
Abstract
Introduction:
The COVID-19 pandemic has had a devastating worldwide effect on mental health. Recent studies correlate the spreading of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with symptoms of depression, most prominent in postpartum women. Our systematic literature review scope is to identify the risk factors and predictors for postpartum depression (PPD) and describe the steps that should be taken to help postpartum women. This study will help clinicians, researchers, and policymakers to elucidate the predictors of PPD during this pandemic and prevent these adverse outcomes in future crises.
Methods:
We conducted a systematic search by employing databases PubMed, Google Scholar, Scopus, and Embase to identify articles published before March 2021. About 463 publications were generated during our search process and from those, 36 were reviewed, summarized, and synthesized. Studies qualified the criteria if they (1) utilized qualitative or quantitative design, (2) explored the risk factors for PPD, and (3) were written in English. Quality evaluation of each study was achieved by using criteria set by Lincoln and Guba.
Results:
Prevalence of depression symptoms ranged from 7% to 80.8% in postpartum women during the SARS-COV 2 pandemic. The risk factors for PPD were classified into 6 major categories: socio-demographic, psychological, pre-existing pathology, metabolic factors, previous events of miscarriage, and media misinformation.
Conclusion:
It is extremely vital to care for women’s mental health during pregnancy and after childbirth during these unprecedented times. This review urges the need to design adequate interventions for this vulnerable population to prevent negative consequences of PPD.
Introduction
Coronavirus disease is caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), a virus belonging to the Coronaviridae family. The COVID-19 pandemic, which began to spread worldwide in early 2020, has led to a myriad of unexpected challenges, affecting people physically, mentally, emotionally, and economically. Many of the hard-hit countries have taken very stringent measures, such as total lockdowns, in an attempt to limit the spread of SARS-COV-2. The lack of general support during these tough times due to social distancing and quarantine measures, the stigma associated with the virus, and a prevailing sense of fear and uncertainty have caused or worsened mental health issues such as depression, anxiety, stress, frustration, phobias, obsessive-compulsive symptoms, and post-traumatic stress disorder (PTSD) among the general populations. 1
Essentially, people worst affected by the adverse mental and psychological effects of this pandemic are those with pre-existing physical or mental health problems, the elderly, victims of sexual violence, people going through domestic or substance abuse, people living in poverty, refugees, and immigrants, and hospitalized patients. 2 Another major group significantly affected by the pandemic is pregnant and postpartum women. The process of childbirth in itself encompasses many biological, psychological, and social adjustments. That, coupled with the emotional distress brought on by the COVID 19 pandemic puts postpartum females at an increased risk of mental health issues, especially depressive symptoms.
Postpartum depression (PPD) is the depression suffered by a mother following childbirth, typically arising from the combination of hormonal changes, psychological adjustment to motherhood, and fatigue; postnatal depression. 3 The CDC reports that about 1 in 8 women experience symptoms of PPD in the USA. 3 Although there has been a multitude of developments in the management of PPD, it is still an underdiagnosed condition. In 2014, a US survey of 1400 women revealed that 40% of people with symptoms of PPD did not seek help and the reasons cited for the same were shame, guilt, and stigma of mental illness. One of the main reasons cited for underreporting was the stigmatization of mental illness during the COVID-19 pandemic was the barrier to diagnosis and treatment. 4 PPD not only impacts the mother’s life and overall functioning but also was noted to increase the odds of delays in language skills, including the production of voices in dialog (OR = 1.86, 95% CI: 1.39-2.49) and speaking 2 to 3 words (OR = 1.22, 95% CI: 1.13-1.35) in children. PPD is also associated with 1.5 times increased odds of delays in personal-social skills.5,6
This systematic review assesses the effect of the COVID-19 pandemic on the mental health of postpartum women, with a focus on the risk factors during the pandemic that increased levels of depression in new mothers.
Methods
Literature Search
Literature review related to postpartum depression was examined through a search of peer-reviewed articles and followed PRISMA guidelines. 7 The databases PubMed, Scopus, Google Scholar, and Embase were searched by using the following terms: “COVID 19,” “Sars-Cov-2,” “Coronavirus,” “Postpartum Depression,” “Postpartum,” “Postpartum depression lockdown.” In total, 463 publications were generated during our search process. The titles and abstracts of all records were reviewed to determine if they met inclusion criteria. Authors S.U and S.J screened all abstracts and full texts for eligibility.
Inclusion and Exclusion Criteria
Inclusion criteria were (1) Covid 19 pregnancy, (2) Mental health impacts during the postpartum period, pp depression, pp blues, (3) Observational Studies, RCTs, (4) Articles in English, and (5) No limitation to age, country. We omitted systematic reviews, meta-analyses, letters to editors, and commentaries.
Review and Data Extraction
Three reviewers (S.U, E.G, W.S) independently extracted data about studies, and the articles that met inclusion criteria were reviewed in full and the following data were extracted, if available: (a) socio-demographic indicators; (b) psychological factors; (c) pre-existing pathologies; (d) metabolic factors; (e) previous miscarriage; and (f) media coverage. The assessment was done at the study level and focused on the main study outcome.
Quality Evaluation
Quality evaluation was achieved by using criteria set out by Lincoln and Guba (1985). 8 Each study was evaluated on the degree of credibility, transferability, dependability, confirmability. We used a 1- to 5-point scale for the process of evaluation; with 1 indicating very little confirmation to support the criterion and 5 indicating strong confirmation to support the criterion. This process was done independently by 4 different authors.
Results
Of the 463 studies initially identified during the search process, 36 studies were included in this systematic review (Figure 1). All the included studies were observational, ranging from cross-sectional to cohort studies.
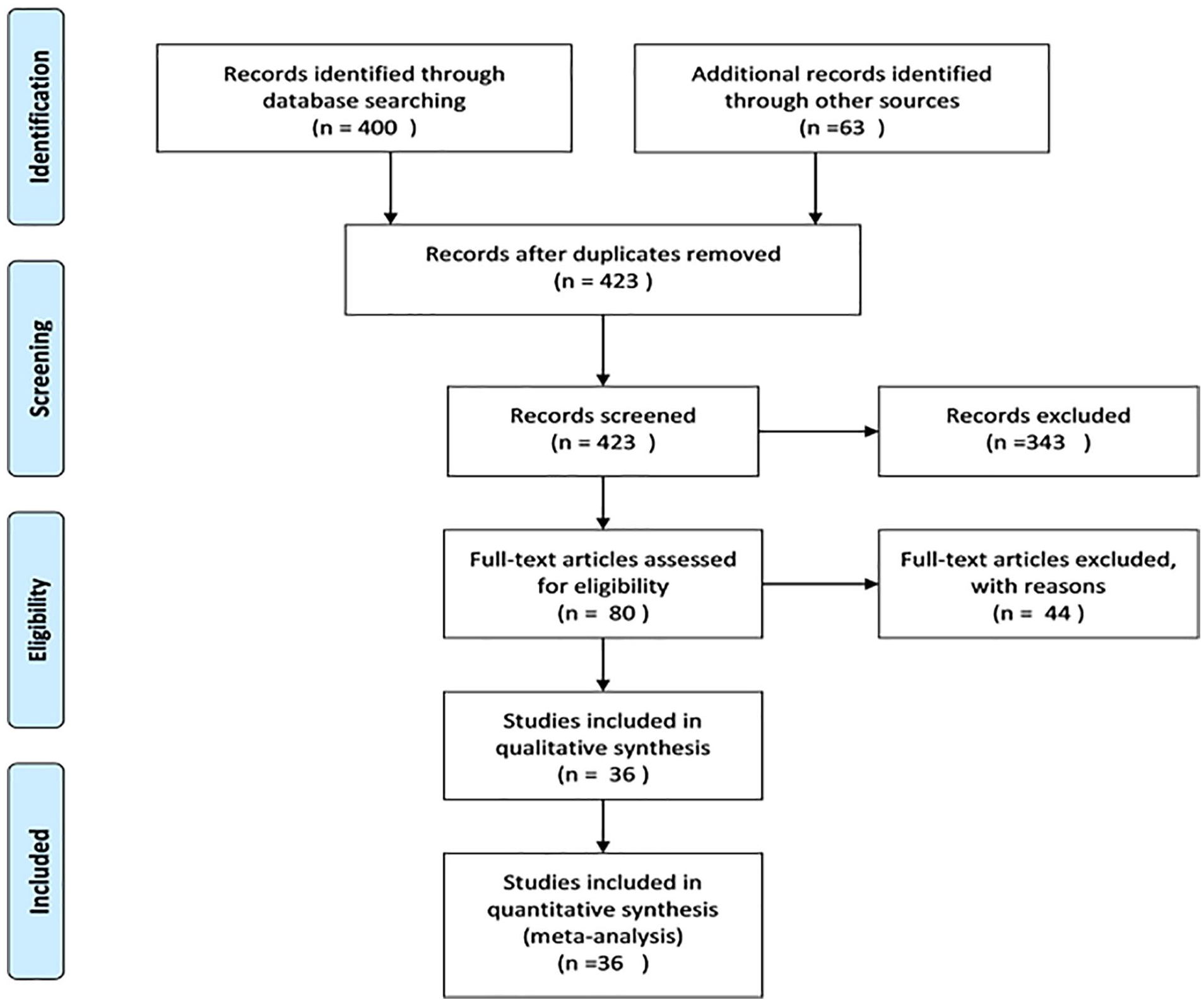
PRISMA flowchart.
The total number of women identified was 35 424 in number (Table 1). The highest representation of countries was noted for the United States (n = 8), followed by Turkey (n = 5), and Italy/China (n = 4) (Figure 2).
Characteristics of included studies.

Abbreviations: A.P, after pandemic; B.P, before pandemic; P, prevalence; PPD, postpartum depression; SZ, sample size.
EPDS (The scale has 10 self-reported questions, rated on a 4-point Likert scale which are scored from 0 to 3. The scale is scored between 0 and 30 and the cut-off point of 13 or higher scores are considered as the probable risk for the presence of postpartum depression); PHQ (Patient Health Questionnaire score is 16. Scores of 5, 10, 15, and 20 represent cut points for mild, moderate, moderately severe and severe depression, respectively. Sensitivity to change has also been confirmed.).

Countries of origin for all included studies.
Our study has explored (1) the mean level of depressive symptomatology of post-partum women over time, (2) the prevalence of depression after the postpartum period, (3) risk factors that predict the course of PPD (Table 2).
Risk Factors for postpartum depression during the COVID-19 pandemic.

Mean Level of Depressive Symptomatology
Nine studies12,16,18,23,26,32,38,42,46 (Table 1)—explored mean depression levels in the postnatal period. Follow-up in these studies ranged from 4 weeks to 3 months. One study 34 found that there is a statistically significant decrease, while in contrary 5 studies14,24,29,34,39,46 described a decrease but did not calculate statistical significance. In 5 studies,18,23,26,32,38,42 the mean level of depression decreased to below the cutoff value for depression defined in each study.
In conclusion, depression levels do not always decrease below the cutoff, however, the decrease is not always statistically significant. In addition, the standard deviations are relatively high, which represent a change in depression levels within a sample is highly variable, proposing that depressed mothers cannot be considered a homogeneous group.
Prevalence of PPD Period
Studies suggest that 14.8% to 40.7% (median = 35%) of mothers with PPD still met criteria for major depression with EPDS > 13 at less than 3 month (n = 8 studies12,16,18,20,21,23,28,38 ); 27.4% at 1 week (n = 1 study 30 ) 38% to 44% (median = 39%) at 1 month (n = 3 studies6,40,41); 30% to 39% (median = 36%) at 4 to 12 weeks (n = 3 studies15,24,47); 12% to 36.3% (median 23.3%) at 2 months (n = 4 studies4,27,32,44 ); and 30% to 80% (median = 33%) at 3 months (n = 6 studies4,14,22,26,42,46); 9.6% to 60% (median = 27%), duration of months is not applicable (n = 11 studies13,17,19,25,29,34,39,43,45,46), 12.4% at <5 months (n = 1 study 22 ). Overall, these findings suggest that at any time point between 1 week and <5 months postpartum, about 27% of mothers diagnosed with PPD still meet criteria for depression.
Risk Factors That Predict the Course of PPD
Various risk factors were identified across the included studies. These included first, sociodemographic risk categories, addressing (1) low income, (2) self/partner unemployment due to COVID-19, (3) immigrant status, (4) women in Western and Central China, and (5) participants of color (Black, Asian, Multiracial, and/or Hispanic/Latinx). Second, psychological risk categories addressing (1) concerns about self/family contracting COVID-19/COVID-19 lockdown/strict COVID-19 protocols, (2) worrying about the future, (3) perceived pain during birth; childbirth stress, (4) poor social support; no close family member or spouse, (5) perceived stress, (6) social isolation/social distancing/loneliness, and (7) dismissive and fearful-avoidant attachment styles/emotional stressors. Third, pre-existing pathologies including (1) pre-existing psychiatric illness, and (2) maternal disability. Fourth, metabolic factors including (1) BMI/Obesity, (2) age group of 33 to 36, (3) age >35, (4) smoking, and (5) fever. Fifth, previous events such as a history of abortion. Sixth, misinformation due to social media. Finally, other factors such as (1) postponed/canceled medical appointments, (2) relationship with spouse, and (3) unplanned pregnancy (Table 2).
Discussion
During the early months of the pandemic, not much was known about the management strategies for pregnant and postpartum women. With most of the medical resources being directed toward the care of COVID-19 infected patients, there was uncertainty among pregnant women and new mothers of receiving timely care.
Childbirth is noted to be a challenging journey for a woman as there are abrupt and dramatic changes in the woman’s body physiologically as well as anatomically. The potential role of hormonal variations on a woman’s mood in the postpartum period, particularly considering estrogen, progesterone, testosterone, prolactin, and thyroxine has been studied. It is noted that roughly about 14% of women experience depressive moods during the early postpartum period. Women have reported having noticed the peripartum mood changes from the time of the onset of delivery up to 4 weeks of postpartum. It is during this period where women are at heightened vulnerability to feel depressed. The spectrum of peripartum mood changes varies from the mother feeling fatigued, tearful, and being overwhelmed with the unfolding of new responsibilities.9,28
A review of our selected studies found that some common risk factors for developing PPD or anxiety included maternal factors like preexisting chronic autoimmune diseases, gestational diabetes, preeclampsia, 10 histories of abortion or pregnancy loss,6,13,14 higher maternal age,15,16 obesity, 17 events of the pregnancy being unplanned. 18
A history of mental illness was also strongly associated with developing postpartum depression, anxiety, or PTSD.19,20 It was observed that mothers with lower social support from family or friends, single mothers, strained marital relationships, 17 higher number of children,15,21 immigrants, lower-income families,16,20,22 and working women, 23 victims of domestic abuse or who do not have access to protective services also had higher levels of PPD and anxiety.6,24
Complications during delivery or admission of newborn to the neonatal intensive care unit,6,20 lack of support in breastfeeding, 25 early use of formula, 12 were also associated with higher levels of PPD and anxiety.
The COVID-19 pandemic has also had an impact on the mental health of new mothers. Mothers who were infected by the virus during the peripartum or postpartum period, or who lived with or were in close contact with people infected with COVID-196,15 showed higher levels of PPD and anxiety. It was observed that these fears were exacerbated by excessive information from external sources like social media messages, news, or well-meaning friends and family found that increased media consumption led to increased levels of anxiety.26,27
The effect of lockdowns and social distancing during the pandemic has also played a role in the higher-than-normal levels of mental health issues in new mothers. Reduced physical activity during pregnancy, 28 boredom, and feeling of isolation, 29 loss of job or housing, 6 missing medical appointments due to lack of transport or city shutdowns, fear of visiting hospitals during the pandemic, lack of a support person during delivery, changes in delivery plan, worrying about family being unable to visit after delivery, absence of childcare facilities, lack of postpartum health care, have all contributed to increased anxiety and depressive symptoms in postpartum women. 26
The fear of the baby or themselves contracting the virus in the hospital was a common cause of PPD and anxiety found in multiple studies.21,29-31 On the other hand, the show of support, empathy, and kindness by the attending hospital staff and the ability to rest due to quietness in the wards are protective against depression. 4
Our review also found, that in contrast, Boekhorst et al 32 reported that during the pandemic, higher levels of maternal stress during pregnancy were found, but there was no increase in depressive levels during pregnancy, nor any increase in stress or depressive levels in the postpartum period. Pariente et al and Silverman et al also found that delivering during the COVID-19 pandemic was independently associated with a lower risk of postpartum depression. Hiiragi et al found no apparent increase in maternal psychological stress due to the COVID-19 pandemic in Yokohama, Japan. A study conducted in China by Zhou et al even found that pregnant women show less depression, anxiety, insomnia, and PTSD symptoms than non-pregnant women during the pandemic.10,22,32-34
Postpartum depression is still a poorly addressed medical issue, as the emphasis is laid mostly on the health of the newborn child. However, if not rightfully addressed, it could cause detrimental effects in both the mother and the child. Depressed new mothers are less sensitive to their infant’s needs which in turn negatively affects mother-child bonding and breastfeeding. 6 This could impact both the short-term and long-term development of the child. Postpartum depression causes parenting difficulties and adverse outcomes for early child development, which again negatively impacts the mental health of the mother. 35
In addition to this, children born to mothers with postpartum depression are reported to be at increased risk of developing anxiety or major depressive disorder in the later parts of their adult life. The mothers are also at increased risk of developing postpartum psychosis characterized by hallucinations, delusions, and thoughts of harming the baby or self. Post-partum psychosis could require emergency hospital admission and inpatient care. 11
It is advised that good social support from the family along with a follow-up to assess for a possible major depressive disorder is recommended. However, as noticed with most psychiatric illnesses, the new mother fears talking about their depressed moods or seeking help. This puts them at an increased risk of progressing to a major depressive disorder (MDD) with peripartum onset.
Health workers may conduct early screening and interventions for postpartum women who are at an increased risk for postpartum depression. New mothers should be encouraged to discuss their mental state and seek help for any symptoms of depression or anxiety. Efforts must be made to destigmatize postpartum depression or anxiety. Mental health screenings should be adapted to the current situation. Currently, some women have chosen remote medical services, such as telemedicine, as a more feasible way to communicate with their health care providers during the postpartum period. While this serves as an important and useful option for patients, it can have disadvantages, such as poor service experience or barriers to physical examination. 36 Patients should also be advised to set up different pathways of receiving support from their family and friends who cannot necessarily be present physically. Virtual meetings or support groups that could include friends, family, or even other new mothers.
While certain lifestyle changes during the COVID-19 pandemic brought impositions that led to increased anxiety and depressive symptoms, some studies suggested these changes had positive outcomes as well. Despite having a sudden change in priorities and social limitations, many new mothers reported enjoying the slower pace, increase in family time, and the opportunity to get more rest. With the stay-at-home orders in place, some women expressed an appreciation of having more time with their partners and the extra help around the house. Virtual technology also provided support to some new mothers, by gaining social support from family and friends using social media and meeting other pregnant and postpartum women online to share experiences. Women even reported using certain available resources such as virtual mental health services, obstetric/pediatric providers, lactational specialists, and others. 27
Conclusion
Our literature review’s purpose was to identify risk factors for anxiety and postpartum depression in women during the SARS COV-2 pandemic. The mental health impacts of the pandemic are of great concern in postpartum women as it affects the wellness of not just the woman herself but the family and her children. Observing these challenges and incorporating changes in our healthcare system can serve as guidelines for incidents like these in the future. Social support for pregnant and postpartum women can play an important role in dealing with depression and anxiety. It is also important to strengthen the knowledge of ways to improve maternal health services during the pandemic. This will help facilitate mental health screening for postpartum women and promote maternal and child health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.