
Abstract
Objective:
Our goal was to deduce the prevalence of low back pain among medical doctors in the teaching hospitals of Karachi, Pakistan, along with its associated variables and the functional disability accompanying it.
Methods:
This cross-sectional study was conducted among medical doctors from Creek General Hospital and United Hospital, affiliated with United Medical and Dental College, Karachi, Pakistan. A sample of 80 participants was included in this study, and a non-probability convenient sampling with randomization was utilized. Using a three-part questionnaire that included the Oswestry Disability Index, all participants were scrutinized for low back pain with its characteristics, associated risk factors, and functional disability.
Results:
Seventy percent of medical doctors included in this study suffered from the problem of low back pain, with 68% experiencing it over the last 3 months to 1 year. Furthermore, 89% and 11% suffered from minimal and moderate disability, respectively, affecting day-to-day and work life. Moreover, this study also found a significantly positive association (p value < 0.05*) of low back pain with age and work-related characteristics and was more common in those with work experience between 1 and 10 years, >8 working hours, >4 standing hours, and belonging to the surgery and medicine specialties. The association was significantly positive according to the chi-square/Fischer exact test.
Conclusion:
Our study addressed the evidence that low back pain is prevalent among medical doctors in teaching hospitals in Karachi, Pakistan, potentially affecting patient treatment and student education and accentuating the need for further intervention and research among doctors worldwide.
Keywords
Introduction
Low back pain, more commonly referred to as “LBP,” is a feeling of discomfort and pain between the inferior gluteal folds and the 12th rib; it may or may not accompany leg pain. 1 Almost 84% of the populace experience LBP at some point in their lives, 23% experience persistent LBP, and around 11%–12% become disabled due to this pain. 2 Among many other musculoskeletal issues, LBP is one of the issues associated with employment status and condition. 3 The general population suffers from LBP less frequently than healthcare professionals.4–6 Back pain is due to many diseases, but psychosocial factors are the leading cause of chronic LBP. 7 Around 37% of LBP cases are caused by working continuously. 8 It is most common among healthcare workers such as doctors, nurses, nursing assistants, and paramedic staff, who are part of direct patient care. Many studies found that healthcare workers had the highest prevalence of LBP, ranging from 50% to 70%,9–11 and female healthcare professionals tended to suffer slightly more than their male counterparts. 12 In addition, according to a systematic review, the prevalence of LBP in physicians was between 33% and 68%. 13 Many factors contribute to lower back pain among medical professionals, especially doctors. These factors include the type of occupation; poor body posture; heavy physical work; job stressors; high psychological demand; bending and twisting. 10 In medical practice, especially in undeveloped countries such as Pakistan, the prevalence of LBP, its characteristics, associated factors, and functional disability among doctors in teaching hospitals, have not been investigated. Many studies have primarily focused on nurses or other healthcare workers, taking them as a whole, while not taking doctors into account to be also affected by it or having a comparative study between different healthcare workers to represent which type of healthcare work is at higher risk of LBP.14–19 Hence, we aimed to determine the prevalence of LBP and its characteristics among medical doctors in teaching hospitals in Karachi, Pakistan, along with its associated risk factors and the degree of functional disability resulting from LBP leading to the impairment and hindrances in day-to-day routine and work life.
Methods
Study setting, design, and period
This multi-institutional cross-sectional study was conducted on medical doctors from Creek General Hospital (CGH) and United Hospital (UH), both affiliated with United Medical and Dental College, from December 1, 2021, to March 30, 2022, after receiving ethical approval from the United Medical and Dental College’s Institutional Review Board (IRB committee).
Sample size and sampling techniques
With 95 medical doctors enrolled in the two institutes at the time of study, the openepi sample size calculator was used to determine a sample size of 76 {n = deff Npq/(d2/1.962 (N−1) + pq)}, 20 with a margin of error of 5%, a confidence level of 95%, and a response distribution of 50%. In addition, a total of 85 participants were recruited, and 80 of them consented and filled out the form. The confidence interval of the proportion of the sample 85 was found to be between 0.941 ± 0.050078 (0.89–0.99). The response rate was 94%. As it was easy to approach participants from the two institutes, a non-probability convenient sampling technique was utilized, but randomization was implemented to reduce bias by selecting each participant at random through Excel from a list of doctors compiled at the time from these two institutes.
Inclusion and exclusion criteria
All the medical doctors associated with the two teaching hospitals, CGH and UH, were included in this study. All physicians and surgeons from the clinical side of CGH and UH were included. All Senior Registrars, Assistant Professors, Resident Medical Officers, Professors, Associate Professors, Consultants, and Registrars belonging to the clinical side of CGH and UH were included in this study. However, doctors not associated with the two teaching hospitals of CGH and UH were excluded from this study. All the doctors from the basic sciences were excluded from this study. All house officers of CGH and UH were excluded from this study. Doctors suffering from any chronic life-threatening disease, psychological disorder, history of family psychological disorders, or refusing to give written consent were excluded from this study.
Study tool and data collection procedure
A modified, self-administered, and semi-structured questionnaire by Tanzil et al. 21 with a consent form was utilized. The questionnaire can be seen in the supplemental section (Supplemental Files 1 and 2), consisting of three sections. Part I was based on demographic characteristics of doctors (interviewed about their general health, other associated comorbid conditions, working hours, job environment, and smoking), Part II consisted of self-reporting questions about back pain and its characteristics which were used to scrutinize LBP and its characteristics, and Part III consisted of the Oswestry LBP disability questionnaire. 22 The Oswestry Disability Index (ODI) instrument has ten components that assess various motor activities, including sleeping, sitting, standing, lifting, and traveling. Each component is assigned a zero to five score, with higher scores indicating greater disability. A percentage is calculated by multiplying the overall score by two. A premade grading system divides the severity of a disability into five groups, ranging from mild to bedbound. The survey proceeded with a consent form detailing the study’s purpose and the horizon of the subject’s involvement. The data were collected in person by the authors from United Medical and Dental College by approaching the doctors during hospital hours (Table 1).
Operational Definitions and Unit and Categories of Variables.

LBP: low back pain; ODI: Oswestry Disability Index.
Instrument validity
Three members of the IRB committee of the United Medical and Dental College in Karachi, Pakistan, examined the questionnaire to ensure its validity and absence of homogeneity, double-barreled questions, and any writing or grammatical errors. A pilot study involving ten medical doctors (12.5% of medical doctors) was conducted to assess the questions’ validity and clarity. The analysis also took into account the pilot study’s surveys.
Statistical analysis procedure
The responses were entered on an Excel sheet and then imported to SPSS version 23 for analysis. Frequencies and percentages are reported for categorical variables. The chi-square/Fischer exact test is applied to assess the relationship between variables. A p value of <0.05* is considered statistically significant. The prevalence of LBP and functional disability was measured using descriptive statistics and the Fischer exact test. In contrast, the demographics and characteristics of LBP were calculated using descriptive statistics, and the chi-square test was used to measure the risk factors related to LBP.
Ethical consideration
The survey was conducted with the utmost confidentiality, and only the researchers had access to the participants’ information.
Reporting of the study
Strobe guidelines are followed for reporting of the study (supplemental file 3).
Results
Demographic data and their job-related characteristics
Out of the 80 participants, 55% were male doctors and 45% were female doctors. Around half of the participants were 25–35 years of age, and the rest were over 36 years of age. Only six (7.5%) and one (1.3%) doctors were suffering from hypertension and diabetes, respectively. A brief description of the demographic and job-related characteristics of participants is given in Table 2.
Demographic data of doctors and their job-related characteristics in teaching hospital, Karachi, Pakistan.

Frequency LBP and associated functional disability:
Overall, 56 (70%) of all doctors in a teaching hospital experienced LBP. The functional disability associated with LBP was assessed by the “Oswestry Low Back Pain Scale” among the doctors who reported to have suffered from LBP, and it was found that the majority 50 (89.3%) of them had minimum disability (Figure 1). The results are statistically significant based on the Fischer exact test (p value = 0.000*) when tested for the difference between the frequency of LBP and the difference between associated functional disability.
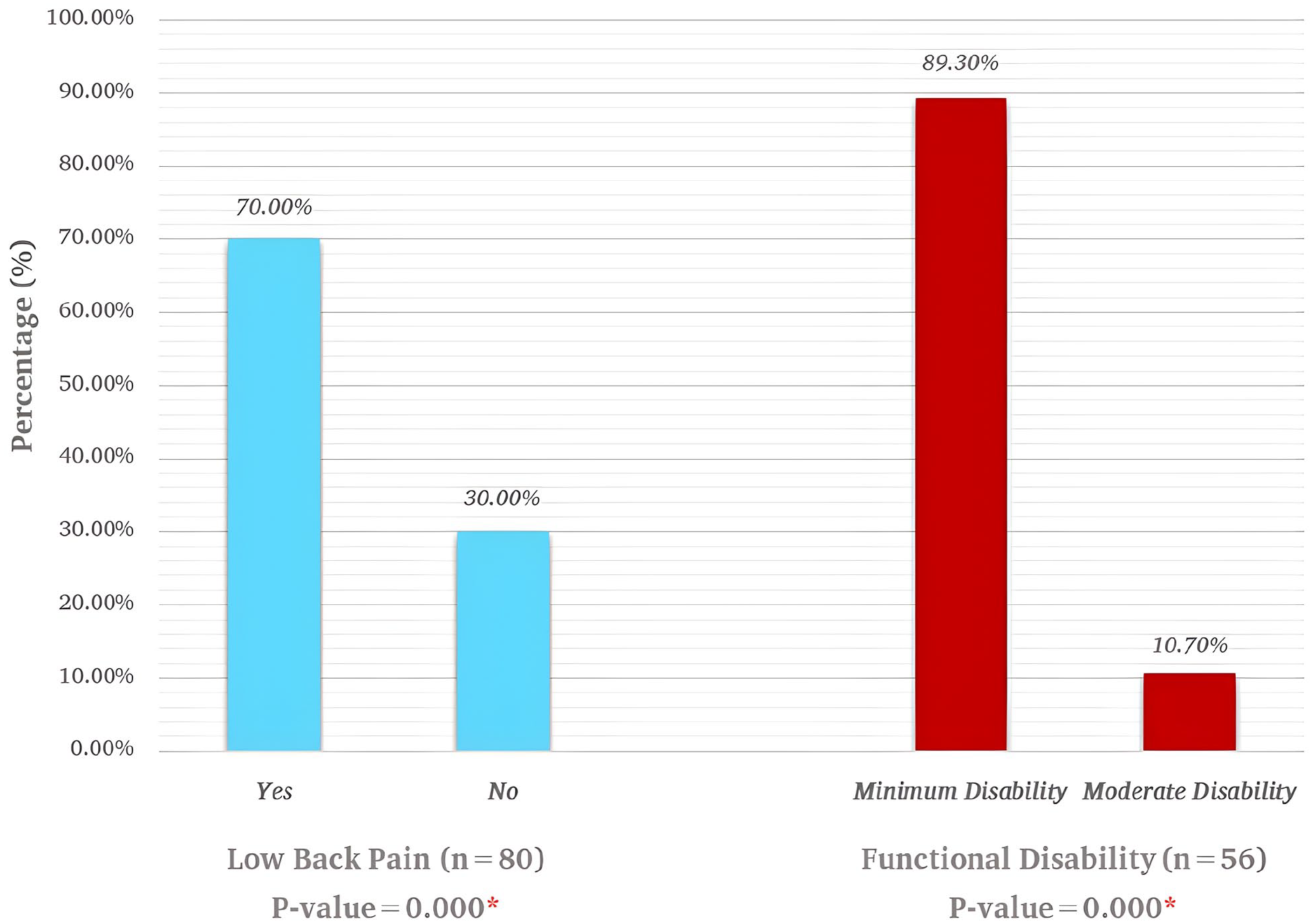
Frequency of low back pain and functional disability associated with it among doctors in a teaching hospital of Karachi, Pakistan.
Characteristics of LBP
However, those reported suffering from LBP, majority of them have experienced LBP for a year and less than 3 months, with the minority suffering over 5 years and 1–5 years, respectively, with the episodes commonly ranging from having LBP experienced at least not very often (once a month) by half of the participating doctors and 48.3% having experienced it in the last 12 months. Furthermore, the intensity of LBP was found to be mild-to-moderate in the majority of the participants (Figure 2). Furthermore, only 9 (16.1%) resorted to taking any medication for LBP, while 47 (83.9%) did not resort to any treatment, which was statistically significant based on the Fischer exact test’s evaluation of the difference in opting for treatment (p value = 0.000*).
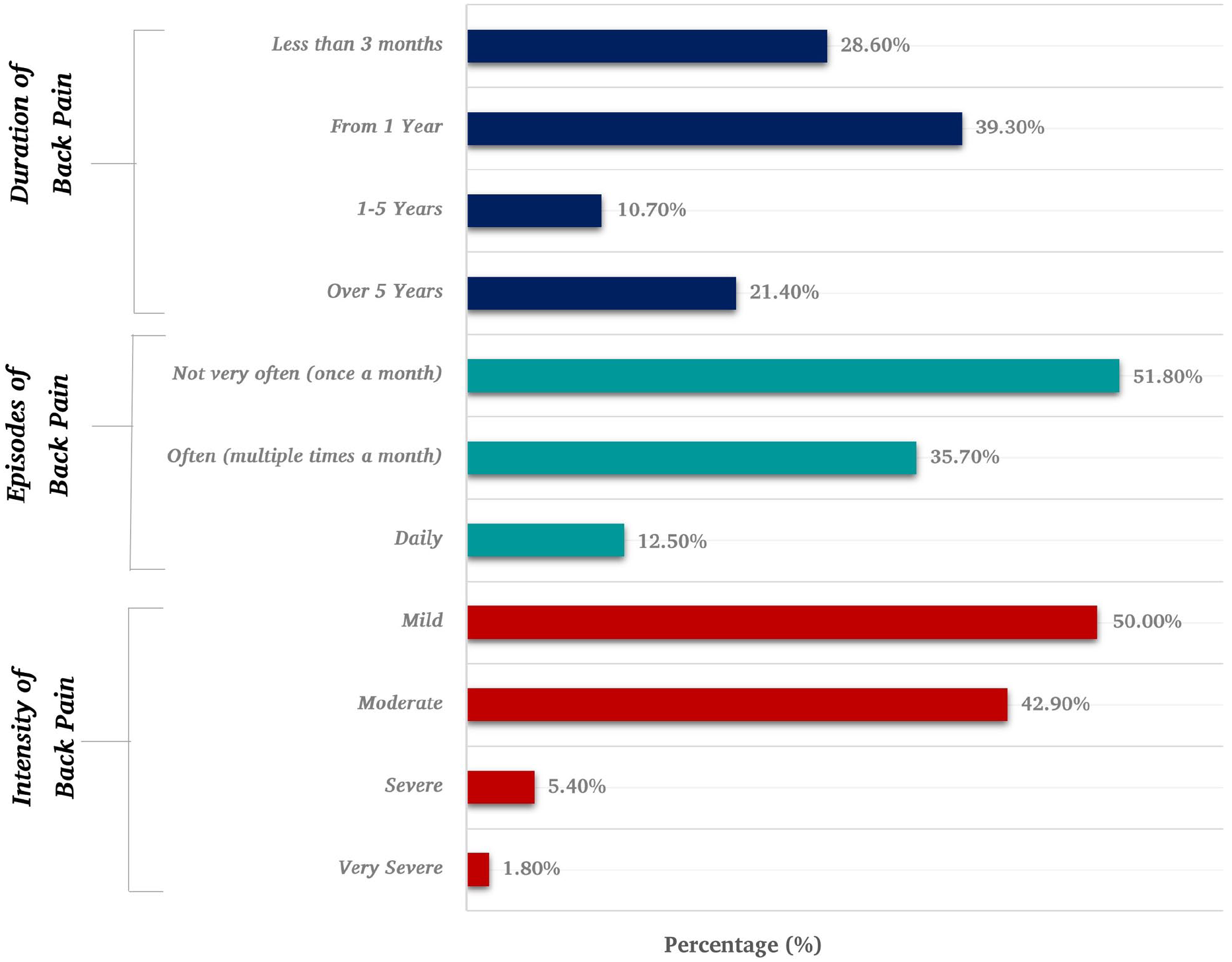
Characteristic of low back pain among doctors in a teaching hospital of Karachi, Pakistan (n = 56).
Moreover, the LBP was also associated with other radiating symptoms in 17 (30.4%) participants, which included stiffness of the lower limb in 10 (17.9%), pain radiating to the lower limb in 5 (8.9%), and numbness of the lower limb in 2 (3.6%), while 39 (69.6%) had only back pain.
Association of low back with demographic and work-related characteristics
In terms of the proportion of LBP among the participants, there was no discernible difference between gender, position, or physical exercise, which, when analyzed using the chi-square test, demonstrates that there was no statistically significant association between LBP and any of these variables (p value > 0.05*). The proportion of LBP among participants was significantly higher in doctors aged 24–44 years and among those working in the field of surgery, with working experience of 1–5 years and 6–10 years, working for more than 8 h a day and standing for more than 4 h a day. The chi-square test revealed that there is a statistically significant association between LBP and demographics’ age and work-related characteristics (p value < 0.05*), indicating that these individuals are more likely to experience LBP (Table 3).
Association of low back pain with demographic and work-related characteristics among doctors in a teaching hospital of Karachi, Pakistan (n = 80).

indicates a significant association between LBP with demographic’s age and work-related characteristics.
Discussion
Our study is an unprecedented attempt in Pakistan while also concentrating on a widespread but unaddressed health issue related to occupation among doctors in a low- to middle-income country. The purpose and aim of this study was to shed light on the prevalence of LBP along with its impact on the working and daily lives of doctors in our community. Our study shows that 70% of doctors working in the teaching hospitals of Karachi are suffering from the problem of LBP. A study by Lee K.Y 25 in a hospital in Selangor, Malaysia, and by Raza A et al. 26 in Lahore found that 65% and 51.55% of doctors had LBP, respectively, which is similar to our study. However, a study by Shah S. et al. 27 among doctors in Surat found that the prevalence of LBP was 36.84%, which is less than our study. Our study holds its relevance as it shows the highest percentile of LBP among doctors because of its conduct in teaching hospitals, where doctors deal not only with patients but also with students. Furthermore, the prevalence in our study is significantly higher than in other studies because it was conducted in a Low-middle-income country, where doctors work longer hours and have less access to healthcare facilities 28 and because it was conducted shortly after the COVID era, when the workload was likely higher than in the pre-COVID era.
Our study also highlights that most doctors, 68%, are suffering from the problem of LBP from 3 months to 1 year, having episodes once a month. In comparison, a study by Raza A et al. 26 in Lahore showed that 51.5% of doctors suffered from LBP in the last 6 months, and a study by Al-Ruwaili B et al. 29 showed that 70.5% of physicians suffered from LBP in the last 12 months, which is in line with the findings of our study. Moreover, a survey conducted in Pakistan by Tanzil S. 21 and a systematic review conducted by Mehrdad R. 30 in Iran showed that 58% of all healthcare workers, including doctors, suffered from LBP with 1–3 episodes of LBP over a period of 12 months. Similarly, a study by Negash NA. et al. 14 at a hospital in Northwest Ethiopia presented that 57.46% of all healthcare workers, including doctors, suffered from LBP, and a study conducted in Saudi Arabia by Alnaami I. 9 and TS Wong. 10 in the district hospital of Malaysia showed 73.9% and 72.5% of healthcare workers including doctors, presented with LBP, respectively. All of the aforementioned studies support our study’s conclusion that more than 50% of doctors suffer from LBP. Nonetheless, the percentile of LBP in our survey was relatively higher because this study is primarily focused on doctors and not all healthcare workers, indicating that doctors are significantly impacted by the problem of LBP in the teaching hospitals of Karachi, Pakistan, as a result of their workload and the hospital environment.
Our study also outlines that 66% of male and 75% of female doctors in a teaching hospital are experiencing LBP, which is in agreement with the study conducted by Tanzil S. 21 and Mehrdad R. 30 which has similar findings: 40.5% male; 44.8% female and 39% male; 40% female healthcare workers, including doctors, suffered from LBP, but there is a significant difference when comparing among those reporting of LBP because these studies include all healthcare workers, which enlightens our study in showing that doctors in the teaching hospitals of Pakistan experience more LBP as compared to other healthcare workers in general as a whole, doctors of both genders are at risk of experiencing more LBP due to the increased workload of seeing patients, doing surgeries, and educating medical students. It was also seen that female doctors tended to suffer from LBP slightly more than male doctors, which could be attributed to a number of factors presented by Wáng YX et al. 31 including psychological factors, hormone fluctuation, menstruation, and a smaller SI joint surface area compared to males, resulting in greater stress across the joints. Another study conducted by Raza A et al. 26 in Lahore presented that 61.85% of male doctors and 38.15% of female doctors suffered from LBP, which opposed the findings of our study. The reason would be that our study had an almost equal proportion of male and female doctors, which is supported by a study conducted by Shah S. et al. 27 in Surat, where female doctors suffered slightly more LBP than male doctors.
Our study also elaborates on the impact of LBP on doctors’ day-to-day lives, presenting that 89% have a minimum disability and 11% suffer from a moderate disability. On the contrary, a study by Almalki M. et al. 32 among medical practitioners and Tanzil S. 21 among healthcare workers including doctors showed the majority to suffer from minimal disability and the minority to suffer from moderate disability, which agrees with our study’s findings. The reason would be that as LBP progresses in intensity it causes different stages of functional disability, which is backed up by the severity of LBP presented by Shah S. et al. 27
Our study also shows that LBP is highly prevalent in doctors between 25 and 44 years of age, who have work experience of between 1 and 10 years, working for more than >8 h a day and standing for more than >4 h a day. Furthermore, all of the above factors were statistically determined to have a significant association with LBP with the chi-square test (p value < 0.05*), which is similar to the findings of the study conducted by Shah S. et al. 27 in Surat among doctors, presenting that LBP was more commonly prevalent in <40 years of age, working for 8–10 h, and prolonged standing, and a study by Raza A et al. 26 in Lahore depicted that doctors working for 6–12 h suffered from LBP. Similarly, a study by Tanzil S. 21 and by TS Wong 10 in Malaysia on healthcare workers, including doctors, as well as a study by Kim J-Y 26 work-related LBP presented the same factors as the cause of LBP. The reason would be giving the body less time to rest and putting more strain on tendons and muscles by constantly working, standing for longer hours, and bending for the examination of patients, as mentioned by Negash NA. et al. 28
Furthermore, of all the participants, most doctors working in the teaching hospitals of Karachi had minimal to moderate functional disability, which depended upon the severity of the LBP, and had the power to do their daily activities with some hindrances affecting their day-to-day life slightly. Therefore, this study identifies the fact that the workload and working hours of doctors in teaching hospitals in a low- to middle-income country are contributing factors to LBP in them, which affect the quality of education and health treatment toward students and patients, respectively. Therefore, albeit having a limited extent of this study, it has significantly contributed to identifying the prevalence of LBP among doctors and its association with other factors and accompanying functional disability.
Limitations and strength
This study has some limitations: First, this cross-sectional study was conducted in two teaching hospitals of Karachi while excluding other hospitals that are not associated with teaching due to outreach and compliance from doctors. Second, foremost, as the information related to LBP, its characteristics were self-perceived/reported, which might have had a slight bias due to recall memory or participant bias. The third limitation of this study is that it was conducted in a low- to middle-income country, which can account for low- and middle-income economies, but results might differ in higher and upper middle-income economies where the hospital management system, as well as the integration of education associated with doctors, has a different approach.
This study also has its strength: it was conducted in two teaching hospitals, which present the maximum amount of workload on a doctor from patients, students, and the hospital’s environment; this study shows the LBP to the extreme extent that a doctor suffers, as well as this study gives a baseline reading for the doctors who are associated and working in a nonteaching hospital of Karachi, Pakistan. The strength of our study also lies in it being conducted after the era of COVID lockdown, which also put the doctors under a heavy workload of both patients as well as the students that had come to the clinical setting who were absent during the lockdown period. As a result, this study emphasizes the number of work hours and period of standing, age, and specialty that resulted in the contributing factor of LBP among doctors at teaching hospitals in Karachi. Another strength of this study is the privilege of being conducted in a developing economy and in a teaching hospital that also runs on trust funding and where a large number of patients come for free treatment and doctors have to work extra hours, which gives a better understanding of the LBP problem that doctors are facing, a major contributing factor to the decline and dropouts in the medical field due to a lack of attention toward doctors’ health. Also, our study’s response rate was excellent regarding doctors. Lastly, many studies have just focused mainly on nurses or healthcare workers as a whole; in doing so, they have neglected taking doctors separately, who are the backbone of medicine, which our study has considered.
Conclusion
Our results highlighted the alarming and unaddressed fact that the LBP problem is widely prevalent among medical doctors working in a teaching hospital of Karachi, Pakistan. Both male and female doctors are equally experiencing the issue of LBP due to the workload and lifestyle they are exposed to, which has a toll on their health and might be affecting the delivery of health services to patients and education to students. This study implies that efforts to prevent and reduce occupational risk factors for LBP in doctors are needed. Multi-institute studies with good methods should be encouraged to find out more about the LBP in doctors around the world, both in teaching hospitals and in hospitals that do not teach.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231157217 – Supplemental material for Prevalence of low back pain among medical doctors of the teaching hospitals in Karachi, Pakistan: A cross-sectional survey
Supplemental material, sj-docx-1-smo-10.1177_20503121231157217 for Prevalence of low back pain among medical doctors of the teaching hospitals in Karachi, Pakistan: A cross-sectional survey by Salman Javed, Muhammad Hamza Dawood, Muhammad Waseem Memon, Ibrahim Zahid Selod and Arshi Seja in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231157217 – Supplemental material for Prevalence of low back pain among medical doctors of the teaching hospitals in Karachi, Pakistan: A cross-sectional survey
Supplemental material, sj-docx-2-smo-10.1177_20503121231157217 for Prevalence of low back pain among medical doctors of the teaching hospitals in Karachi, Pakistan: A cross-sectional survey by Salman Javed, Muhammad Hamza Dawood, Muhammad Waseem Memon, Ibrahim Zahid Selod and Arshi Seja in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121231157217 – Supplemental material for Prevalence of low back pain among medical doctors of the teaching hospitals in Karachi, Pakistan: A cross-sectional survey
Supplemental material, sj-docx-3-smo-10.1177_20503121231157217 for Prevalence of low back pain among medical doctors of the teaching hospitals in Karachi, Pakistan: A cross-sectional survey by Salman Javed, Muhammad Hamza Dawood, Muhammad Waseem Memon, Ibrahim Zahid Selod and Arshi Seja in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank United Medical and Dental College for ethically approving our study and endorsing our efforts to conduct research.
Author contributions
SJ and MHD are the guarantor of this study. The contributions of each author are as follows: SJ was involved in research proposal, study design, and manuscript writing as well as supervision. MHD was involved in questionnaire development, majority manuscript writing, data collection, data coding, and data analysis. MWM and IZS was involved in checking analyzed results accuracy/credibility, reviewing, and proofreading. AS was involved in data collection and data entry. All authors have approved the submitted version and have agreed to be personally accountable for their own work and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which they were not personally involved, are appropriately investigated.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the Institutional Review Board of United Medical and Dental College at Karachi city (ref. no: UMDC/Ethics/2021/06/12/297).
Informed consent
Written informed consent was taken from all the doctors for their participation during the collection process.
Data availability statement
The datasets that support the findings of this study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.