
Abstract
Objective
To investigate the correlations between pain, quality of life, fatigue, levels of depression, disability and activity, and sleep quality and common sleep disorders in patients with rheumatoid arthritis (RA).
Methods
This multicentre, cross-sectional study enrolled patients with RA and sex- and age-matched control subjects. Clinical, sociodemographic, serological and therapeutic data were collected. Data from the Disease Activity Score (DAS28-CRP), the Epworth Sleepiness Scale (ESS), Pittsburgh Sleep Quality Index (PSQI), Berlin questionnaire, a visual analogue scale to evaluate fatigue severity (VAS-F), health assessment questionnaire disability index (HAQ-DI) and the Center for Epidemiological Studies-depression (CES-D) score were analysed.
Results
The study enrolled 247 patients with RA (190 females and 57 males) and 60 control subjects (50 females and 10 males). The PSQI for patients with RA was significantly associated with the DAS28-CRP, HAQ-DI and VAS-F. There was a significant correlation between the CES-D score, the Berlin questionnaire and the HAQ-DI and the age of control subjects. Multiple linear regression analysis demonstrated that HAQ-DI (coefficient β = 0.103) and VAS-F (coefficient β = 0.028) significantly predicted the risk of sleep apnoea.
Conclusion
Patients with RA may suffer from poor sleep quality, which is attributed to depression, fatiguability, disability and disease activity.
Introduction
Rheumatoid arthritis (RA) is an autoimmune disease with an uncertain cause that mostly affects joints and progresses to deformation. 1 The prevalence of RA has been observed to range between 0.5% and 1%, with a female-to-male ratio of 3:1. 2
Poor sleep quality is frequent in the chronic rheumatic disease population. 3 RA patients have a significant prevalence of obstructive sleep apnoea (OSA) 4 and insomnia, 5 among other main sleep disorders. Sleep difficulties were experienced by 72% of 100 RA patients, 6 which was likely due to pain-related arousals 6 or anatomic abnormalities that might induce upper airway restriction. 7 Fatigue in RA contributes significantly to decreased quality of life and, hence, increases disease burden, making RA management more difficult. 8 Despite this, people with RA have expressed a lack of assistance in the management of RA fatigue in healthcare facilities. 9 Depression, which is common in RA, has been linked to fatigue and sleep disturbances. 10
This current study investigated the association between common sleep disorders, sleep disturbance, and the risk of OSA with pain, quality of life, fatigue, depression levels, disability, disease duration, and disease activity in RA patients.
Patients and methods
Study design and participants
This multicentre, cross-sectional study was conducted in the Departments of Rheumatology of King Fahad Hospital in Medina, Saudi Arabia and Al Azhar University Hospitals in Cairo and Assiut, Egypt between December 2021 and July 2022. The study recruited consecutive patients >18 years and <60 years classified with RA according to the European Alliance of Associations for Rheumatology 2010 classification criteria for RA who agreed to participate in the study. 11 The exclusion criteria were as follows: (i) patients who were pregnant; (ii) patients with any rheumatological disease other than RA; (iii) patients diagnosed with fibromyalgia or other systemic diseases affecting sleep quality.
Age- and sex-matched control subjects met the following inclusion criteria: (i) provided consent to participate in the study; (ii) confirmed the absence of RA or collagen disorders, fibromyalgia, sleep disturbances or depression; (iii) had no family history of RA or collagen disorders in first-degree relatives; (iv) were from the same geographical region as the patients with RA. Healthy control subjects were recruited from the Departments of Medicine at King Fahad Hospital in Medina, Saudi Arabia, and Al Azhar University Hospitals in Cairo and Assiut, Egypt, where they were attending clinics for routine examinations.
The study was conducted under the Helsinki Declaration. Ethical approval was obtained on 30 January 2022, from the research ethical committee at Al Azhar University, Cairo, Egypt (IRB number 1222). All participants provided written informed consent after a clear explanation of the study process. All patient details were de-identified. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 12
Sociodemographic and clinical assessment
All study participants had a detailed history and clinical assessment to determine sociodemographic characteristics (age, sex, marital status, body mass index [BMI], educational level, current occupation) and the patient's medical history (disease duration, current therapy, comorbidities).
Laboratory assessments
Laboratory tests, including vitamin D, haemoglobin level, thyroid-stimulating hormone, inflammatory markers (erythrocyte sedimentation rate and C-reactive protein [CRP]), rheumatoid factor (RF) and anti-citrullinated peptide (anti-CCP), were carried out on all patients in the Departments of Laboratory Medicine of King Fahd Hospital and Al Azhar University Hospitals, where the analyses were conducted on the same day as sample collection.
Measurements
Disease activity was measured by rheumatologists based on the Disease Activity Score (DAS28-CRP) and included a measurement of the swollen joint count (SJC), tender joint count (TJC), CRP levels (mg/l) and the patients' global assessment score. DAS28-CRP >5.1 indicates high disease activity, >3.2 to 5.1 indicates moderate disease activity, 2.6–3.2 indicates mild disease activity and 2.6 indicates remission. 13 Fatiguability was evaluated using a visual analogue scale to quantify fatigue severity (VAS-F). 14
Questionnaire evaluation
All participants were reviewed by a qualified investigator (M.K.) who was unaware of each patient’s clinical state, using a structured questionnaire to obtain their responses. Furthermore, every questionnaire was translated into Arabic to minimize patient misconceptions. The following questionnaires were used: (i) risk of sleep apnoea was determined using the Berlin questionnaire. The scoring procedure involves analysing ‘yes or no’ replies and multiple-choice options; 15 (ii) daytime sleepiness was evaluated using the Epworth Sleepiness Scale (ESS). 16 A patient with a score >10 was classified as having excessive daytime sleepiness (EDS); (iii) sleep quality was determined using the Pittsburgh Sleep Quality Index (PSQI); 17 (iv) functional disability was measured using the Health Assessment Questionnaire-Disability Index (HAQ-DI). 18 Each item is answered on a four-level impairment scale. Summing all categories yields the final score; (v) depression was measured using the Center for Epidemiological Studies in Depression (CES-D) score. It was created for the assessment of depressed mood, physical problems and interpersonal discomfort, which are among the primary components of depression. 19
Statistical analyses
The sample size was calculated a priori based on previous research.6–9 A two-sided independent t-test was used to determine it with a significance level (α) of 5% and power (1−β) of 90%. Accordingly, the minimum required sample size was 215.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to determine data normality. When the distribution of continuous data was normal, data are reported as the mean, standard deviation (SD) and ranges. Data that were not normally distributed are presented as the median with the interquartile range (IQR). Frequencies and percentages are used to present categorical variables. The two groups were compared using an independent-sample t-test and the Mann–Whitney U-test. χ2-test was used to analyse categorical variables. To determine the degree of association between two sets of variables, Spearman's rank correlation coefficient was used. The confidence interval was 95% and a P-value <0.05 was considered statistically significant.
Results
A total of 247 patients were consecutively included in the study (190 females and 57 males), with a mean ± SD age of 45.49 ± 8.24 years. Sixty age- and sex-matched controls were also included. The baseline demographic and clinical characteristics of the patients and controls are summarized in Table 1. There were no statistically significant differences between RA patients and the control group in terms of the demographic characteristics, except for the prevalence of diabetes mellitus, which was more common in the RA patients (P = 0.037). There was a strong positive correlation between CES-D score, VAS-F, Berlin questionnaire, ESS, PSQI and HAQ-DI and RF, anti-CCP, TJC, SJC and DAS28-CRP scores (P < 0.01 for all correlations) (Table 2). There was a significant correlation between the Berlin questionnaire and HAQ-DI scores and the age of patients with RA (P < 0.01 for both correlations). There was a significant inverse correlation between scores for the Berlin questionnaire, ESS and HAQ-DI and BMI for control subjects (P < 0.05 for all correlations) (Table 3).
Baseline demographic and clinical characteristics of patients with rheumatoid arthritis (RA) (n = 247) and age- and sex-matched control subjects (n = 60) that were included in a multicentre, cross-sectional study to investigate the association between common sleep disorders, sleep disturbance, and the risk of obstructive sleep apnoea with pain, quality of life, fatigue, depression levels, disability, disease duration, and disease activity.
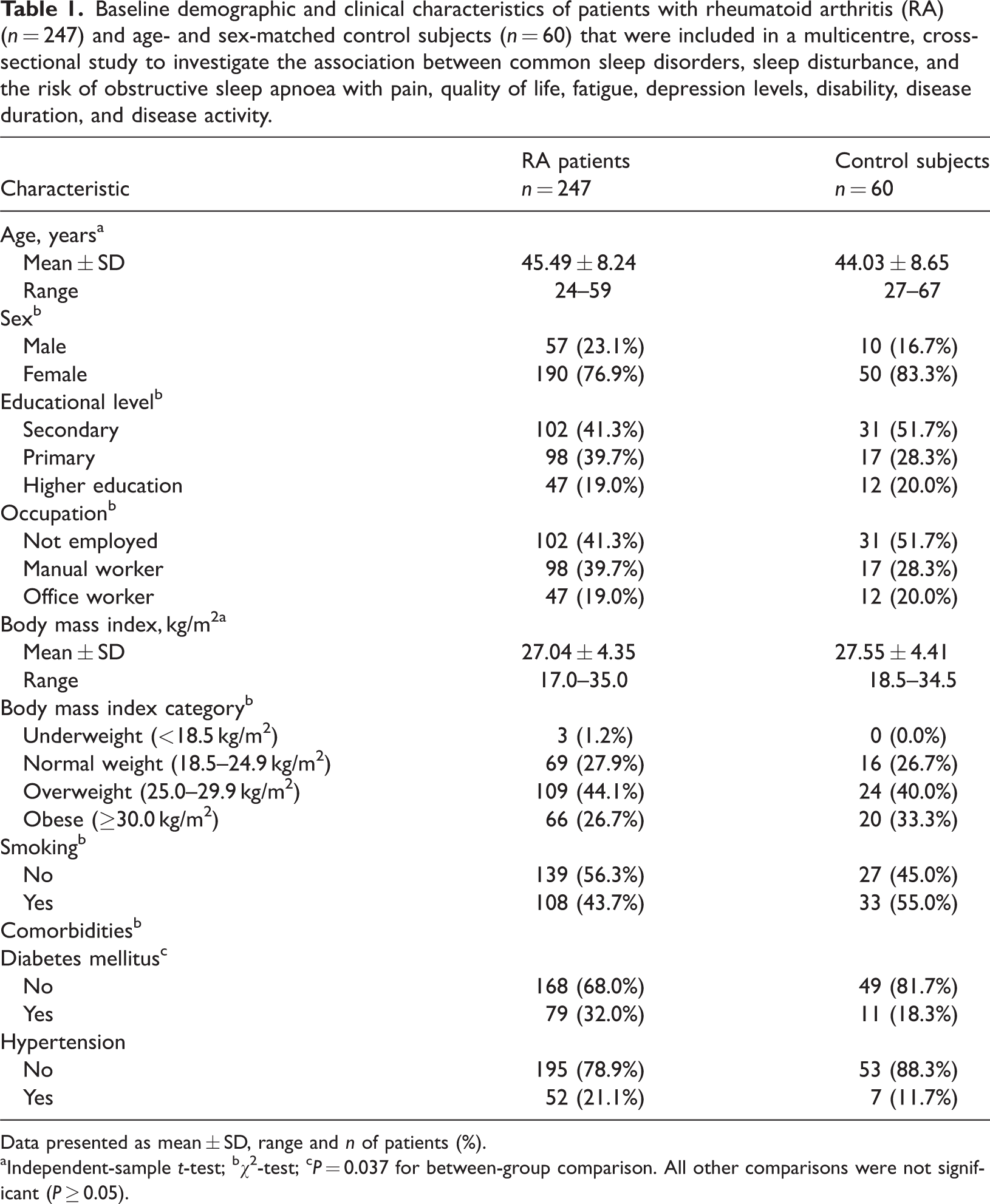
Data presented as mean ± SD, range and n of patients (%).
Independent-sample t-test; bχ2-test; cP = 0.037 for between-group comparison. All other comparisons were not significant (P ≥ 0.05).
Spearman's rank correlation coefficient among different study variables in patients with rheumatoid arthritis (n = 247) that were included in a multicentre, cross-sectional study to investigate the association between common sleep disorders, sleep disturbance, and the risk of obstructive sleep apnoea with pain, quality of life, fatigue, depression levels, disability, disease duration, and disease activity.
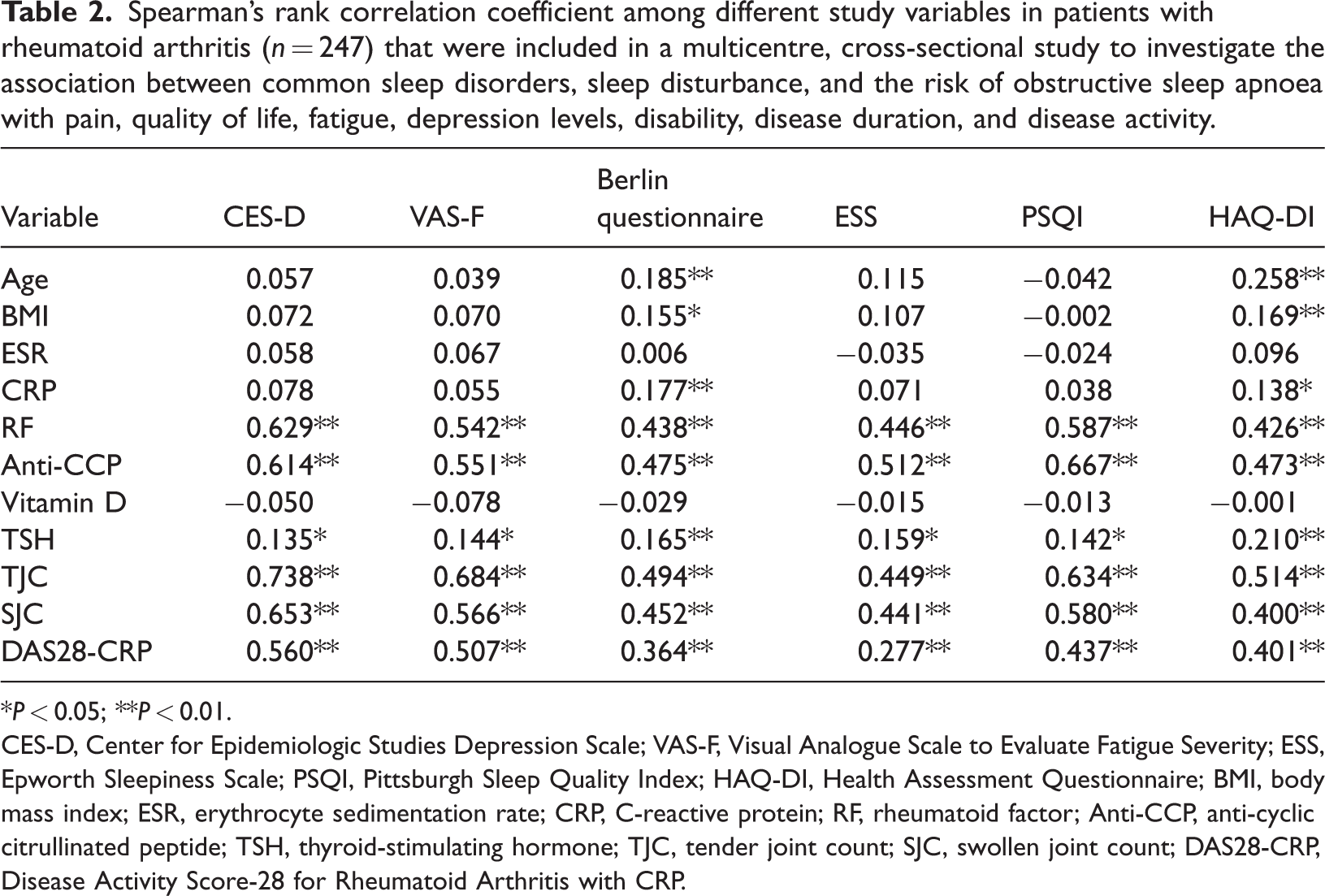
*P < 0.05; **P < 0.01.
CES-D, Center for Epidemiologic Studies Depression Scale; VAS-F, Visual Analogue Scale to Evaluate Fatigue Severity; ESS, Epworth Sleepiness Scale; PSQI, Pittsburgh Sleep Quality Index; HAQ-DI, Health Assessment Questionnaire; BMI, body mass index; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; RF, rheumatoid factor; Anti-CCP, anti-cyclic citrullinated peptide; TSH, thyroid-stimulating hormone; TJC, tender joint count; SJC, swollen joint count; DAS28-CRP, Disease Activity Score-28 for Rheumatoid Arthritis with CRP.
Spearman's rank correlation coefficient among different study variables in control subjects (n = 60) that were included in a multicentre, cross-sectional study to investigate the association between common sleep disorders, sleep disturbance, and the risk of obstructive sleep apnoea with pain, quality of life, fatigue, depression levels, disability, disease duration, and disease activity.
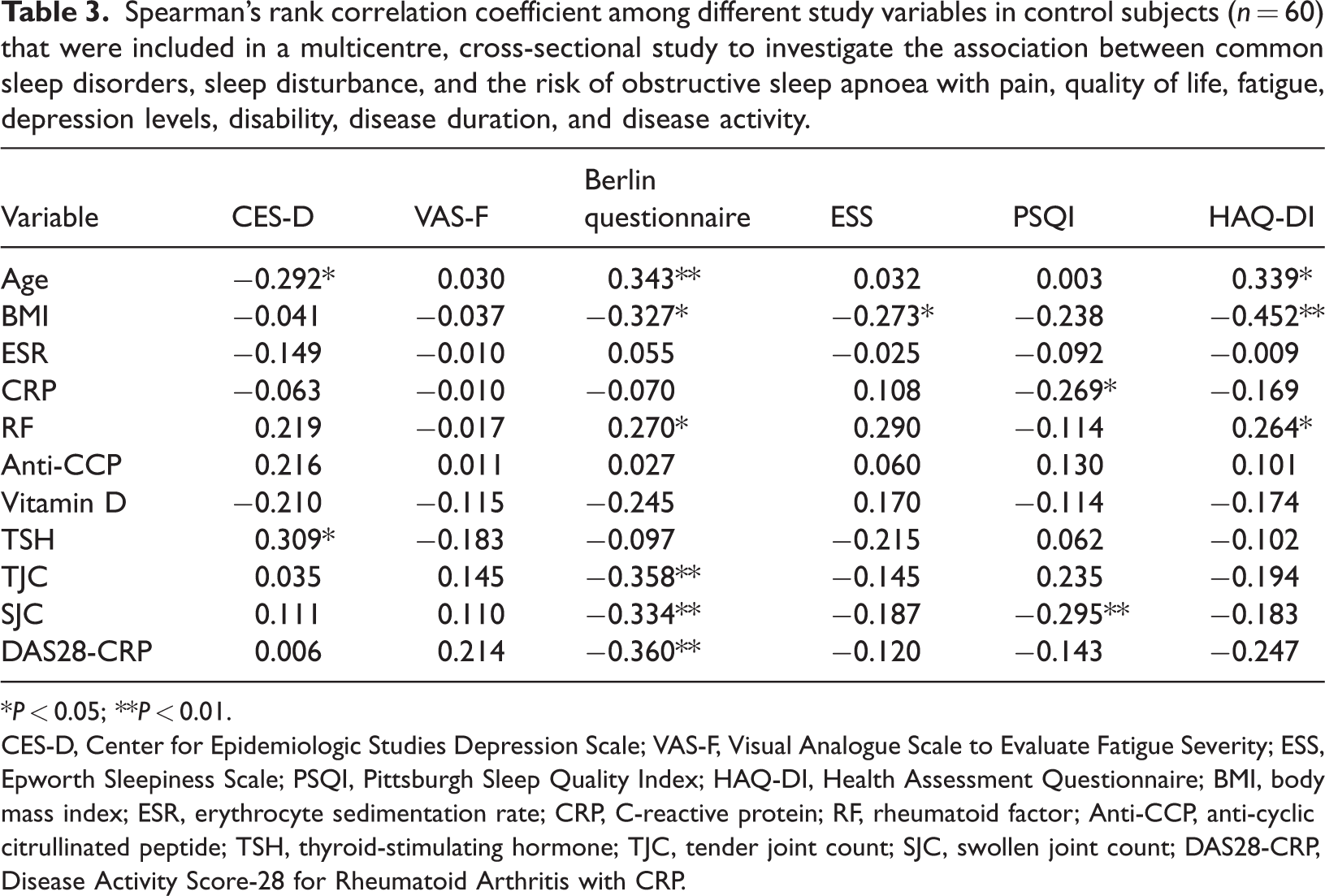
*P < 0.05; **P < 0.01.
CES-D, Center for Epidemiologic Studies Depression Scale; VAS-F, Visual Analogue Scale to Evaluate Fatigue Severity; ESS, Epworth Sleepiness Scale; PSQI, Pittsburgh Sleep Quality Index; HAQ-DI, Health Assessment Questionnaire; BMI, body mass index; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; RF, rheumatoid factor; Anti-CCP, anti-cyclic citrullinated peptide; TSH, thyroid-stimulating hormone; TJC, tender joint count; SJC, swollen joint count; DAS28-CRP, Disease Activity Score-28 for Rheumatoid Arthritis with CRP.
There was a significant positive correlation between PSQI and DAS28-CRP, HAQ-DI scores and VAS-F in patients with RA (P < 0.01 for all correlations) (Table 4). There was a significant difference between the normal and abnormal groups in EDS measured by the ESS among the different educational levels for the study population (P < 0.01) (Table 5). Multiple linear regression was used to test whether disease duration, DAS28-CRP, HAQ-DI and VAS-F significantly predicted the risk of sleep apnoea. The overall regression was significant (R2 = 0.492; P < 0.001), which means that the predictors explained 49.2% of the variance in the risk of sleep apnoea. HAQ-DI (coefficient β = 0.103; P < 0.001) and VAS-F (coefficient β = 0.028; P < 0.001) significantly predicted the risk of sleep apnoea (Table 6). In the second model, the same predictors to predict sleep quality were used and the overall regression was significant (R2 = 0.371; P < 0.001), which means that the predictors explained 37.1% of the variance in sleep quality. HAQ-DI (coefficient β = 0.158; P < 0.001) and VAS-F (coefficient β = 0.077; P < 0.001) significantly predicted sleep quality. The same predictors were used in the third model to predict excessive daytime sleepiness. The overall regression was significant (R2 = 0.448; P < 0.001), which means that the predictors explained 44.8% of the variance in HAQ-DI (coefficient β = 0.158; P < 0.001) and VAS-F (coefficient β = 0.077; P < 0.001) significantly predicted PSQI.
Spearman's rank correlation coefficient between sleep qualities and clinical characteristics in patients with rheumatoid arthritis (n = 247) that were included in a multicentre, cross-sectional study to investigate the association between common sleep disorders, sleep disturbance, and the risk of obstructive sleep apnoea with pain, quality of life, fatigue, depression levels, disability, disease duration, and disease activity.
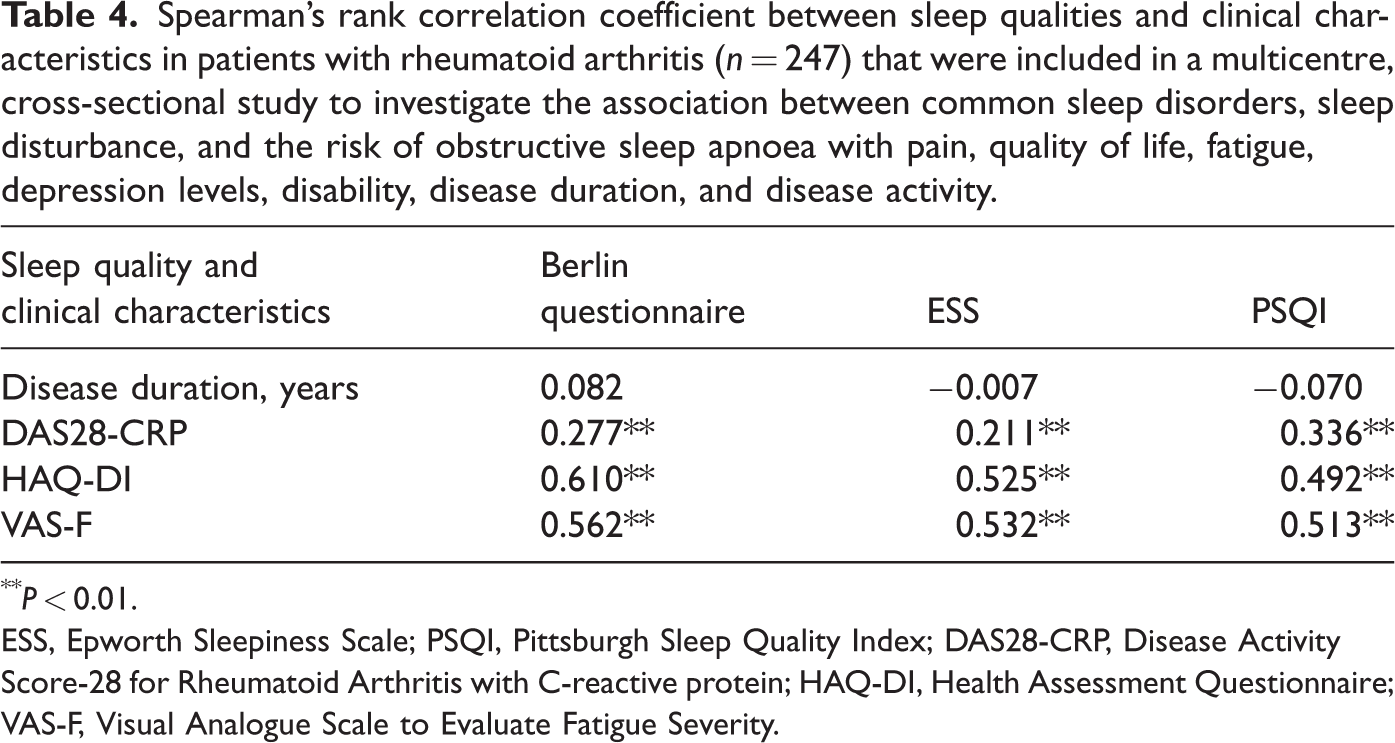
P < 0.01.
ESS, Epworth Sleepiness Scale; PSQI, Pittsburgh Sleep Quality Index; DAS28-CRP, Disease Activity Score-28 for Rheumatoid Arthritis with C-reactive protein; HAQ-DI, Health Assessment Questionnaire; VAS-F, Visual Analogue Scale to Evaluate Fatigue Severity.
Association between demographic data and sleep quality as measured by the Berlin questionnaire, Epworth Sleepiness Scale (ESS) and the Pittsburgh Sleep Quality Index (PSQI) in patients with rheumatoid arthritis (RA) (n = 247) and age- and sex-matched control subjects (n = 60) that were included in a multicentre, cross-sectional study to investigate the association between common sleep disorders, sleep disturbance, and the risk of obstructive sleep apnoea with pain, quality of life, fatigue, depression levels, disability, disease duration, and disease activity.
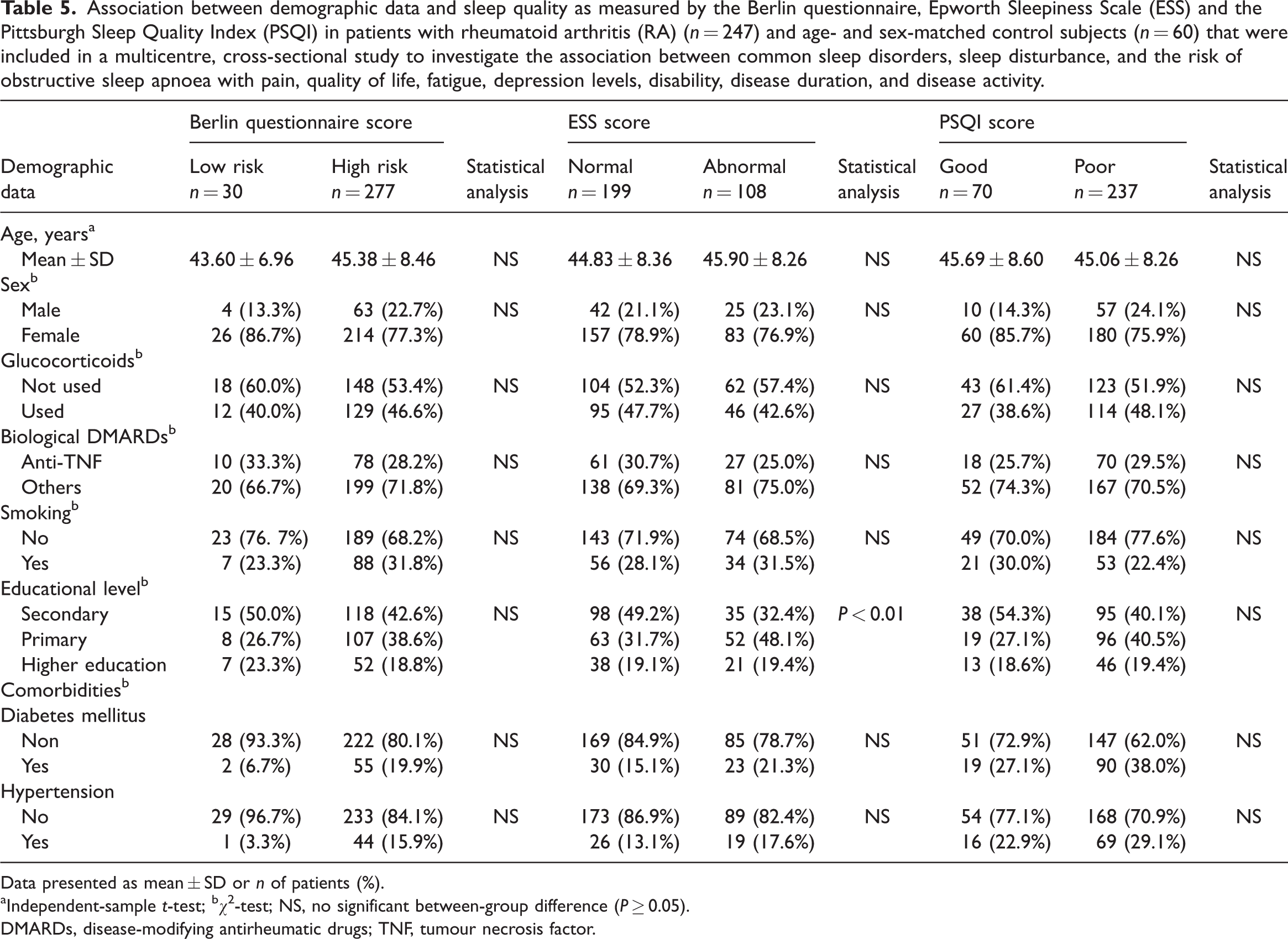
Data presented as mean ± SD or n of patients (%).
Independent-sample t-test; bχ2-test; NS, no significant between-group difference (P ≥ 0.05).
DMARDs, disease-modifying antirheumatic drugs; TNF, tumour necrosis factor.
Multiple linear regression analysis between disease duration, Disease Activity Score-28 for Rheumatoid Arthritis with C-reactive protein (DAS28-CRP), Health Assessment Questionnaire (HAQ-DI) and Visual Analogue Scale to Evaluate Fatigue Severity (VAS-F) as predictors for sleep quality.
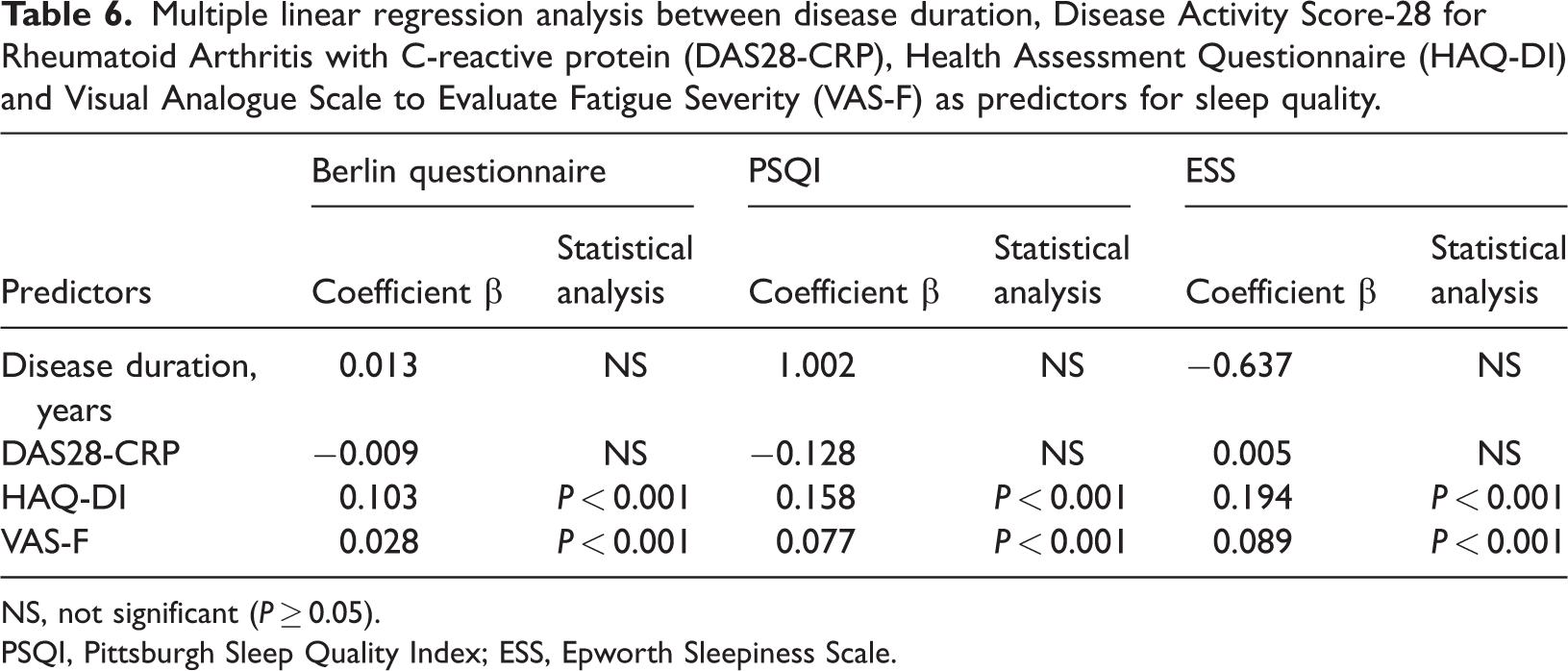
NS, not significant (P ≥ 0.05).
PSQI, Pittsburgh Sleep Quality Index; ESS, Epworth Sleepiness Scale.
Discussion
Rheumatoid arthritis is a disease with systemic manifestations, which include articular and extra-articular manifestations such as depression, pain and fatigue, as well as disturbances of sleep and life. 9 This current study aimed to determine whether sleep quality and common sleep disorders were associated with RA disease activity, pain, stress, depression and quality of life. Many previous studies have demonstrated the association between RA and sleep disturbances. For example, sleep disturbances were claimed to be the underlying aetiology of other disorders, such as fatigue, stress, depression and mood disorders. 20 Sleep disturbance among RA patients includes difficulty falling asleep with frequent awakenings at night, which leads to daytime sleepiness.21,22 Sleep disturbances are experienced in approximately half of RA patients. 23 The current study provides support for such findings, suggesting a significant relationship between RA and poor sleep quality compared with the control group. This is in agreement with a previous study that reported that patients with RA have a high prevalence of nonoptimal sleep. 7 Only one study has demonstrated that sleep problems are independently associated with depression in RA, involving cross-sectional and longitudinal analyses. 10 This previous finding was consistent with the current findings, as there was a significant positive correlation between CES-D and RF, anti-CCP, TJC, SJC and DAS28-CRP scores. These current results are supported by previous research that detected a higher level of depression in RA patients. 24 There are many factors that contribute to the pathogenesis of depression, including the presence of fatigue, which is highly frequent in patients with RA, the burden of the disease itself, and the presence of sleep disturbances. 10 This current study also found that sleep quality in RA patients was affected by pain severity, as evident by a positive correlation between the DAS28-CRP score and the PSQI, ESS, and Berlin questionnaires. This is supported by a study suggesting that pain thresholds can be lowered in both RA patients and the general population. 25 Furthermore, unsatisfactory sleep quality was found in the current study to be associated with high levels of fatiguability, as evident by the strong correlation between PSQI and VAS-F, which is also consistent with previous research. 26 Disability caused by RA can have a catastrophic influence on patients' lives by reducing not only their ability to engage in everyday tasks, but also avocational activities such as playing sports. 27 Recognizing the relationship between RA and sleep disturbances is important for healthcare providers to provide thorough treatment for patients with RA. Overall, the relationship between RA and sleep disturbances is complex, and addressing both conditions is crucial for improving the quality of life of individuals with RA. 25 By recognizing and treating sleep disturbances in patients with RA, healthcare providers might be able to improve their overall health and well-being.
This current study had several strengths, including a representative sample size of 247 RA patients. Furthermore, it included a control group for comparison and collected data on medication use that could contribute to sleep disorders. In addition, multiple questionnaires, including ESS, PSQI, VAS-F, HAQ-ID and CES-D, were used to assess the study participants. BMI was reported as a potential confounder. In addition, a thorough history was collected and a physical examination was performed. Laboratory tests, such as CRP to calculate the DAS28-CRP score that was used to determine the relationship between sleep disorders and disease activity, were undertaken. However, there were some limitations to this current study, including its cross-sectional design, which prohibits causal inferences regarding variable correlations from being drawn. Furthermore, the study did not use a confirmatory test such as polysomnography to identify OSA.
In conclusion, this current study has demonstrated a significant association between RA and poor sleep quality, as well as common sleep disorders. Sleep disturbances in patients with RA include difficulty falling asleep, frequent awakenings and daytime sleepiness. These sleep disturbances have been linked to other disorders such as fatigue, stress, disability, depression and disease activity. The current study highlights the importance of recognizing and treating sleep disturbances in patients with RA, as it may significantly improve their overall health and well-being. Healthcare providers must effectively manage RA symptoms to improve sleep quality and provide comprehensive care for patients with RA.
Footnotes
Author contributions
Wesam Gouda and Mohamed Kamal were involved in the study's design. Reem Alreefi, Taif Alomar and Fatimah Kushk were responsible for the data collection and manuscript preparation. Raghad Alahmadi and Mona Mokhtar were responsible for data analysis and manuscript preparation. Seham A. Elazab, Mayada Khalil, Wesam Gouda and Mohamed Kamal retrieved and analysed the data. Seham A. Elazab and Wesam Gouda wrote the manuscript. All authors reviewed and confirmed the final manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.