
Abstract
Background:
To characterize the experience of converting a geriatrics clinic to telehealth visits in early stages of a pandemic.
Design:
An organizational case study with mixed methods evaluation from the first 8 weeks of converting a geriatrics clinic from in-person visits to video and telephone visits.
Setting:
Veteran’s Health Administration in Northern California Participants Community-dwelling older Veterans receiving care at VA Palo Alto Geriatrics clinic. Veterans had a mean age of 85.7 (SD = 6.8) and 72.1% had cognitive impairment.
Intervention:
Veterans with face-to-face appointments were converted to video or telephone visits to mitigate exposure to community spread of COVID-19.
Measurements:
Thirty-two patient evaluations and 80 clinician feedback evaluations were completed. This provided information on satisfaction, care access during pandemic, and travel and time savings.
Results:
Of the 62 scheduled appointments, 43 virtual visits (69.4%) were conducted. Twenty-six (60.5%) visits were conducted via video, 17 (39.5%) by telephone. Virtual visits saved patients an average of 118.6 minutes each. Patients and providers had similar, positive perceptions about telehealth to in-person visit comparison, limiting exposure, and visit satisfaction. After the telehealth appointment, patients indicated greater comfort with using virtual visits in the future. Thirty-one evaluations included comments for qualitative analysis. We identified 3 main themes of technology set-up and usability, satisfaction with visit, and clinical assessment and communication.
Conclusion:
During a pandemic that has limited the ability to safely conduct inperson services, virtual formats offer a feasible and acceptable alternative for clinically-complex older patients. Despite potential barriers and additional effort required for telehealth visits, patients expressed willingness to utilize this format. Patients and providers reported high satisfaction, particularly with the ability to access care similar to in-person while staying safe. Investing in telehealth services during a pandemic ensures that vulnerable older patients can access care while maintaining social distancing, an important safety measure.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a novel virus that causes COVID-19 infection, has created a worldwide pandemic disproportionately killing older adults. Recent studies have shown that more than 80% of deaths among adults occurred in those 65 years old and older. 1 Additionally, this virus causes poorer outcomes for those with multiple medical comorbidities. Since a large percentage of older adults also have multiple medical comorbidities, they are particularly at risk for adverse outcomes and severe illness from COVID-19. 1 The Centers for Disease Control and Prevention 2 recommends that older adults limit in-person interactions with others, especially indoors, in addition to social distancing, wearing masks, and practicing good hand hygiene. In order to limit in-person interaction with others, telemedicine is the safest way to deliver necessary medical care. However, little is known about the experience of providing geriatric primary care via telemedicine, with the extant studies focusing on specialty care.3-5
Many challenges arise when offering telemedicine to geriatric populations. Older adults are less likely to have access to technology and may lack fluency in the use of devices.6,7 High prevalence of cognitive and sensory deficits may make technology use more difficult. 8 Moreover, the current pandemic precludes the use of successful telemedicine models including direct installation of telehealth equipment in patients’ homes 9 and hub-and-spokes models, where central “hub” sites provide telemedicine consultation to “spoke” facilities that have telemedicine capable equipment. 10
Despite these challenges, many older adults have positive attitudes toward telemedicine 9 and interest in adopting new technologies when usefulness and usability outweigh feelings of inadequacy. 11
Thus, these studies conducted in non-crisis settings give reason for optimism regarding conducting telemedicine visits with complex, frail older patients. 12 In March 2020, COVID-19 necessitated immediate expansion of telemedicine practices. This paper documents the experience of providing telemedicine care from the patient and provider perspectives in the early months of the pandemic. Specifically, we examine the feasibility and acceptability of telemedicine visits for primary care and geriatrics consultation in complex older patients with a high proportion of cognitive impairment.
Methods
Design
This qualitative improvement (QI) project was conducted within an outpatient geriatrics clinic in a Veterans Health Administration (VHA) facility in northern California between March 9, 2020 and May 5, 2020. The project utilized quantitative and qualitative feedback gathered from patients or caregivers after participation in a telemedicine appointment, as well as from the multidisciplinary clinical team members delivering the care to these patients. The Institutional Review Board at Stanford University determined that this QI project was not human subjects research. A concurrent mixed methods evaluation was conducted.
Participants
This case study was conducted in the outpatient geriatrics primary care clinic at VA Palo Alto in Palo Alto, California, a small, academic teaching clinic for geriatric medicine fellows, medical residents, and other associated health trainees which serves a frail, elderly population. Participants in this case study included older patients who received geriatrics primary care or geriatric consultative care from this VA geriatrics clinic. The sample drawn from the 2 clinics was aged 72 years or older, with 68% of participants over age 85 years old.
Procedures and Measures
Face-to-face appointments were converted to VA Video Connect (VVC) video or telephone visits due to California’s shelter-at-home guidelines to mitigate community COVID-19 spread. Appointments were scheduled as phone or video appointments based on patient preference and video capability. Patients elected to either have phone or video appointments, not both. Phone and video appointments were the same length of time as typical in-person visits. Figure 1 displays procedures employed to prepare patients for the visits. Providers documented access to technology and whether the patient needed caregiver assistance in connecting to the appointment.

Procedures employed to prepare patients for visits.
After the visit, patients or caregivers were invited to complete an optional, 7-question survey about their experience, which was developed for this QI project. If the patient or caregiver agreed to complete the survey, they were asked the extent to which they agreed with statements about how conversion to telemedicine affected access to care, perceived similarity to in-person visits, perceived benefit from limiting in-person exposure, comfort of telemedicine use, and visit satisfaction. Responses were rated on a scale from 1 to 5, with 1 being “not at all” and 5 being “a great deal.” Time and travel savings were also asked as open-ended questions. In some cases, providers observed the caregiver eliciting feedback from the care recipient (patient). Following the visit, multidisciplinary clinical providers also completed a 4-question survey examining the extent to which they agreed with statements about perceived similarity to in-person visits, perceived benefit from limiting exposure, and overall satisfaction. Responses were rated on a scale from 1 to 5, with 1 being “not at all” and 5 being “a great deal.” Both patient and provider surveys included an opportunity to provide free-response comments about the visit. Patient surveys included an open-ended question about recommendations for the service. When caregivers assisted with the completion of the surveys, they generally discussed responses with the patients.
Patient demographics, distance from clinic, active medications, active problems, cognitive status, and encounter diagnoses were collected from the medical record.
Data Analyses
We conducted descriptive analyses to characterize the sample and examine the feasibility of converting appointments to telemedicine. The percentage of visits converted was calculated. Patients’ acceptability of, and satisfaction with telemedicine appointment included analyses of the survey satisfaction questions and calculation of average time and mileage saved. Clinician acceptability was determined based on survey responses. Cronbach’s alpha was used to determine internal consistency of patient and provider surveys. The open-ended question on time saved was excluded since it was not a Likert scale item. Non-parametric analyses (Mann Whitney U) were used because data resulted in non-normal distributions. Data for both patient and provider scores was significantly different from a normal distribution based on the Shapiro Wilk Test of Normality (P < .001) for all variables. Qualitative content analysis 13 was conducted in that responses were grouped by respondent (patient/caregiver or provider) and type of visit (phone or video). One author initially coded the responses. Coded responses were subsequently reviewed by 3 authors including the lead author. The final categories were determined by consensus. Four authors reviewed the coded response and identified themes and subthemes. Qualitative data were compared and contrasted by modality code (phone or video) and respondent type (patient/caregiver or provider) as well.
Results
Demographics
Patients had a mean age of 85.5 years (SD = 6.8) and 72.1% had some degree of cognitive impairment (see Table 1). On average, these patients had 8.4 (SD = 4.4) active prescriptions for oral medications and 16.9 (SD = 4.9) active medical conditions. Patients’ average round trip distance from the clinic was 40.1 miles (SD = 34.3). Because patients receiving primary geriatrics care (n = 39) did not differ from those receiving consultative care (n = 3) on any characteristics, the findings for the 2 groups are reported together herein.
Characteristics of Patients with Completed Virtual Appointments (N = 43).
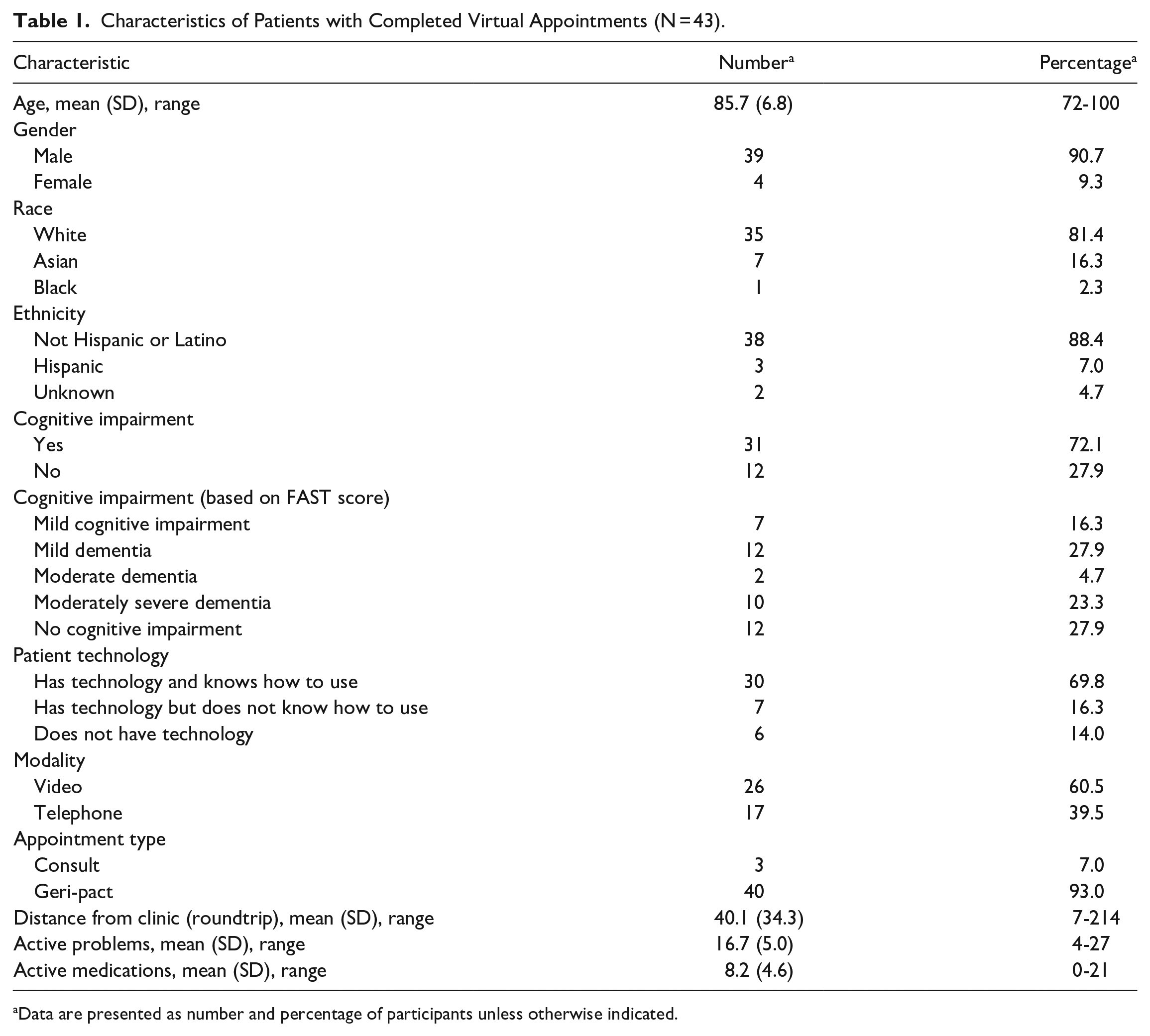
Data are presented as number and percentage of participants unless otherwise indicated.
Providers had a mean age of 41 years (range 31-63) and were in the disciplines of geriatric medicine, nursing, social work, and psychology. Approximately 12 providers completed a total of 80 evaluations. Due to anonymity of surveys, we do not have the exact number of unique provider survey respondents.
Converted Appointments
Of the 62 scheduled appointments, 43 telemedicine visits (69.4%) were conducted. Of the remaining 19 visits, 1 was conducted in-person, 1 rescheduled, 1 no-showed, 2 were deceased, and 14 canceled. Cancellation reasons included: non-urgent issues (n = 4), preference to wait for face-to-face (n = 4), admission to a skilled nursing facility and did not need urgent care (SNF) (n = 1), needed in-person treatment but could not leave SNF during pandemic (n = 1), issue addressed prior to appointment (n = 1), and unknown reasons (n = 3). Of the telemedicine visits, 26 were by video (60.5%) with the remainder by phone. Introducing VVC, coaching technology set-up, and testing prior to appointment required 1 to 4 phone calls per patient. All patients with dementia had support from a caregiver to complete their visits. Barriers to video visit included low technological literacy, lack of device with camera, inability to follow the email instructions with video visit link, internet and bandwidth difficulties, and password difficulties.
Surveys
Patients or caregivers completed 32 surveys yielding a response rate of 74.4%. Providers completed 80 surveys, corresponding to 35 visits (≥1 provider gave feedback each visit), thus yielding a response rate of 81.4%. Internal consistency was calculated with Cronbach’s alpha separately for 6-items in the patient survey (α = .75) and the 4-item provider survey (α = .78), and results showed good reliability for each scale. Survey findings revealed similar ratings across both patients and providers. The medians for both patient and provider responses on all questions were 5, which suggests that patients and providers had similar, positive perceptions about telemedicine compared to in-person visits, limiting exposure, and visit satisfaction. Across these 4 questions, patients scored on average between 4.50 and 4.97, and providers scored on average between 4.66 and 4.93. A Mann-Whitney U test was conducted to determine whether there was a difference between patient and provider scores on 4 similar items across the surveys. Parametric analyses were not used because the data was not normally distributed. Patients and provider responses did not significantly differ on the 3 items: similarity of visit to an in-person visit (U = 1107.5, P = .099), feeling better by limiting exposure to others (U = 1187, P = .408), and overall satisfaction (U = 1107, P = .235). Due to the distribution of the responses from patients and providers differing significantly, we were unable to use the Mann-Whitney U test to examine the extent to which the conversion to video/telephone appointments improved either access to care (patient) or ability to provide care (provider). Instead, we utilized a chi-square analysis to examine whether patients and providers different in their responses regarding access to care or ability to provide care (dichotomized as 1-4 vs 5). No differences in the distributions of responses emerged (χ2 = 1.75, P = .186).
On average, patients reported “a great deal” of travel cost savings (M = 4.4, SD = 0.9). Patients saved approximately 2 hours of travel time (M = 118.6 minutes, SD = 59.0). After the appointment, patients indicated greater comfort with using video or telephone visits in the future (M = 4.5, SD = 0.9) (see Table 2).
Frequency of Patient and Provider Evaluation Responses.

Missing items are denoted with superscripts: aN = 31, bN = 79. When items are missing, the total percentage does not equal 100%. Approximately 12 providers completed the evaluations.
Qualitative Analysis
Thirty-one visits (n = 13 telephone, n = 18 video) included comments for qualitative analysis. We identified 2 main themes expressed by both patients and providers: (1) technology set-up and usability and (2) satisfaction with visit (see Table 3). Telephone set-up and usability appeared to be easy and efficient for both patients and providers. In contrast, providers reported that video technology was cumbersome and time-consuming, but no patients or caregivers reported technology challenges with videos on the survey. The second theme, satisfaction with visit, revealed similarities across both modalities (see Table 3). Patients reported feeling connected and appreciative of the visits regardless of modality. Providers appreciated the ability to include family members in different locations and see the patient’s living environment, an observation not possible in an outpatient clinic.
Patient/Caregiver and Provider Perspectives on Technology and Satisfaction with Visit.
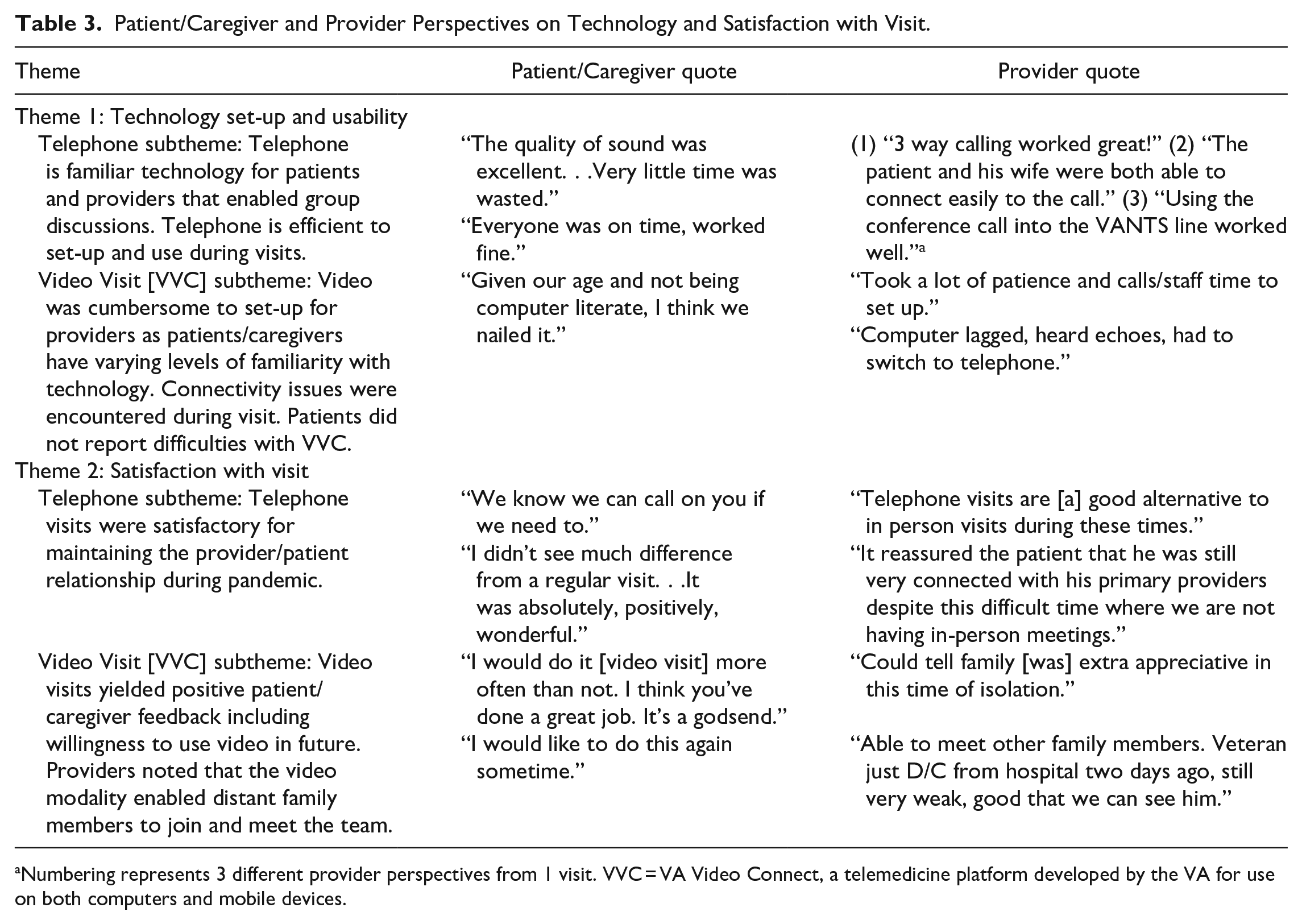
Numbering represents 3 different provider perspectives from 1 visit. VVC = VA Video Connect, a telemedicine platform developed by the VA for use on both computers and mobile devices.
An additional theme, clinical assessment and communication was noted by providers, but not patients. Telephone was effective for obtaining clinical history, but the lack of visual input for a physical exam proved challenging for specific situations (ie, assessment of leg swelling, wounds, or lung examination.) Video permitted examination of wounds, but an in-person evaluation would have been preferred given limited clarity of some video, which may have impacted accuracy of the virtual physical exam.
For patients with hearing impairment, providers reported challenges during telephone visits, but not video visits. Multiple providers noted effective communication on video with one mentioning “I think we got more accomplished on this video visit than in person.” while another provider highlighted the benefit of telemedicine for providers “This patient is COVID+. I am so grateful I didn’t have to evaluate in person.”
Discussion
This organizational case study showed that telemedicine care via phone or video is not only feasible for geriatric primary care services, but also accepted and appreciated in this very frail, older adult clinic. There was a large time investment in helping this population set up the technology and software for video visits, but this worthwhile investment resulted in high patient and provider satisfaction. Most telemedicine conversions were made to video visits, despite low level of technology access and literacy in the older population. 14 The COVID-19 pandemic provided the opportunity to deliver telemedicine to this vulnerable group and examine the experience of these visits using feedback from all involved participants: patients, caregivers, doctors, nurses, social workers, psychologists, and trainees.
Our findings clarified the role of phone versus video visits for tele-geriatrics care. Phone calls facilitated history taking, discussion of mood, chronic condition management, medication discussions, dementia management, caregiver support conversations, and discussion of goals of care. Video visits were necessary for dermatologic issues, wound care, leg edema, and other conditions where visual examination adds crucial information. Physical exams via video, while less clear than in-person assessments, were still adequate. Video visits helped visualize living situations and support socially isolated patients and caregivers. Topics covered via phone could also be covered during video visits, provided the internet connectivity and video quality remained adequate. When internet connectivity was poor, video visits were more challenging than telephone visits. For patients with hearing impairment, impulsivity issues, or difficulty staying on topic, virtual visits were challenging, but similar challenges are present with in-person visits. During virtual visits, providers tried to streamline communication by having 1 team member lead the discussion.
Our findings demonstrated numerous ways in which virtual visits were superior to in-person visits. These included team inclusiveness, inclusion of other family members, goals of care conversations, anxiety and depression management, and dementia caregiver counseling and support. The virtual format facilitated superior team communication to in-person visits. Providers noted that virtual visits enabled the entire care team to meet at the same time with the patient, allowed multiple providers with different expertise to answer patient questions, and even facilitated discussion of challenging topics such as advanced care planning. Furthermore, due to the telemedicine format, important family members who live far away from the patient were able to attend, allowing for improved family-care dynamics and promoting shared decision making. Dementia caregiver counseling was easier to conduct by telemedicine, because the patient could step away from the visit in the comfort of their own home, while the caregiver conversation continued.
Providers, patients, and caregivers expressed a high degree of satisfaction over the time efficiency, travel time saved, and cost savings of virtual visits. The average time savings of almost 2 hours is very significant for older patients, who often have mobility limitations and may depend on others to accompany them to in-person visits. Multiple patients expressed that although they value in-person visits, they would like the option of continuing some telemedicine appointments after the pandemic.
Several limitations should be noted regarding our case study. First, our case study sample size was small, which limits our power to detect significant effects such as differences in perceptions among patients/caregivers and providers and limits the generalizability of our findings. Second, because our sample contained a high proportion of patients with cognitive impairment, the findings may be more reflective of the caregivers’ perceptions rather than those of the patients themselves. Third, we did not collect information on the caregivers’ demographic characteristics, which limits the conclusions that can be drawn about factors influencing their responses. Fourth, it is possible that our patients and their caregivers had access to technology more readily than individuals in other regions, which may contribute to high satisfaction with the modalities. Despite these limitations, this case study that was designed to examine the feasibility and acceptability of telemedicine visits provides evidence of patient, caregiver, and provider acceptance of telemedicine among a sample of complex older patients receiving care from a VHA medical center.
Conclusion
Telemedicine during a pandemic comes with challenges, including the time needed to prepare and assist patients with technology, securing the availability of devices, and ensuring sufficient bandwidth to support surge usage. Despite these challenges, satisfaction amongst older patients, caregivers and providers with virtual visits was generally high. Providers completed the majority of clinical care virtually, and patients expressed interest in continuing with telemedicine after the pandemic. Having an organizational champion to lead telemedicine conversion efforts was also important to the success of this endeavor. The use of telemedicine in geriatrics has been sustained in the primary care clinics and has now expanded to consultation clinics as well based on the lessons learned from our case study. Future directions include developing telemedicine rotations for geriatric medicine fellows and evaluating whether conversion to telemedicine for primary care improves access to care and delays hospitalization or long-term care institutionalization. Future studies may also consider examining whether provider characteristics and beliefs predict telehealth use, satisfaction, and other outcomes among geriatric populations.
Footnotes
Acknowledgements
Views expressed in this article are those of the authors and not necessarily those of the Department of Veterans Affairs or the Federal Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.