patients, during long-term follow-up, following LD.10,11 Some provide the assumption that structural changes, after disc removal, are to blame.10,12 We assume that due to degeneration of the disc, the adjacent vertebrae and articulations are in already ankylotic state which limits the structural changes after discectomy, and thus, providing better outcomes and higher satisfaction in elder patients.
As of now, no decisive conclusion appears in the literature regarding the clinical efficacy of discectomy in the elderly and satisfaction rate post-operative. The purpose of this study was to assess age-related difference in patient reported outcomes (PROs) of patients undergoing LD for chronic low back and radicular pain without neurological compromise.
Materials and Methods
Study Design
We conducted a retrospective analysis of data of patients who underwent lumbar discectomy in our institution between 2014 and 2017. No informed consent was needed for this study. The study was approved by our institutional ethical board.
Patient Population
All patients who underwent lumbar discectomy for symptomatic disc herniation in the spine unit of our institution were candidates for this study. Inclusion criteria were (1) non-urgent lumbar discectomy; (2) intractable sciatic pain and disability related to herniated disc with symptoms duration of at least 3 months irresponsive to non-operative treatment; (3) isolated single-level herniation without other spinal pathology in the pre-operative MRI; and (4) a minimum of 12 months follow-up. Exclusion criteria were (1) previous spinal surgery; (2) multi-level disc involvement; (3) urgent surgery due to neurological deficit; and (4) work accident injury. Patients were divided into two groups by their age: group 1 of younger patients (<60 years old) and group 2 of older patients (≥60 years old). Since the semi-elective nature of the surgery, patients elected for this operation are with ASA score of 1 or 2.
Study Protocol
All patients underwent a full clinical evaluation including physical examination and MRI scan prior to the surgery. The same surgical technique was used in all operations and performed by single senior surgeon (Y.F): (1) marking the surgical level; (2) performing a midline longitudinal incision to the interlaminar gap; (3) partial exposure of the spinous process and lamina; (4) partial laminotomy and resection of flavum to expose the exiting nerve roots; and (5) nerve retraction and removal of herniated disc. Post-operatively, all patients were allowed to mobilize as pain allowed. Isometric strengthening and an exercise program were started 6 weeks following surgery.
Outcome Measures
Data from medical records and lumbar spine imaging (x-ray, CT, and MRI scans) of the patients were collected and compared between the study groups. Patients were followed up in the outpatient clinic at 6 weeks, 6 months, and a phone call visit at 1 year post-operatively. Clinical outcomes were assessed by comparing patients’ self-reported (1) back and radicular pain using visual analog scale (VAS); (2) related disability using the Oswestry Disability Index [ODI] 13 ; and (3) SF-12 questionnaire using a 0 to 100% satisfaction score, where a higher score indicates more satisfaction and better quality of life.
Data Analysis
Pre-operative and post-operative data were compared between the groups and within each group. Continuous parameters (age, pain score, ODI, and SF-12) are described as the mean ± standard deviation (SD) and were compared between the groups using unpaired 2-tailed t-test. Categorical parameters (gender and type of work) are described with proportions and were compared between the groups using chi-square test. Comparison within each group between pre-operative and post-operative values, at 6 week and last follow-up, were performed using one-way ANOVA with Tukey post-hoc pairwise comparisons. Statistical analysis was performed using MedCalc Statistical Software (Version 18.0, MedCalc Software bvba, Ostend, Belgium). A probability of .05 and lower was defined as statistically significant.
Results
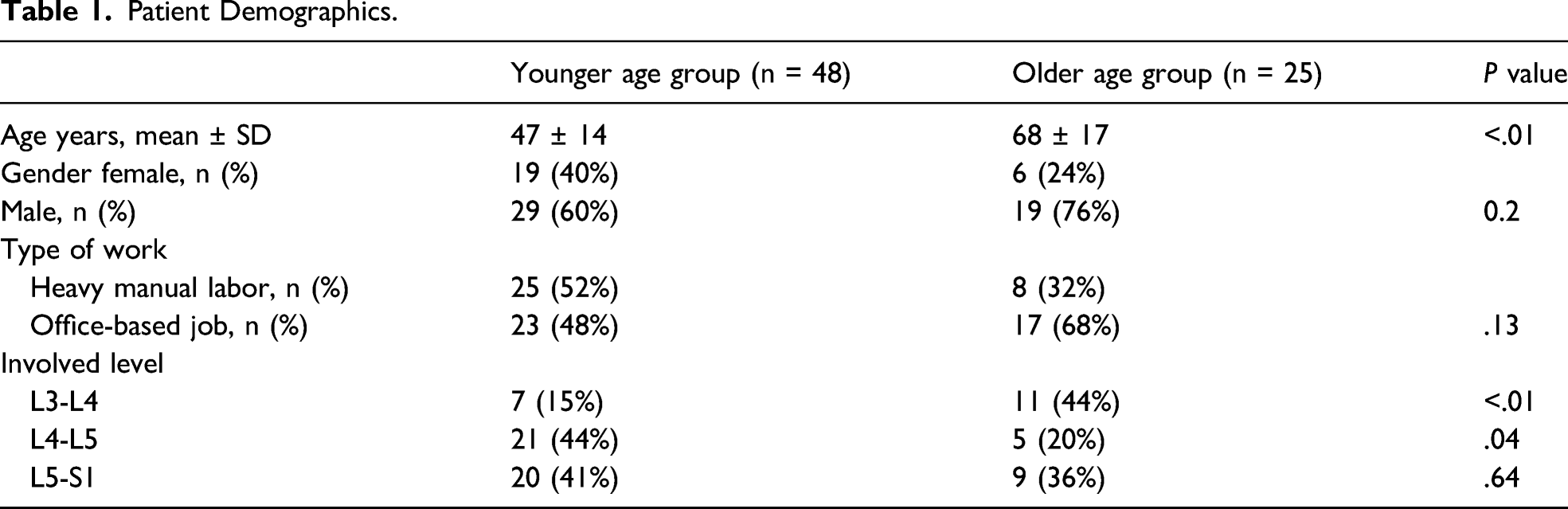
Seventy-three patients met the inclusion criteria, 48 (66%) of them were under 60 years of age, and 25 (34%) were over 60 years of age. The mean age was 47 ± 13 (range 34–60) and 68 ± 8 (range 60–76) in the younger and older age groups respectively (P < .01). Both groups (younger and older patients) included more males than females (60% vs 40% and 76% vs 24%, respectively, P = .2).
Patient Demographics.
Low back pain intensity (VAS) before the surgery was identical in both age groups (7.7 ± 1.2 and 7.8 ± 1.3). The pain levels went down to 1.6 ± 1.4 and 1.8 ± 1.2 at 6 weeks after surgery and at the last follow-up time point among the younger age group vs 2.0 ± 1.5 and 2.2 ± 1.3 in the older age group. However, there was no statistically significant difference in the pain levels between the groups, at both time points post-surgery (P > .05).
The same trend was noted in the ODI data. The scores in both age groups before the surgery were almost identical, 49 ± 15 in the younger age group and 48 ± 18 in the older age group. The decrease in the ODI scores after the surgery was statistically significant compared to the scores before the surgery (P < .01) in both groups, but there was no statistically significant difference between the groups (P > .05) (15 ± 22 and 15 ± 16 6 weeks after surgery and at the last follow-up time point among the younger age group vs 15 ± 20 and 15 ± 17 in the older age group).
Age-Related Comparison of Outcome Measures Between the Groups.

Values are presented as mean ± SD (range).
aComparison between the groups was performed using unpaired two-tailed t-test.
bComparison within the groups between pre-operative and post-operative values at 6 week and the last follow-up were performed using one-way ANOVA with Tukey post-hoc pairwise comparisons.
Discussion
Chronic LBP is assumed to affect about 23% of the population and up to 12% will be disabled by it.14,15 While lumbar disc herniation (LDH) accounts for only 5% of LBP complaints, it is the most common reason for sciatica, and thus, surgery due to back and leg symptoms.1,2 Most of the complaints of sciatica will resolve with conservative treatment, but patients with persistent symptoms or neurological deficit benefit greatly with surgery.1,2,16
The literature discussing and comparing the clinical outcomes of lumbar discectomy (LD) in the elderly and younger patients is scarce. Strömqvist et al. compared the outcomes of surgical treatment for LDH at 1-year post-operative period between elderly (≥65 years of age) and younger patients (20–64 years of age). They found higher VAS scores regarding leg pain, and EQ5D, DOI, and SF-36 scales showed worse patient reported outcomes (PROs) in the elderly. 4 On the other hand, Fujii et al. studied 12 patients aged 65 years and more and compared them to 25 young patients aged between 20–40 years. They found no significant difference between the groups in the manner of post-operative pain. 17 Hai et al. evaluated the outcomes of LDH surgery in patients ≥80 years old and found a comparable satisfaction and pain reduction to patients aged 40–60 years old.
Studies regarding surgery for spinal stenosis hold the same disagreement. Khashan et al. evaluated patients ≥75 years of age and younger than 45 years of age to compare safety and efficacy after decompressive spinal surgery. The younger age group showed a significantly higher improvement in VAS scores and PROs compared to the older group. However, Khashan et al. 18 attribute this difference to the general physical and mental status typical for increasing age. Aleem et al. included patients younger and older than 70 years who underwent surgery for lumbar spinal stenosis. They found that the improvements rates in ODI among the elderly patients were comparable to those of younger patients. 19
Although the results of this study are not better in the elderly group, they are neither inferior. We assume that the reason for the satisfactory results in the elderly group are related to the degenerated spine of the elder. Kotilainen et al. examined patients for 3 years after single level disc herniation surgery. They found that 29% of patients suffer from post-operative LBP, and when comparing between different age groups, the rate was lower after the age of 50 years. 21 Schaller reviewed 2353 records of patients after primary microdiscectomy and concluded that younger patients (in their 40 s) are prone to intervertebral instability due to post-operative narrowing of the intervertebral space. Galbusera et al. 22 conducted a literature review and reached an agreement that a degenerated disc and adjacent structures provide a stiffer, less prone to changes, spine. It is our assumption that removing a herniated disc from an ankylotic spine will result in less mechanical and structural changes in the adjacent vertebrae.
The data from our study revealed that the outcome measures of pain, disability, and quality of life, as measured by VAS, ODI, and SF-12 scores, were similar for both younger and older patients pre- and post-operatively. These findings are in agreement with some of the previous studies.17,20 Although a significant improvement was observed post-operatively in both groups, no statistically significant differences was observed between the age groups. When considering complications, the literature shows 4–8% of accidental durotomy, ∼1% SSI and <1% neurological injury. 2 In our study, we found none of the above. It might be due to our small number of patients operated by an experienced single surgeon.
Limitations and Strengths
As a retrospective study, our study holds some inherent limitations. Adding to that, our study groups were not of the same size; however, it is in correlation with the incidence of lumbar disk herniation being treated surgically in the general population.
Our study holds some strengths as this study was conducted in a single center, and all the surgeries were performed by a single surgeon those minimizing differences in surgical techniques. Furthermore, to prevent bias resulting from secondary gain, patients who introduced with work accident or traffic accident litigation were excluded from this study.
Conclusion
Our study shows that surgery for lumbar disc herniation in the elderly is not inferior to surgery in the young in the manner of pain recurrence and satisfaction rate as reported by the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.