
Abstract
Historically, many rural veterans have had to travel long distances to obtain care from Veterans Health Administration (VA) facilities. 1 For several years, the VA has been establishing community-based outpatient clinics (CBOCs) to bring primary care, mental health care, and other office-based services closer to veterans who live far from the nearest VA medical center.2,3 Currently, more than 900 CBOCs are in operation nationwide, which has greatly reduced the travel burden for many rural outpatients. Nevertheless, in some of the most rural areas of the nation, veterans still must travel quite far even to reach the nearest CBOC, and the number of veterans living nearby is too low to justify creating another local full-time CBOC. Recently, the VA’s Office of Rural Health (ORH) funded the creation of smaller outreach clinics (ORCs) to serve market areas of more than 250 but fewer than 1300 veteran enrollees (and where enrollee populations are not projected to increase within 5 years). Though ORCs operate on a part-time schedule (30 or fewer hours per week), they are expected to adhere to VA quality standards providing primary care, on-site case management, access to mental health care, and referral capacity. 4 To date, use and quality of care in ORCs have not been studied.
One of the first outreach clinics established by ORH is in sparsely populated (11 persons/mi2) Aroostook county of northern Maine, a region that has long been recognized as lacking access to VA primary care services. 5 The ORC is situated in Houlton, Maine, a town of 6500 residents located at the northern terminus of interstate 95, approximately 3 miles from the Canadian border and 195 miles north of Maine’s only VA hospital, the Togus VA Medical Center in Augusta. Before the Houlton Outreach Clinic (HORC) opened, the nearest VA primary care available to veterans in the Houlton area was either in Lincoln, ME (81 miles to the south) or Caribou, ME (55 miles to the north via secondary roads).
Co-located with the private Houlton Regional Hospital, HORC opened in June 2008 with capacity to serve about 225 veterans, 1 full day per week with VA staff including a physician, registered nurse, and medical clerk detailed from the Bangor, Maine CBOC 120 miles to the south. The HORC provides primary care services including evaluation, diagnosis, and treatment of medical conditions not requiring subspecialty or inpatient services, and referral to other VA locations for veterans who need mental health or other specialty care. Laboratory and radiology services for HORC patients are provided on-site through a contract with the regional hospital. Patients at HORC who require services on days when the clinic is closed will be seen by VA primary care in Lincoln, Bangor, or Togus.
To better understand the outreach clinic model as a strategy for improving rural veterans’ access to VA healthcare, we took advantage of a natural comparison to examine patients’ use of HORC and the quality of care received there, as well as their use of local non-VA primary care. We compared use and standard VA quality performance measures for HORC care to those of the 2 nearest VA primary care sites: the small-staffed but full-time VA clinic in Lincoln and the full-service CBOC in Caribou.
Method
Measures for the comparisons were abstracted from VA electronic medical records, Computerized Patient Record System (CPRS), for any outpatient visits received by HORC patients, any Lincoln patients, and a random sample of Caribou patients with at least 1 primary care provider visit between June 4, 2008 and June 10, 2009. We defined a provider visit as an in-person contact with a medical doctor, nurse practitioner, or physician assistant. Nurse-only visits or telephone contacts were not included in the analysis. We developed a paper chart abstraction tool that included data definitions and coding rules. Patient-level data elements included sociodemographic information (sex, date of birth, race/ethnicity, insurance status, new enrollee vs transfer status), health care use (number of VA medical visits made during the study period, whether the patient had a local non-VA medical doctor at the beginning of the interval, whether the patient maintained that local doctor throughout the interval). We compared the HORC, Lincoln, and Caribou clinics on the percentages of cases meeting VA quality of care performance standards set by the VA’s Office of Quality and Performance for several measures: screenings for obesity, alcohol misuse, depression, tobacco use, breast cancer, cervical cancer, colorectal cancer; influenza and pneumococcal vaccination; and adequate management of diabetes, hypertension, and cardiovascular disease. 7 Patient zip codes were abstracted using GoogleMaps (http://maps.google.com/maps?hl=en&tab=wl) to obtain time estimates for travel to the sites of care. This study was approved by Dartmouth College’s Committee for the Protection of Human Subjects and the Edith Nourse Rogers Memorial VA Hospital Institutional Review Board.
Three research assistants experienced in medical chart review performed the abstractions. Training by the authors included a review of the content and organization of CPRS, definitions of the specific data elements to be abstracted, and sample chart abstractions. Each research assistant then abstracted the same sample set of 10 charts; interrater reliability, assessed using Fleiss’ κ, was good (κ = 0.84). The research assistants abstracted study records independently, and each case was abstracted by only 1 assistant. Paper data were entered into a Microsoft Access 2007 database and corrected for entry errors. Data analyses compared the 3 treatment sites on performance measures and primary care use during the study period using chi-square analyses (or Fisher exact test for some low-n comparisons). All data analyses were conducted using SAS 9.2 (SAS Institute Inc., Cary, NC).
Results
The abstractors reviewed 1251 charts (164 HORC, 602 Lincoln, and 485 Caribou patients). Mean age was 65 years, range 21-93; very few patients were other than male, white, and non-Hispanic (Table 1). Approximately 75% of all patients had health insurance coverage, and Caribou patients were a little more likely to have it than HORC or Lincoln patients (χ2 = 8.0, P < .05). Regardless of treatment site, nearly 3 in 5 patients had a non-VA local medical doctor (LMD) involved in the patient’s care, and among patients who had one, nearly all kept their LMD involved in their care throughout the study period. About one-third of patients at the HORC and Lincoln clinic had 3 or more provider visits at these clinics during the study year, whereas fewer than 1 in 7 patients at the Caribou CBOC did (χ2 = 66.7, P < .001. When the analysis was limited to patients who relied solely on the VA for care (ie, those without a local medical doctor), roughly 4 of 5 HORC or Lincoln patients had 3 or more visits, as compared to 3 of 5 Caribou patients (χ2 = 26.6, P < .001).
Demographic and Utilization Characteristics

Abbreviation: HORC, Houlton Outreach Clinic.
Of the 164 HORC patients, only 6 (3.7%) were new enrollees to VA care. All others had transferred care from another VA hospital or clinic, and the majority (74.0%) had transferred from Caribou. Averaging across all patients who transferred their primary care to HORC, their 1-way driving burden was reduced by 52.9 miles and 58.1 minutes.
From the cases that were eligible for each quality of care performance measure (e.g., breast cancer screening, diabetes management, pneumococcal vaccination), we calculated the percentage of cases that met VA standards (Table 2). Performance at HORC was significantly worse than the other clinics on obesity screening (χ2 =84.3, P <.001); referral of smokers to cessation clinic (χ2 =17.9, P = .001); diabetes management (including completion of annual hemoglobin A1c testing [χ2 = 5.7, P =.06], low-density lipoprotein cholesterol control [χ2 = 6.6, P = .04], blood pressure control [χ2 = 8.2, P = .02], nephropathy screening [χ2 = 9.4, P = .009], and retinal examination [χ2 = 20.7, P < .001]; and blood pressure control for patients with a diagnosis of hypertension (χ2 = 36.7, P < .001).
Adherence to VA Performance Measures
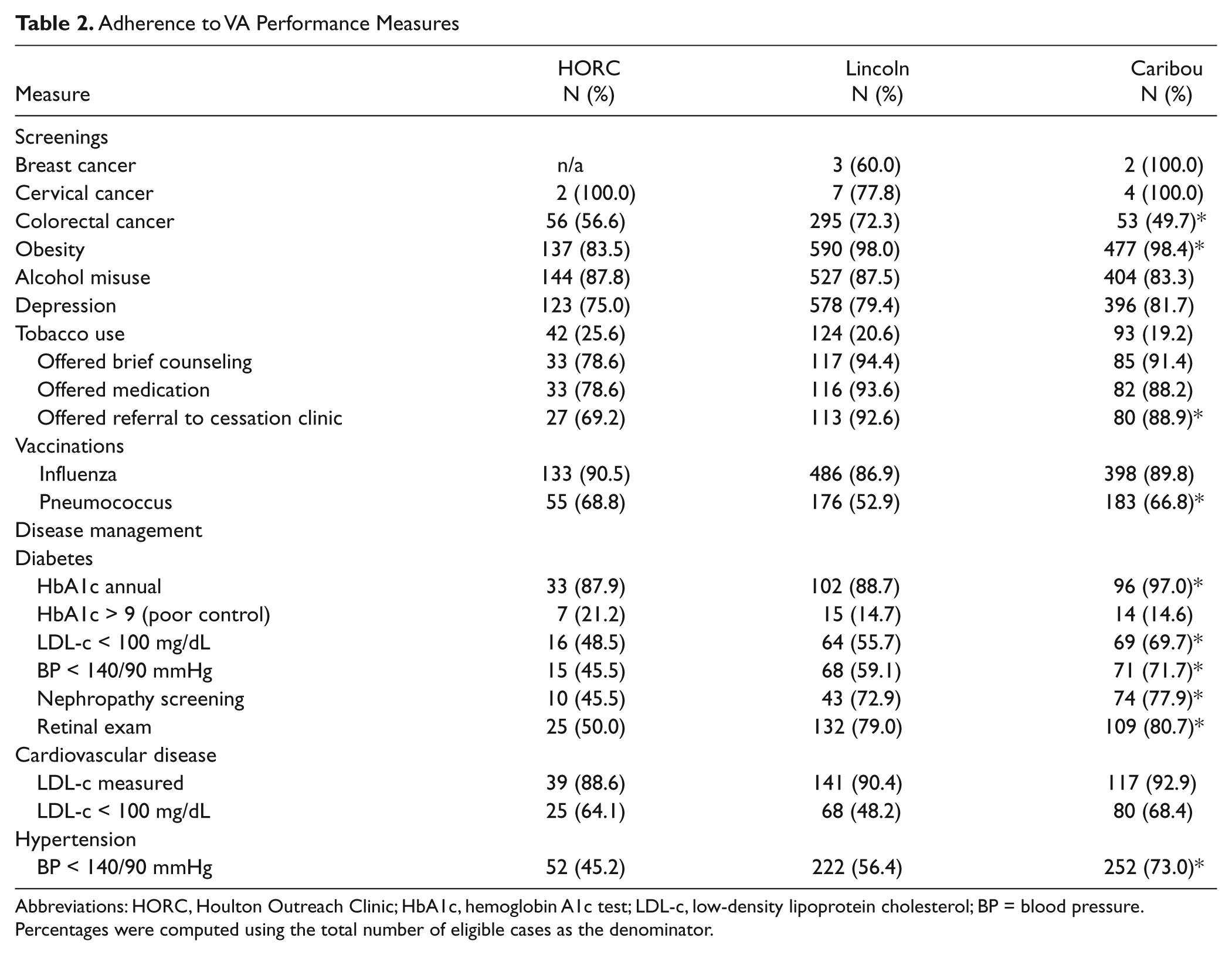
Abbreviations: HORC, Houlton Outreach Clinic; HbA1c, hemoglobin A1c test; LDL-c, low-density lipoprotein cholesterol; BP = blood pressure.
Percentages were computed using the total number of eligible cases as the denominator.
Discussion
We compared use and quality at a new 1-day per week outreach clinic in rural northern Maine (Houlton) to that provided at the nearest VA clinic (Lincoln) and the nearest CBOC (Caribou), both of which operated 5 days per week. Patients formerly seen at these sites who opted to use the HORC had their travel burden reduced by nearly an hour, on average, and they were more likely than Caribou patients to have multiple medical visits during the study year. Although this finding might demonstrate improved access, it is also possible that because the full-time and full-service CBOC offers more options for follow-up, such as attending nursing clinics for hypertension or diabetes management, its patients needed fewer visits with a medical doctor, nurse practitioner, or physician’s assistant (our definition of a “visit”).
Care at HORC was comparable to other VA sites on many quality of care measures, but the clinic did not perform as well with regard to obesity screening, referral for smoking cessation services, and diabetes or hypertension management. Obesity screening (demonstrated in the medical record by a valid body mass index) probably was influenced by a simple lack of equipment, as we learned that HORC does not have a stadiometer attached to its scale, so that patients must go to a separate area in the hospital to obtain a height measurement. The comparison sites also offer on-site smoking cessation clinics, but HORC does not have this capacity. To receive this service, HORC patients must travel to the Bangor CBOC (120 miles) or the Togus VAMC (195 miles), and so HORC providers might have chosen not to offer this option based on the anticipated travel burden. Diabetes and hypertension management might have been less adequate at HORC because, as with smoking cessation, both comparison sites have chronic disease management clinics run by staff nurses, whereas HORC does not.
Other Limitations
Our understanding of the roles of local medical doctors in the care of these patients is limited. Three-quarters of patients had health insurance, and the majority had a local non-VA medical doctor who remained involved in their care throughout the study period; differences across sites were small and not (or marginally) significant. We do not know how much care or what specific services were provided by LMDs or their level of responsibility for developing treatment plans, guiding care, and serving as “primary” provider from the patient’s perspective. The HORC attracted only 6 new enrollees during its first year, of whom 4 had health insurance and all had a local medical doctor that they kept. We do not know whether the HORC filled some unmet need for these new enrollees, if it served simply as an adjunct to their current care, if it became a source for inexpensive medications, or if it was being given a “trial run” as a replacement.
The quality of information obtained through medical chart abstraction can suffer from both abstraction and data entry errors. Several quality of care measures, however, are derived from standardized templates in the VA electronic medical record for gathering specific information during medical visits, which likely reduce errors and between-clinician variation. Services ordered and received through LMDs, such as laboratory tests, screenings, and exams, might not be documented in the VA chart, so that our quality of care measures may have been underestimated. It also is possible that patients who transferred care to HORC differed from others in their health status prior to the study, their compliance with treatment, or other characteristics that might affect use or performance measures. Additionally, performance during the first year of operation does not necessarily predict that of subsequent years, since use and quality may well improve after a “start-up” period.
Conclusions
Establishing a 1-day-per-week ORC in remote northern Maine greatly improved the convenience of primary care for several current VA outpatients, but it attracted few new enrollees. Several quality of care metrics were lower than those of other VA outpatient sites, possibly because of equipment and staffing limitations. Most patients also had a local non-VA medical doctor with whom they remained in care despite the availability of VA services.
Footnotes
Acknowledgements
This material is the result of work supported with resources and the use of facilities at the VA Maine Health Care System, Augusta, ME and the White River Junction VA Medical Center, White River Junction, VT. The authors wish to thank Suzan Spears, Adrienne Kinne, and Kristin Collins for their abstraction of study charts. Their contribution to this project was invaluable. The contents of this article do not represent the views of the Department of Veterans Affairs or the United States government.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.