
Abstract
Introduction:
Telehealth has the potential to improve access and timeliness of care, enabling primary care teams to deliver hybrid (virtual/in-person) services that will likely extend beyond the COVID-19 pandemic. To optimize its use and sustainability, it is imperative to understand how primary care teams perceive the suitability of telehealth services, including appropriate choice of mode (telephone or video). However, there is limited research on providers’ decision-making processes surrounding telehealth use in primary care, including whether to use telephone or video, which this VA-focused study addresses. We examined how primary care (PC) team members determine whether to use telehealth and the mode of delivery, in the care of patients.
Methods:
Qualitative case study that included 15 semi-structured interviews with employees who provided or supported telehealth care at primary care clinics at the Veterans Health Administration. We used a team-based rapid analysis approach to identify experiences using telehealth soon after COVID-19’s emergence, consisting of the creation of structured summaries of each transcribed interview. The lead author then identified and compiled themes and sub-themes related to the suitability of telehealth in primary care, as well as associated quotes from transcripts. Resulting themes and quotes were reviewed and validated by 2 members of the project team.
Results:
Primary care team members considered several factors when assessing both the suitability of telehealth for appointments, and mode of use. They were largely guided by patient-related factors including patient preferences, specific health issues, and access to technology. Additional considerations centered on team members’ personal preferences and factors that supported the wellbeing of the team, such as the flexibility to work from home (work-life balance) and protection from infection. Generally, participants viewed the option of both telephone and video telehealth modalities as useful tools in the care of patients although a few respondents emphasized its inferiority to in-person care.
Conclusions:
Determining the suitability of telehealth services, including appropriate choice of mode is complex. Its suitability is tied to a variety of factors related to multilevel resources, preferences, and timing. When appropriate, telehealth should be considered a useful tool in the care of patients and for employee well-being.
Introduction
With the onset of the COVID-19 pandemic in March 2020 and the resulting rapid expansion and adoption of telehealth services in outpatient services in primary care, there have been a multitude of Veterans Health Administration (VA) and non-VA studies that have examined patient and provider satisfaction,1-4 advantages and benefits, as well as disadvantages, challenges, and barriers to both the implementation and use of telehealth services in primary care.5-12 Some of the benefits/advantages to the provision and implementation of telehealth services for patients are increased availability of services, improved follow-up care, improved communications, 5 reduced deferred care and facilitated health outreach, additional opportunities for education,7,8 reduced travel burden on patients,6,7 timelier access to care, 10 and increased ability to provide patient-centered care.7,8 Some of the benefits for providers are increased flexibility due to in teleworking, 5 enhanced communication with patients and caregivers, improved efficiency for providers,7,8 more time for patient counseling, opportunities for medication reconciliations, and ability to evaluate patient home environment. 9 Although most studies have found high levels of satisfaction from both patients and providers, patients tend to be more satisfied compared to providers.1-4
Recent research on telehealth has also identified a range of challenges/disadvantages to the provision and implementation of telehealth services for both patients and providers. For patients, some of the challenges and disadvantages are difficulties with access to and use of technologies, concerns about change in patient engagement and expectations, 5 unequal access to virtual care for rural, older, or cognitively impaired patients,7,8 patients’ skills and comfort, 12 privacy and confidentiality, as well as language and cultural differences. 11 For providers, some of the challenges and disadvantages are inability to conduct a physical examination, limited personal connection and touch, changes in workflow to avoid provider burnout, 9 payment parity for in-person versus video and telephone visits,7,8 difficulties in diagnosing in the absence of a physical exam, technological limitations, maintaining the therapeutic relationship with patients, 5 and provider knowledge and skills. 12 Given that telehealth will likely be incorporated into hybrid care beyond the COVID-19 pandemic,13,14 it is imperative to have a more nuanced understanding about the suitability of delivering primary care services via telehealth, as well as a deeper dive into the mode (telephone or video) of delivery. There is limited research on both patient and provider preferences about what types of outpatient care are best suited for virtual visits15-17 as well as their mode (telephone or video) of delivery. Previous research comparing the 2 modes of telehealth encounters in primary care, telephonic care versus videoconferencing, has found that the 2 modes are similar in consultation length, content, and quality, 18 while videoconferencing may have an advantage over telephone, since the clinician can visibly see patients and provide useful clinical context.18-24 Videoconferencing, compared to telephonic care, may also help in building patient-provider rapport, improving patient-provider communication.18-21 On the other hand, technical problems, and disparities in access to camera-enabled digital devices and use are more common with videoconferencing than with telephone encounters.18,19,25 Ultimately, previous research has shown that both telehealth modalities (video and telephone) play important roles in health care access. 26 However, there is still a knowledge gap related to providers’ decision-making processes surrounding telehealth use in primary care, including whether to use telephone or video, which this VA-focused study addresses. The VA is the ideal setting to examine these issues given that it has over 2 decades of experience in virtual care. Although some sites encountered technological challenges early in the pandemic due to issues such as patient internet connectivity, these sites benefited from having access to VA’s resources and expertise in telehealth, which enabled a rapid shift to virtual care when providers were instructed to switch to telehealth, and specifically video when possible.27-30 Moreover, interviews for this study were conducted at an opportune time, soon after telehealth processes and practices became routine in local clinics, which enabled respondents to easily recall and reflect on various care delivery modes. VA primary care is based on a patient-centered medical home model that includes an interdisciplinary care team (eg, physicians, nurses, social workers, dietitians, pharmacists, mental health providers). In this qualitative study, the main objective is to describe the factors that primary care providers consider when determining appropriate encounter modality (telehealth or in-person) and telehealth mode (telephone vs video).
Methods
Study Design and Setting: Data were collected as part of a study comparing the use and uptake of telehealth services in a VA health care system across 3 clinics (PC, cardiology, and home-based primary care). 31 Results presented here are drawn from the portions of the study examining telehealth implementation and modes of telehealth delivered in primary care.
Study population: Semi-structured telephone interviews were conducted with employees who provided or supported telehealth care at PC clinics in one healthcare system. Primary care leadership at the VA local site helped advertise the study through email, and a project team member individually reached out to staff members to explain the study and inquire about participation. Project team members obtained informed, verbal consent from participants to participate in interviews.
Data collection and management: Fifteen interviews were conducted from July to October 2020 with 7 primary care providers (PCPs), 5 nurses, 2 social workers, and 1 psychologist. Each 30-min interview was conducted by 2 to 3 research team members. The interview guide, developed in coordination with clinical co-investigators, centered on 6 topics: (1) pre-COVID-19 telehealth experience, (2) telehealth implementation during COVID-19, (3) telehealth processes, (4) modes of telehealth delivered, (5) facilitators and barriers using telehealth during COVID-19, and (6) patient assistance with telehealth. Interviews were recorded and transcribed.
Analysis: We used rapid qualitative analysis methods to guide our review of the data.32,33 First, we used interview guide domains to create a structured summary template that was used by our team to summarize interview data from each interview. The summary template was reviewed and modified by the research team after testing it with a single transcript. The team next divided interview transcripts and independently summarized assigned interviews that were later reviewed by another team member to achieve consistency in data summary. Next, the analytic team created a “summary of summaries” matrix that consolidated findings across interviews and captured key points and themes. The lead author then identified and compiled themes and sub-themes related to telehealth use in primary care, as well as associated quotes from transcripts. Resulting themes and quotes were reviewed and validated by 2 members of the project team. This study was approved by the local VA Greater Los Angeles Institutional Review Board.
Results
Overview of Findings
Participants considered several factors when assessing the suitability of telehealth for primary care appointments: patient preferences and characteristics, patient health conditions, and participants’ own professional and personal preferences (Table 1).
Key Findings: Primary Care Team Members’ Perceptions of Telehealth Suitability and Mode of Use.
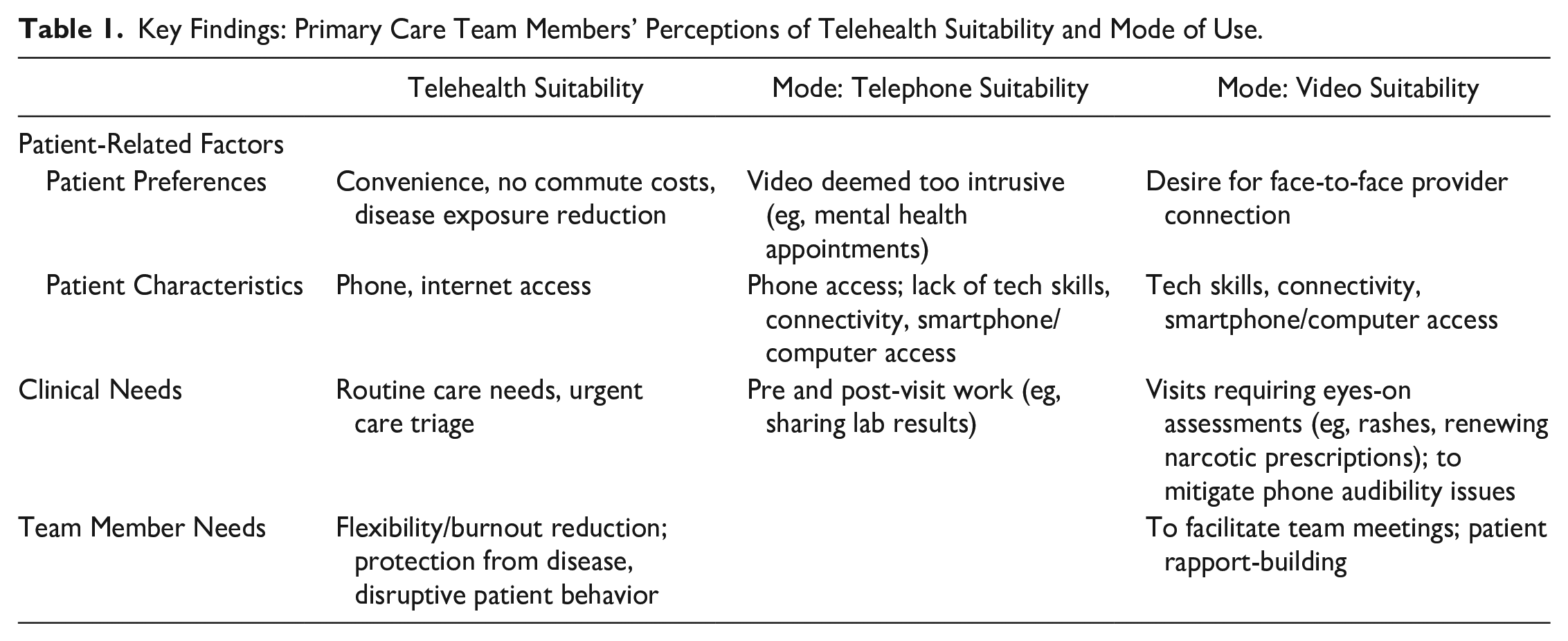
Patient Preferences and Characteristics
Primary care team members discussed 2 different decision-making paradigms when discussing the use of telehealth for care delivery. The first was whether telehealth as a modality was appropriate. The second was which mode of telehealth to employ.
Primary care team members emphasized the importance of patient preference and characteristics when determining the appropriateness of telehealth. Team members explained that some patients preferred virtual encounters because they were considered less burdensome and expensive in terms of travel time and gas costs. In addition, patients requested telehealth appointments to reduce their exposure to communicable diseases such as COVID-19 or when they were not feeling well enough for an in-person visit. Conversely, telehealth was not deemed suitable for patients with certain characteristics, such as those without phone or internet access. For example, one team member explained: “. . .a lot of them (patients experiencing homelessness) don’t have phones, and they just randomly show up. So, sometimes you have to take them when they show up so you can get them care.” (Registered Nurse)
To determine telehealth mode (eg, telephone vs video visits), patient characteristics and preferences emerged again as important considerations. Respondents explained that video was inappropriate for those lacking smartphone/computer access and skills or internet connectivity, and for patients who prefer telephone virtual care, such as patients receiving mental health treatment who may find video encounters too intrusive. “So, the older, [people in their] 80s, not all of them [have a] computer. Some of them only have like a flip phone, they can’t receive things. And I think that’s hard.” (Registered Nurse) “Some patients find mental healthcare overwhelming generally, and so there’s something about doing on the phone feels safer. Like they can talk without having to like look me in the eye and not feel uncomfortable to them. I’ve noticed some patients that I was seeing before the pandemic, and then we switched to telephone, and I think some people opened up a bit more, I felt like, because we were doing it on the telephone. Of course [for] other people that’s not the case.” (Psychologist)
However, in other cases, patients requested video because it helped them feel more personally connected to providers. “. . .the patients, especially older ones that we thought maybe wouldn’t like it (video) as much because of the technology, they actually really like it. They said they feel more cared for. We’ve gotten some really good feedback. They like actually looking at you and feel more engaged.” (Registered Nurse)
Patient Health Conditions
Respondents considered telehealth useful for addressing certain routine care needs, as well as triaging urgent care patients, thereby reducing the number of walk-ins during the pandemic. Determining which telehealth mode to use was based in part on patients’ specific clinical needs.
Telephone visits were used for pre- and post-visit work such as patient reminders for immunizations and medical screenings, geriatric social work screenings, and sharing lab results.
For patient health conditions that require seeing patients, video was considered indispensable, especially when clinics were limiting in-person care during the pandemic. Video was useful for observing blood pressure readings, patients with multiple symptoms, rashes, and renewing narcotic prescriptions: “. . .one time a patient complained about a rash, and I asked them to show me the rash. And it turns out he had sunburn, which I could see quite clearly on the video, and I told him as such. So that was very helpful. That saved me from saying, ‘I don’t know what it is, come in’.” (PCP) “. . .in order for us to give narcotics, you have to see the patient every so often.” (Registered Nurse)
In addition, a clinical pharmacist stated that video was useful for providing visual cues in instances when patient audibility was difficult over the phone.
Behavioral health providers explicitly discussed the value of video appointments, due to the video allowing them unique exposure to their patients’ home environments. As one social worker explained: “I had a Veteran who. . .had mental health issues. He was believing that chemicals were coming through his vents, and [through video] he was able to walk me around the apartment and show me the vents he was talking about and show me the smudges on the wall that he was worried about. I wouldn’t have been able to get that quality of, you know, an interaction over the phone.” (Social Worker)
Telehealth, whether by phone or video, was considered inadequate for some patient health conditions requiring hands-on exams such as mammograms, pap smears, procedures such as removing sutures, screenings for colon cancer, some skin issues, and for patients with chest pain. In addition, some types of appointments were considered too cumbersome to do virtually, such as mental health screenings, where patients complete an extensive intake form that was difficult to share on-line, or too medically complicated, like caring for patients with multiple comorbidities: “So, some of those patients that are that complex, [clinicians] have to see them. You just can’t do a phone unless it’s just a focused visit. If they have 16 things that you’ve got to address, sometimes you just have to bring them in.” (Registered Nurse)
Primary Care Team Members’ Needs
Respondents perceived telehealth as helpful for meeting some of their own professional needs. For example, due to the nature of the interdisciplinary primary care team whose members were not always in-clinic on all days due to COVID-19, video conferencing technology was found to be essential to facilitate team huddles. In addition, video was deemed useful as a rapport-building tool for new patients. “I think [video is] nice, because then you actually see the person and you meet them for the first time, at least you can put a face to the name, which is nice. It’s harder to do that if you do it by phone.” (PCP)
Several respondents also discussed how telehealth was personally advantageous by enabling them to work remotely (and thereby eliminating commute times), which provided more job flexibility and improved employee quality of life. One respondent explained: “. . .in some capacity, [teleworking] is actually really good for, you know, like preventing some level of burnout. . .I’ve realized as it’s gone on it’s also helped us in terms of just balancing the stress . . ..” (Social worker)
A few also described how telehealth eliminated direct contact with patients which provided a measure of safety from infection and in one case, disruptive patient behavior in the form of sexual harassment: “. . .personally I feel safer with telehealth. So, there’s certain encounters with patients where, you know, they’re making inappropriate remarks, or they’re just sort of agitated, and that’s just not a problem when we’re doing telehealth. I think also frankly just like not being around the VA as much I’m not getting like the sexual harassment stuff just from random people in the hallways because I’m not there.” (Clinical Pharmacist)
Perceptions of the benefits of telehealth were not shared among all respondents. A number of team members described face-to-face care as clinically more useful. This was due in part to technological challenges of video conferencing in the early days of telehealth implementation, but also due to the particular nature of a primary care visit. As described by one PCP, “I think that the information that we get often and what we can do with our interaction is somewhat limited and not as complete as the face-to-face visits.” (PCP)
Discussion
Primary care team members described several factors that contributed to the suitability of telehealth for appointments, as well as the mode of use (eg, video vs telephone). They were largely guided by patient-related factors, including patient preferences, specific health issues, and patient characteristics, such as access to technology. Additional considerations centered on team members’ personal preferences and factors that supported the wellbeing of the team. Generally, participants viewed the option of both telephone and video telehealth modes as useful tools in the care of patients although a few respondents emphasized its inferiority to in-person care.
Patient preference can facilitate or hinder telehealth usage.13,34 In line with prior research, providers in our study reported that patients value telehealth because it reduces exposure to communicable diseases such as COVID-19, and because it eliminates commute time and gas expenses.7,35,36 Adepoju et al 37 underscored this consideration by demonstrating that the likelihood of having a telehealth appointment increased with longer commute times. Importantly, however, they did not find a consistent pattern of telemedicine use within patients, suggesting its use only for occasional care delivery (ie, for renewing prescriptions).
Our findings indicate that providers also take patient-related factors into account when considering the most appropriate mode of telehealth for an appointment. As also discussed in the wider literature, providers in this study emphasized the lack of suitability of video visits for patients who have access issues stemming from socioeconomic and technology factors (ie, patients who do not own smartphones) and/or lack of connectivity (ie, patients living in rural areas where internet may be slow).5-8,11,38 Thus, it’s important to take access equity issues into account when assessing the feasibility of video as an effective option for telehealth and healthcare delivery. 7 And yet, for patients with suitable resources to conduct a video visit, video may afford unique opportunities that a telephone encounter cannot, such as providing a visual connection between patient and provider and for new patients, to build rapport. Part of building rapport is establishing trust, and Hall et al 39 found, for example, that video was particularly useful in telepsychiatry for patients who had difficulty establishing trust with new providers. Further, as described by our providers, video is also useful for health issues that require eyes-on care such as blood pressure readings, rashes, and mental health care where seeing a patient’s environment provides useful contextual information for providers. For example, mental health providers have reported high satisfaction with video visits due to the ability to visualize patients’ home lives 40 and primary care providers have reported that video facilitates the engagement of family caregivers in patient care. 36 Despite the advantages of video telehealth visits, respondents in our study echoed findings reported elsewhere that, notwithstanding the mode, telehealth is not ideal for issues that require a hands-on physical exam which could theoretically lead to missed diagnoses.13,41,42
In addition to advantages conferred to patients, telehealth may also enhance the ability to provide clinical care. For example, healthcare professionals in our study and elsewhere have reported that telehealth facilitates team and patient communication. 7 It can also reduce exposure to infection 43 and according to our findings, may limit providers’ exposure to disruptive patient behavior, which is a prevalent problem throughout the health care industry.44,45 For instance, one study reported that 60% of women physicians had endured sexual harassment by patients in the past year. 46 Similar studies of VA are limited, but a survey among internal medicine physicians at one VA medical center found that 97% of women and 77% of men had ever experienced patient-perpetrated sexual harassment. 47 Given the adverse effects of harassment on staff productivity, retention, and mental health48,49 it is critical that healthcare organizations take steps to protect employee well-being, which includes further investigation of how telehealth may impact occurrences of disruptive patient behavior, including sexual harassment of staff. For example, contrary to our findings, there is limited evidence that telephone and video visits may not necessarily protect healthcare staff from patient-perpetrated harassment.50,51
Primary care team members reported to us that telehealth had facilitated job flexibility and protected against burn out. Indeed, other researchers report high satisfaction with telehealth and its association with lower symptoms of burn out among primary care residents and providers, which may be tied to reduced patient visit lengths. For example, a survey of primary care residents revealed that burnout scores decreased with the use of telemedicine, which was also associated with patient visit lengths that were 10 to 20 min shorter than face-to-face care. 52 However, other evidence points to providers’ increased anxiety and reduced job satisfaction with telehealth use due to the difficulty of managing conditions and expressing empathy remotely, changed or increased workflows, and technological challenges.9,53-55 Ultimately, emerging evidence points to the importance of effective telehealth education, adequate video and audio quality and technology, and improved workflow integration to increase uptake and satisfaction with telehealth among healthcare professionals.1,56-58
Study Limitations and Future Directions
This study has several limitations. First, it captures data from VA primary care clinics located in a single geographic region with urban and suburban areas and thus may not be representative of primary care team members’ experiences in other regions, particularly rural ones. However, a strength is that the sample was drawn from a high telehealth utilizing system which increased research feasibility and yielded rich data. Second, it does not explore the perspectives of patients and other stakeholders but instead delves into the underexplored topic of primary care team perspectives related to telehealth care delivery, although we were unable to detect clear differences by disciplinary role due to our sample size. Moreover, providers’ discussions of access challenges indicate the need for additional inquiry into the continued challenge of technology access. To gain a more complete picture of the suitability of telehealth services in primary care, future research should also focus on the perspectives of patients, who our research shows are a driving force in the uptake of this technology in medical practices. In addition, future research would benefit from exploring how perspectives of primary care team members may vary by role, including how telehealth may or may not mitigate disruptive patient behavior during clinical encounters. Finally, future research should examine factors related to organizational capacity to provide telehealth services through a focus on leadership support, IT support, and other available resources.
Conclusions
The findings of this study suggest that determining the suitability of telehealth services, including appropriate choice of mode (telephone or video) is complex. Its suitability is tied to a variety of factors related to multilevel resources, preferences, and timing such as patient preference, digital access issues, specific health conditions, and team members’ needs. For example, although telehealth has the potential to offer patients and healthcare professionals flexible care arrangements, disparities in high-speed internet access and disruptions in workflow could mitigate its advantages. More research is needed across healthcare settings to identify successful care patterns, as well as research into care quality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based on a COVID-19 Rapid Response project (C19–20-204) funded by the US Department of Veterans Affairs (VA), Health Services Research & Development (HSR&D). The funding body did not play any role in the study design, data collection, data analysis, interpretation of data, and writing the manuscript.