
Abstract
Background and objective:
Understanding the mental health impact of the COVID-19 pandemic on persons receiving COVID-19 testing will help guide mental health interventions. We aimed to determine the association between sociodemographic factors and mental health symptoms at 8 weeks (baseline) after a COVID-19 test, and compare prevalence of mental health symptoms at baseline to those at 16-week follow-up.
Materials and Methods:
Prospective cohort study of adults who received outpatient COVID-19 testing at primary care clinics. Logistic regression analyses were used to assess the association between sociodemographic characteristics and COVID-19 test results with mental health symptoms. Mental health symptoms reported at baseline were compared to symptoms at 16 weeks follow-up using conditional logistic regression analyses.
Results:
At baseline, a total of 124 (47.51%) participants reported at least mild depressive symptoms, 110 (42.15%) participants endorsed at least mild anxiety symptoms, and 94 participants (35.21%) endorsed hazardous use of alcohol. Females compared to males were at increased risk of at least mild depressive symptoms at baseline (Adjusted Odds Ratio (AOR): 2.08; 95% CI: 1.14-3.79). The odds of at least mild depressive symptoms was significantly lower among those residing in zip codes within the highest quartile compared to lowest quartile of household income (AOR: 0.37; 95% CI: 0.17-0.81). Also, non-Hispanic Whites had significantly higher odds of reporting hazardous alcohol use compared to non-Whites at baseline (AOR: 1.94; 95% CI: 1.05-3.57). The prevalence of mental health symptoms remained elevated after 16 weeks.
Conclusion and Relevance:
We found a high burden of symptoms of depression and anxiety as well as hazardous alcohol use in a diverse population who received testing for COVID-19 in the primary care setting. Primary care providers need to remain vigilant in screening for symptoms of mental health disorders in patients tested for COVID-19 well after initial testing.
Introduction
The impact of the COVID-19 pandemic on the psychological and mental health of individuals is an ongoing area of intensive study. Recent studies that examined the burden of depression pre and post COVID-19 found a higher burden of depressive symptoms following the pandemic than before.1,2 A study of the prevalence of depressive symptoms showed that individuals having prior mental health risk or exposure to life stressors are at increased risk. 1 In addition, socioeconomic factors were associated with an increased prevalence of depressive symptoms following COVID-19 outbreak. 1 Anxiety, trauma and stress-related disorders, alcohol abuse, and suicidal ideation have also been on the rise since the pandemic began.2-4
As with most disease outbreaks, the direct impact of the disease and resultant physical and mental health symptoms experienced vary disproportionately across different sociodemographic groups.5,6 Certain racial/ethnic minority groups are at higher risk of severe illness due to prevalent comorbidities, lower rate of insurance coverage, and lower access to testing. 7 Also, financial hardship from COVID-19 is worse among Blacks, Hispanics, and lower-income groups. 8 In a recent Morbidity and Mortality Weekly Report, suicidal ideation during the pandemic was higher among young adults, minority racial/ethnic groups, unpaid caregivers, and essential workers. 3
As COVID-19 cases continue to surge across the US with hospitals reaching capacities, several states have ordered businesses, schools, and workplaces to close and enforced community mitigation strategies such as wearing face masks, limitation of mass gatherings, travel bans, and physical distancing.9,10 There is variation in COVID-19 beliefs and compliance with precautionary measures across different sociodemographic and racial groups, which could have implications for decision making.11-13 Understanding the burden of mental health symptoms during the COVID-19 pandemic and how this varies among different sociodemographic groups will help inform public health interventions for the most vulnerable populations.
While a few studies have examined the mental health impact of COVID-19 in the general population,1,3,4,14 little is known about the mental and psychological sequelae among a segment of the population who have been tested for COVID-19 relatively early in the pandemic in the primary care setting. Also, given that this population is already engaged with the healthcare system, it may be easier to provide mental health services to those affected. Using a prospective cohort study design, we examined the association between sociodemographic factors and mental health symptoms at 8 weeks (baseline) after a COVID-19 test was ordered in primary care sites in a large academic group practice, and compared the prevalence of mental health symptoms at baseline to those at 16 weeks follow-up.
Methods
Study Design and Populations
This was a prospective cohort study of adults who had a COVID-19 test at one of the clinics in UT Physicians (the practice plan of McGovern Medical School at UTHealth) in the Greater Houston Metropolitan area, Texas. All patients for whom a COVID-19 test was ordered between March 10th and May 4th, 2020, were divided into weekly cohorts (total of 8 cohorts) with each cohort beginning 8 weeks from their first COVID-19 test order (Supplemental Table 1). This design allowed patients’ responses to be interpreted in context with the rapid changes in COVID-19 policies and epidemic peaks. A total of 790 patients aged 18 years and older received an email invitation to complete an online questionnaire administered through Qualtrics at baseline and 16 weeks later. The questionnaires included a set of psychometrically-validated data collection instruments designed specifically for COVID-19-related behavioral and social science domains by the NIH Office of Behavioral and Social Sciences Research (OBSSR), NIH Disaster Research program (DR2), and PhenX Toolkit. We also used other standard instruments for mental health and other domains. Demographic information including age, gender, race/ethnicity, insurance status, and zip code (as a proxy for income) were also collected. The questionnaires took approximately 15-20 minutes to complete. Participants were offered the incentive of a $20 digital gift card for each questionnaire completed.
All participants received nasopharyngeal nucleic acid amplification testing for COVID-19 after consultation with a triage nurse and a healthcare provider. Most consultations were conducted via telemedicine or telephonic visits. Majority of the tests were ordered by primary care providers. Samples were obtained at our primary care clinics, analyzed at commercial lab facilities and results returned to the ordering provider through the electronic health record (EHR). In 83% of eligible participants, the test ordered date in the EHR was recorded on the test result date. Early in the pandemic, the turnaround time was much longer than it is now. As such, we used the average time (6 days) between the test order date and test result date in the 17% of eligible participants for whom test order date and test result dates were entered separately, as a benchmark to estimate a proxy test order date. Non-responders received up to 2 reminder emails. To further optimize response rates, we made follow-up phone calls to non-respondents on day 15 after the initial email was sent. To minimize bias, the follow-up team was unaware of the patient’s COVID-19 test status.
Measures
COVID-19 test status
COVID-19 test status was dichotomized as either “positive” or “negative.” A positive result was defined as having a positive COVID-19 test as obtained from electronic health records at any point before the respective survey submission.
Depressive symptoms
Depressive symptoms were self-reported and assessed using the Patient Health Questionnaire-9 (score 0-4 = none to minimal, 5-9 = mild, 10-14 = moderate, 15-19 = moderately severe, 20-27 = severe). 15 Depressive symptoms were recategorized as a dichotomous variable, “0-4 = none to minimal” and “5-27 = at least mild depressive symptom.”
Anxiety symptoms
Anxiety symptoms were self-reported and assessed using the General Anxiety Disorder-7 questionnaire (score 0-4 = none to minimal, 5-9 = mild, 10-14 = moderate, ≥15 = severe). 16 Anxiety symptoms were recategorized as a dichotomous variable, “0-4 = none to minimal anxiety” and “≥5 = at least mild anxiety symptom.”
Hazardous alcohol use
Hazardous alcohol use was self-reported and assessed using the AUDIT-C Questionnaire. 17 This was a dichotomous variable, “≥4 = positive for males or ≥3 = positive for females” and “negative” if otherwise.
Sociodemographic characteristics
Sociodemographic characteristics assessed at baseline include age (18-34 years, 35-49 years, 50-64 years, and ≥65 years), gender (male and female), race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, and non-Hispanic American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander or Other). Race/ethnicity was further reclassified as non-Hispanic White and Non-White for analysis to allow for larger sample sizes. Non-White represented all those who self-reported their race/ethnicity as non-Hispanic Black, Hispanic and non-Hispanic American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander or Other. Income was approximated using zip code level median annual household income from the American Community Survey 2006 to 2010, and categorized into quartiles (First quartile: $25 127-$41 755; Second quartile: $41 756-$65 105; Third quartile: $65 106-$93 660 and Fourth quartile: $93 661-$153 649). 18 Age and gender were extracted from EHR while race/ethnicity was self-reported at baseline.
Statistical Analyses
We assessed the prevalence of mental health symptoms stratified by COVID-19 test status and sociodemographic characteristics at baseline and at 16 weeks follow-up using simple proportion and chi-square test. Univariable and multivariable logistic regression analyses were used to assess the association between sociodemographic characteristics and COVID-19 test results with mental health symptoms at baseline. Age, sex, race/ethnicity, median household income, and COVID-19 test result were adjusted in multivariable logistic regression models. Changes in individual scores for depressive symptoms, anxiety symptoms, and hazardous alcohol use at baseline compared to 16 weeks follow-up were presented using a scatter plot. Furthermore, the odds of having mental health symptoms at 16 weeks follow-up compared to those at baseline were estimated using conditional logistic regression analyses. Each conditional logistic regression model was adjusted for COVID-19 test status. All analyses were conducted in Stata/IC V.15.1. 19 Statistical significance was defined as a two-sided P-value <.05 for all comparisons.
Results
A total of 267 participants representing an overall response rate of 33.8% completed the survey at baseline (8 weeks) with a mean (SD) age of 47.07 (16.57) years. The participants were predominantly female (71.54%) and non-Hispanic White (50.39%). The average (SD) median household income for the region of residence of participants was $70 017 ($31 161). At baseline, a total of 33 (12.36%) participants tested positive for COVID-19. There was no significant difference in the distribution by age, sex, and zip code level median household income in those who tested positive compared to those who tested negative for COVID-19. There was a significant difference in the racial/ethnic distribution of COVID-19 test status with 15.63% of non-White having a positive COVID-19 test compared to 7.69% of non-Hispanic Whites (P = .047). Also, at baseline, a total of 124 (47.51%) participants reported at least mild depressive symptoms (PHQ-9 score of 5 or higher), 110 participants (42.15%) endorsed at least mild anxiety symptoms (GAD-7 score of 5 or higher), and 94 participants (35.21%) endorsed hazardous use of alcohol. There was no significant difference in the distribution of mental health symptoms by COVID-19 test status (Table 1).
Distribution of Sociodemographic Characteristics and Mental Health Symptoms of Patients by Covid-19 Test Results at Baseline and at 16 Weeks Follow-Up.

Boldface indicates statistical significance (P < .05).
9 observations were missing for self-reported race/ethnicity. Of the 128 non-Whites at baseline, 57 (44.5%) were non-Hispanic African American, 28 (21.9%) were non-Hispanic American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander or Other, and 43 (33.6%) were Hispanic. Of the 97 non-Whites at follow-up, 39 (40.2%) were non-Hispanic African American, 25 (25.8%) were non-Hispanic American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander or Other, and 33 (34.0%) were Hispanic.
6 observations were missing for depressive symptoms and anxiety.
A total of 52.15% of females endorsed at least mild depressive symptoms at baseline compared to 36.0% among males (P = .018). The prevalence of at least mild depressive symptoms ranged from 33.33% in the highest quartile of income to 56.92% in the lowest quartile of income (P = .016 for the overall trend). In addition, the prevalence of at least mild anxiety symptoms was higher in the younger age groups compared to the older groups (P = .030 for the overall trend) (Table 2).
Distribution of Sociodemographic Characteristics by Mental Health Symptoms at Baseline (N = 267).

Boldface indicates statistical significance (P < .05).
Depression was assessed using PHQ-9 Questionnaire (No = none to minimal depressive symptoms (0-4), Yes = at least mild depressive symptoms (≥5)).
Anxiety was assessed using GAD-7 Questionnaire (No = None to minimal anxiety symptoms (0-4), Yes = at least mild anxiety symptoms (≥5)).
Hazardous alcohol use was assessed using AUDIT-C Questionnaire (No = No hazardous alcohol use (<4 for males and <3 for females), Yes = hazardous alcohol use (≥4 for males and ≥3 for females)).
9 observations were missing for self-reported race/ethnicity.
6 observations were missing each for depressive and anxiety symptoms.
A total of 204 participants completed a follow-up survey at 16 weeks representing an overall response rate of 76.4%. There were 26 (12.75%) participants who had tested positive for COVID-19 at least once by 16 weeks follow-up. We found no significant difference in the distribution of sociodemographic characteristics and mental health symptoms by COVID-19 test status at 16 weeks follow-up. A total of 94 (47.24%) participants reported at least mild depressive symptoms, 87 participants (43.28%) endorsed at least mild anxiety symptoms, and 73 participants (35.78%) reported hazardous use of alcohol (Table 1). At 16 weeks follow-up, the prevalence of at least mild depressive symptoms (53.57%) and at least mild anxiety symptoms (48.25%) was significantly higher in females compared to males (P < .05). While non-Hispanic Whites were less likely to endorse at least mild anxiety symptoms (35.35%) compared to Non-Whites (51.55%) (P = .022), non-Hispanic Whites were more likely to report hazardous alcohol use (45.10%) compared to non-Whites (25.77%) (P = .004) (Supplemental Table 2).
At baseline, the adjusted odds of reporting at least mild depressive symptoms was significantly higher among females compared to males (Adjusted Odds Ratio (AOR): 2.08; 95% CI: 1.14-3.79). Also, the adjusted odds of reporting at least mild depressive symptoms was significantly lower among those residing in regions within the highest quartile compared to the lowest quartile of household income (AOR: 0.37; 95% CI: 0.17-0.81). Sociodemographic characteristics and COVID-19 test status were not associated with the adjusted odds of having at least mild anxiety symptoms. Non-Hispanic Whites had significantly higher odds of reporting hazardous alcohol use compared to non-Whites (AOR: 1.94; 95% CI: 1.05-3.57). The adjusted odds of hazardous alcohol use was significantly lower among the older population ≥65 years compared to those 18-34 years (AOR: 0.34; 95% CI: 0.14-0.83) (Table 3).
Association between Sociodemographic Characteristics and Covid-19 Test Results, and Mental Health Symptoms at Baseline: Logistic Regressions.
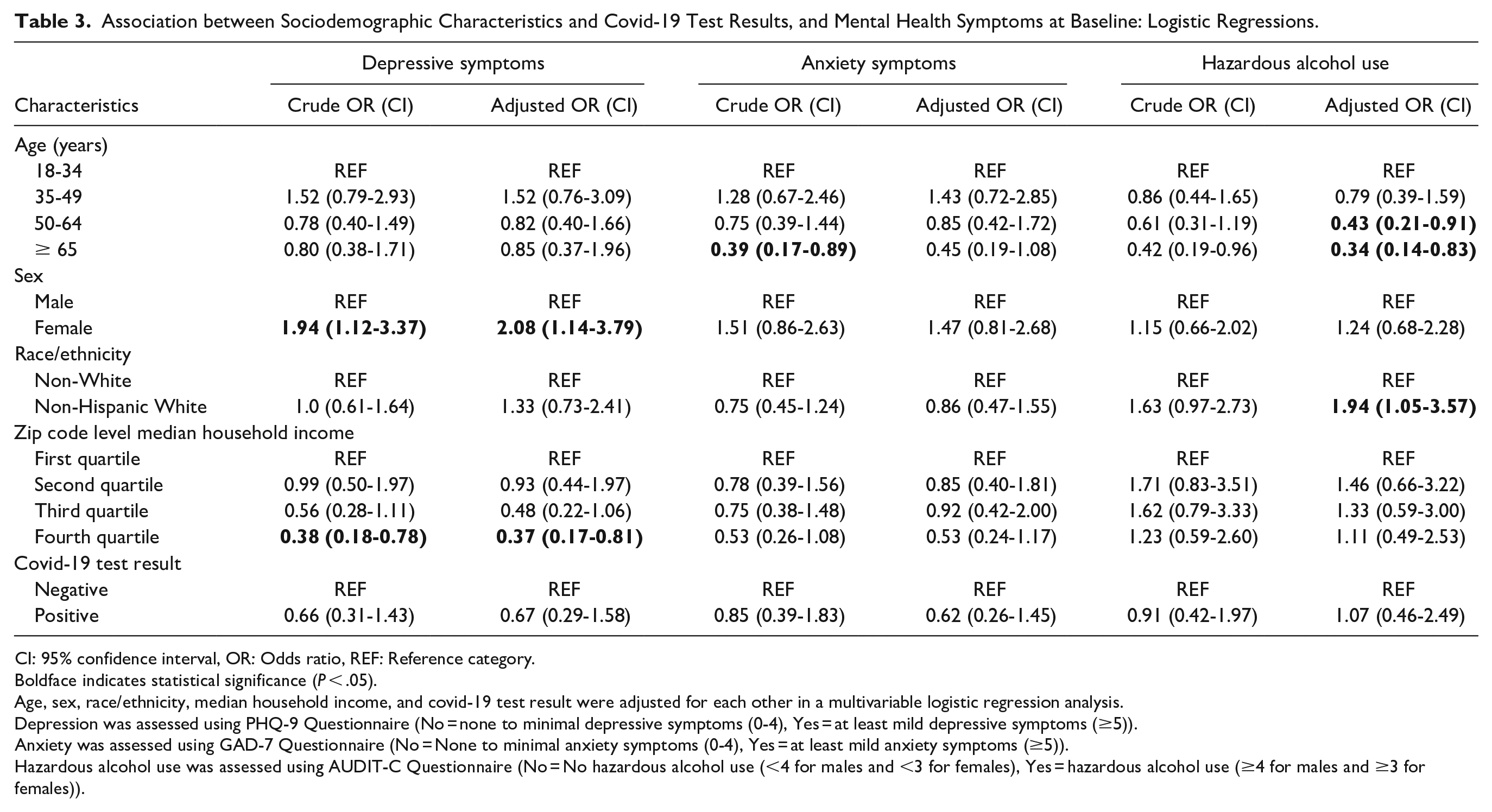
CI: 95% confidence interval, OR: Odds ratio, REF: Reference category.
Boldface indicates statistical significance (P < .05).
Age, sex, race/ethnicity, median household income, and covid-19 test result were adjusted for each other in a multivariable logistic regression analysis.
Depression was assessed using PHQ-9 Questionnaire (No = none to minimal depressive symptoms (0-4), Yes = at least mild depressive symptoms (≥5)).
Anxiety was assessed using GAD-7 Questionnaire (No = None to minimal anxiety symptoms (0-4), Yes = at least mild anxiety symptoms (≥5)).
Hazardous alcohol use was assessed using AUDIT-C Questionnaire (No = No hazardous alcohol use (<4 for males and <3 for females), Yes = hazardous alcohol use (≥4 for males and ≥3 for females)).
We found no significant difference in the odds of reporting at least mild depressive symptoms, at least mild anxiety symptoms, or hazardous alcohol use at 16 weeks follow-up compared to baseline (AOR: 1.06; 95% CI: 0.55-2.01, AOR: 1.17; 95% CI: 0.62-2.19, AOR: 1.20; 95% CI: 0.52-2.78 respectively) (Table 4).
Change in Mental Health Symptoms at 16 Weeks Follow-Up Compared to Baseline: Conditional Logistic Regression.

CI, 95% confidence interval.
Depression was assessed using PHQ-9 Questionnaire (None to minimal depressive symptoms (0-4), At least mild depressive symptoms (≥5)).
Anxiety was assessed using GAD-7 Questionnaire (None to minimal anxiety symptoms (0-4), At least mild anxiety symptoms (≥5)).
Hazardous alcohol use was assessed using AUDIT-C Questionnaire (No hazardous alcohol use (<4 for males and <3 for females), hazardous alcohol use (≥4 for males and ≥3 for females)).
Adjusted odds ratio from conditional logistic regression model adjusted for COVID-19 test result.
There was marked heterogeneity in the change in mental health scores from baseline to follow-up, as depicted in Figure 1. A total of 108 of 194 (55.67%) participants had the same level of severity in depressive symptoms at baseline and follow-up. Among these, 59 participants had none to minimal depression, 21 had mild and 28 (14.43%) had moderate to severe depressive symptoms. On the other hand, 93 of 196 (47.45%) participants had none to minimal anxiety and 25 had moderate to severe anxiety at both baseline and follow-up. Furthermore, 61 of 204 (29.90%) participants reported hazardous alcohol use at both baseline and follow-up (Figure 1 and Supplemental Table 3).
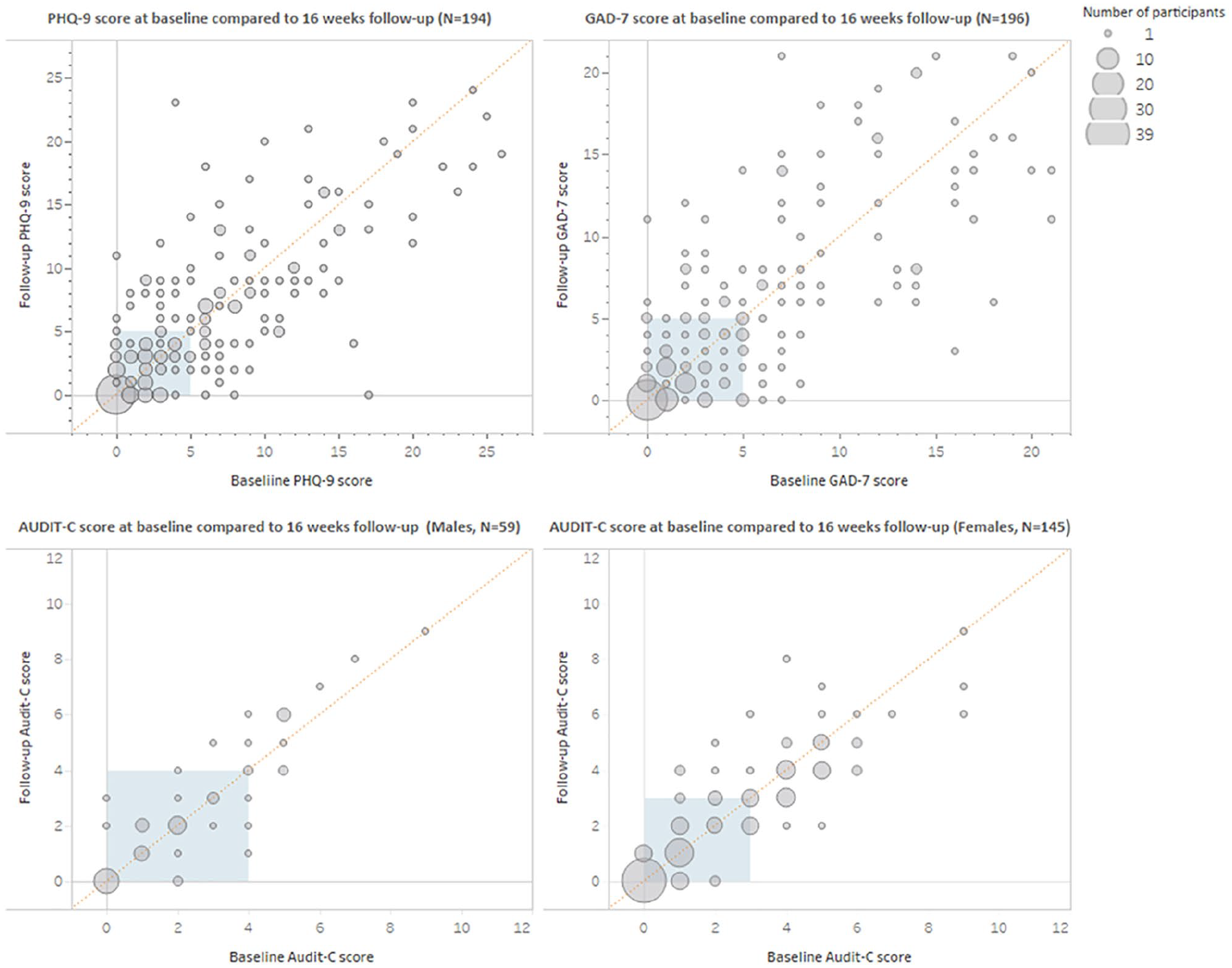
Change in mental health symptoms at baseline compared to 16 weeks follow-up.
Discussion
Our study found that among 267 participants who sought COVID-19 testing in the primary care setting, at 8 weeks after the test (baseline), a significant portion reported depressive symptoms, anxiety symptoms, and hazardous use of alcohol. Even 16 weeks after initial testing, the prevalence of these conditions did not change. Findings from our study are similar to reports from other population-based studies that assessed the burden of mental health symptoms during the COVID-19 pandemic.1,4,20 This finding is not surprising given the physical and socio-economic disruptions faced by individuals, families, and communities since the pandemic began. 21 Unemployment rates, housing instability, and food insecurity have soared with untold consequences on the mental well-being of individuals.8,21 However, Czeisler and colleagues found a lower prevalence of anxiety (25.5%) and depressive symptoms (24.3%) in the general U.S. population during the COVID-19 pandemic compared to what we found from our study. 3 The high prevalence of mental health symptoms seen in our study may be due to additional stress and anxiety associated with getting tested and the possibility of a positive test result. These findings call for increased mental health screening in the general U.S. population, and particularly among persons getting tested for COVID-19.
We found a high burden of hazardous alcohol use among our study participants. Other studies have reported a high rate of problematic alcohol use as a response to stress and as a coping mechanism following a major life event.22-25 For example, almost 25% of New York residents reported increased alcohol use following the attack on the World Trade Center in 2001. 26 A link between anxiety and depressive symptoms and an increase in harmful alcohol use has been documented previously. It has also been found that following a traumatic event, persons with mental health symptoms are more likely to indulge in hazardous alcohol use compared to those with no mental health symptoms.27-29 Similarly, a recent study conducted in the US found that during the COVID-19 outbreak, persons with anxiety or depression were more likely to indulge in harmful alcohol use. 29 Boredom and lack of routine following COVID-19 mitigation strategies including quarantine and isolation have been associated with the increased alcohol consumption seen during the pandemic. 24 However, it is argued that the increased alcohol use seen after a disaster may be more among individuals with a pre-existing history of alcohol abuse or psychological disorders. 30
Our study found that those aged 65 years and older were less likely to indulge in hazardous alcohol use during the pandemic compared to those aged 18 to 34 years. This is similar to what was reported following previous disasters, and reports from a recent study during the COVID-19 pandemic, with all showing a higher prevalence of harmful alcohol use among the younger age group.26-28 It is well established that females are twice as likely to be depressed than males.31-33 Our study, similar to other studies conducted during the pandemic, supports this theory of a gender difference in the prevalence of depressive symptoms. 34 Several factors ranging from biological, psychological, and environmental factors at the micro and macro levels have been linked with the gender difference in depression. 33 Furthermore, we found that those in the highest socio-economic quartile are less likely to endorse depressive symptoms. This may be related to the disproportionate impact of the pandemic with persons in the lowest socio-economic groups lacking fundamental necessities and access to healthcare such as counseling services for mental well-being.6,35 The sociodemographic differences in mental health symptoms and hazardous alcohol use seen in our study highlights the need for targeted policies and interventions during the pandemic and even long after the pandemic is over.
We did not find a significant overall change in mental health symptoms over the 16 weeks of follow-up. This may suggest a heavy psychological toll felt by patients even months after receiving their test results. Following the Severe Acute Respiratory Syndrome (SARS) outbreak in 2003, the cumulative prevalence of depressive and anxiety disorders among SARS survivors remained elevated up to 30 months after the outbreak with depressive disorders persisting in 15.6% of survivors. 36 Moreover, the difference in mental health symptoms between baseline and follow-up in our study may have been obscured by the overlapping period between first wave and second wave of the outbreak. Furthermore, though we found no difference overall between both time points, we observed changes in the severity of mental health symptoms at individual levels which may demonstrate differences in individual resilience and coping mechanisms.
Our study is important in that it provides insights regarding the prevalence of mental health symptoms among individuals undergoing testing for COVID-19. As such, it highlights an opportunity to engage patients and provide mental health services proactively. Notably, the longitudinal nature of the study design allowed us to compare changes in mental health symptoms over time. However, our findings may not be generalizable to populations outside of our geographic area since different areas of the U.S. experienced surges in COVID-19 incidence and testing at different times.
In conclusion, our study found a high burden of symptoms of depression and anxiety as well as hazardous alcohol use in a diverse population who received outpatient testing for COVID-19 at an academic primary care system. These findings warrant increased mental health screening, targeted psychological interventions, and policies to address the burden of mental health symptoms during and after the pandemic. Often being the first contact a patient has with a health care system, primary care providers play a vital role in addressing the psychological fallout of the ongoing pandemic by administering frequent screenings and prompt intervention including referrals to their mental health colleagues. Future studies should explore whether the increase in mental health symptoms seen during the pandemic is more prevalent among those with prior history of psychiatric or behavioral disorders.
Supplemental Material
sj-docx-1-jpc-10.1177_21501327211027100 – Supplemental material for Prevalence and Factors Associated With Mental Health Symptoms in Adults Undergoing Covid-19 Testing
Supplemental material, sj-docx-1-jpc-10.1177_21501327211027100 for Prevalence and Factors Associated With Mental Health Symptoms in Adults Undergoing Covid-19 Testing by Ikponmwosa Osaghae, Linh K. Nguyen, Tong Han Chung, Olivia Moffitt, Yen-Chi L. Le, Mark B. Suh, Pooja N. Prasad, Eric J. Thomas, Christine D. Gordon and Kevin O. Hwang in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by UTHealth and the Center for Clinical and Translational Sciences (CCTS) as well as the Centers for Medicare and Medicaid Services (CMS) funded Texas Delivery System Reform Incentive Payment (DSRIP) Program under the Medicaid 1115 Waiver.
Ethical Approval
The study was approved by the UTHealth Committee for the Protection of Human Subjects (study HSC-MS-20-0410).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.