
Abstract
Introduction:
Same-day referrals from primary care to mental health increase subsequent mental health treatment engagement. VA Primary Care-Mental Health Integration (PC-MHI) clinics offer integrated mental health services embedded in primary care clinics, providing a key entry point to mental health care. Although telehealth use expanded rapidly after the onset of COVID-19, the impact of telehealth on same-day primary care access among new PC-MHI mental health patients is unknown. To address this knowledge gap, we examined associations between telehealth use and same-day primary care access in VA PC-MHI.
Methods:
We examined electronic health record data to identify same-day primary care appointments among PC-MHI patients who initiated care during 3/1/2018 to 10/29/2021. We used logistic regression analyses to evaluate the effect of telehealth on same-day primary care access. Time, demographic characteristics, mental health diagnoses (PTSD and depression), and substance use disorder diagnosis were evaluated as covariates.
Results:
New PC-MHI patients who were seen via telehealth were less likely to receive same-day primary care access than patients seen in person (OR: 0.54; 95% CI: 0.41-0.71; P < .001).
Conclusions:
Despite the potential advantages of using telehealth to increase access, VA patients with an initial PC-MHI visit via telehealth were less likely than patients seen in person to be referred from primary care. Telehealth may adversely affect primary care referrals to mental health services, an outcome that could ultimately reduce specialty mental health care continuity. There is an urgent need to identify strategies to facilitate PC-MHI care coordination in the telehealth context.
Keywords
Introduction
Integrated behavioral health clinics with mental health services embedded within primary care settings facilitate smooth and timely transitions between primary care and mental health providers. 1 Despite the coronavirus disease-19 (COVID-19) pandemic and an attendant widespread shift to telehealth for mental health care, little is known about how virtual care impacts the ability of integrated behavioral health clinics to quickly engage patients presenting with new mental health symptoms. This is a critical knowledge gap given that time to treatment initiation is a key factor when engaging mental health patients. 2
In the Veterans Health Administration (VA), Primary Care-Mental Health Integration (PC-MHI) clinics provide co-located mental health care embedded in primary care settings. 3 PC-MHI focuses on the treatment of mental health concerns that frequently present in primary care, including depression, anxiety, alcohol abuse, and PTSD. 4 Many PC-MHI patients are new to mental health care, or are re-establishing care after an extended period without mental health care. PC-MHI services include engaging patients in mental health care, supporting mental health care management, and receiving “warm handoffs” from primary care.3,4
Prompt initiation of mental health care following a primary care appointment can increase the likelihood that patients receive and attend subsequent specialty mental health appointments.1,5,6 Ideally, a primary care patient with mental health needs is referred to PC-MHI (i.e., receives a warm handoff) and seen by a PC-MHI mental health provider on the same day as their primary care appointment. 3 A study by Cornwell et al 7 reported that 33% of new PC-MHI patients received a same-day referral from primary care. Yet, despite the centrality of the warm handoff to the PC-MHI model, few studies have examined the extent to which integrated care settings are able to provide same-day service. 5
The VA has provided telehealth services since 2003. 8 Prior to the onset of COVID-19, VA had the largest telehealth program in the U.S., with approximately 2.6 million visits provided in 2019. 9 Following the onset of the U.S. COVID-19 pandemic and associated VA telehealth expansion, 10 integrated care providers sought alternatives to traditional, in-person strategies for managing care coordination. Virtual care strategies to facilitate care coordination in the integrated care context include electronic consults, video consultations, and messaging via the electronic health record. 11 To our knowledge, no research exists about the impacts of telehealth on same-day referrals from primary care to PC-MHI mental health care. This information would facilitate the identification of strategies to maximize same-day care in the wake of widespread telehealth adoption.
Using VA integrated behavioral health as a case study, we aimed to examine the impact of telehealth on warm handoffs between primary care and PC-MHI mental health providers. Data were collected from an urban PC-MHI clinic. This work provides an exploratory examination of VA PC-MHI capabilities to manage care coordination while providing virtual care.
Methods
We investigated PC-MHI same-day primary care access in a sample of veterans seeking care in a California VA PC-MHI clinic. The clinic served approximately 1200 veterans during fiscal year 2021 and is located in a large, urban VA medical center. The study employed a retrospective cohort observational design. We used electronic health record (EHR) data to identify patients who visited the clinic between 3/1/18 and 10/29/21. Data from eligible patients’ initial PC-MHI visit during the study period were examined to determine whether PC-MHI mental health care was initiated after a same-day primary care appointment. As PC-MHI is designed to be an initial access point to mental health, we only included PC-MHI naïve visitors with no PC-MHI visits during the previous 2 years. This study was approved by the VA Greater Los Angeles Healthcare System Institutional Review Board. No participants were recruited for this study, which consisted solely of EHR secondary data analyses. Therefore, a Waiver of HIPAA Authorization and Waiver of Informed Consent covered all study activities.
Measures
PC-MHI telehealth use
The PC-MHI telehealth variable indicated whether each patient attended their initial PC-MHI visit via telehealth or in person. PC-MHI visits that took place over telephone or video were categorized as telehealth visits, and were identified using VA clinic codes. We created a patient-level PC-MHI telehealth visit indicator variable (0 = No, 1 = Yes).
Same-day primary care access
The same-day primary care access measure assessed whether PC-MHI patients saw a primary care provider on the same day as their initial PC-MHI visit. PC-MHI and primary care visits were identified using VA clinic codes. The measure represents the availability of PC-MHI providers to receive patients who are referred from primary care. This measure mirrored a national VA Office of Mental Health and Suicide Prevention mental health quality metric. The denominator consisted of PC-MHI naïve patients who initiated care during 3/1/18 to 10/29/21. The numerator consisted of patients with a visit in primary care on the same day as their initial PC-MHI visit.
Time
Because the onset of COVID-19 affected VA telehealth utilization patterns, we included visit time as a covariate (0 = pre-COVID-19, 1 = during COVID-19). We began data collection in March 2018 to allow examination of same-day primary care access prior to the onset of the U.S. COVID-19 pandemic (March 2020).
Demographics
We obtained gender, race/ethnicity, and age as of the initial PC-MHI visit date from patient characteristics tables in the EHR. All patients who reported Hispanic ethnicity were categorized as Hispanic.
Mental health/substance use disorder diagnosis history
PTSD, depression, and substance use disorders are the most commonly treated diagnoses in PC-MHI. 3 To control for mental health diagnosis history, we obtained PTSD, depression, and substance use disorder diagnoses from the EHR. PTSD (0 = No, 1 = Yes), depression (0 = No, 1 = Yes), or substance use disorders (0 = No, 1 = Yes) were determined based on the presence of 1 inpatient diagnosis or 2 outpatient diagnoses during the 2 years preceding each patient’s initial PC-MHI visit.
Analyses
We calculated frequencies for demographic characteristics, past-year mental health diagnoses, substance use disorder diagnoses, and PC-MHI telehealth use. We ran a logistic regression analysis to evaluate the effect of PC-MHI telehealth use on same-day primary care access. The regression model included same-day primary care access (0 = No, 1 = Yes) as the dependent variable. PC-MHI telehealth use (0 = No, 1 = Yes) was the independent variable. Time period (pre vs during COVID-19), demographic characteristics (age, gender, race/ethnicity), mental health diagnoses (PTSD and depression), and substance use disorder diagnoses were evaluated as model covariates. All analyses were performed using Stata (v.15). 12
Results
Table 1 shows patient same-day primary care access rates, demographic characteristics, mental health diagnoses, and substance use disorder diagnoses by PC-MHI telehealth use. The sample included 2479 veterans. The mean age was 48.7 years old (SD = 16.4). Seventy-two percent of the sample were men. The sample was 33.4% Non-Hispanic White, 42.8% Non-Hispanic Black, 16.4% Hispanic, and 7.5% Other Race. Diagnosis rates for PTSD and depression were 28.0% and 28.2%, respectively. Sixteen percent of the sample had a substance use disorder diagnosis.
Patient Characteristics by PC-MHI Telehealth Use.

Abbreviation: PC-MHI, Primary Care-Mental Health Integration.
The sample included patients from a California PC-MHI clinic with visits between 3/1/2018 and 10/29/2021. The sample comprised PC-MHI-naïve patients, defined as having no PC-MHI visits during the previous 2 years. Pre-COVID-19 pandemic denotes visits that took place before 3/1/2020. PTSD, depression, and substance use disorder diagnoses were derived from VA visits within 2 years prior to PC-MHI visit date.
P < .05.
Thirty-six percent of patients who visited PC-MHI in person received same-day primary care, compared to 19.7% of telehealth visitors (χ2(1) = 65.5, P < .01; Table 1). Thirteen percent of veterans initiated PC-MHI services via telehealth pre-COVID-19 onset, compared to 80.5% during COVID-19 (χ2(1) = 1061.0, P < .01). This rapid telehealth expansion during COVID-19 corresponds with findings from past research with VA populations. 10 Regarding patient characteristics, women comprised 39% of in-person PC-MHI visitors, but only 3% of telehealth visitors. Whites (32% vs 36%) and Hispanic (16 vs 18%) veterans comprised a higher proportion of PC-MHI telehealth patients compared to in-person patients, whereas Black veterans (44% vs 39%) were less represented among telehealth patients compared to in-person patients (χ2(1) = 8.4, P = .04).
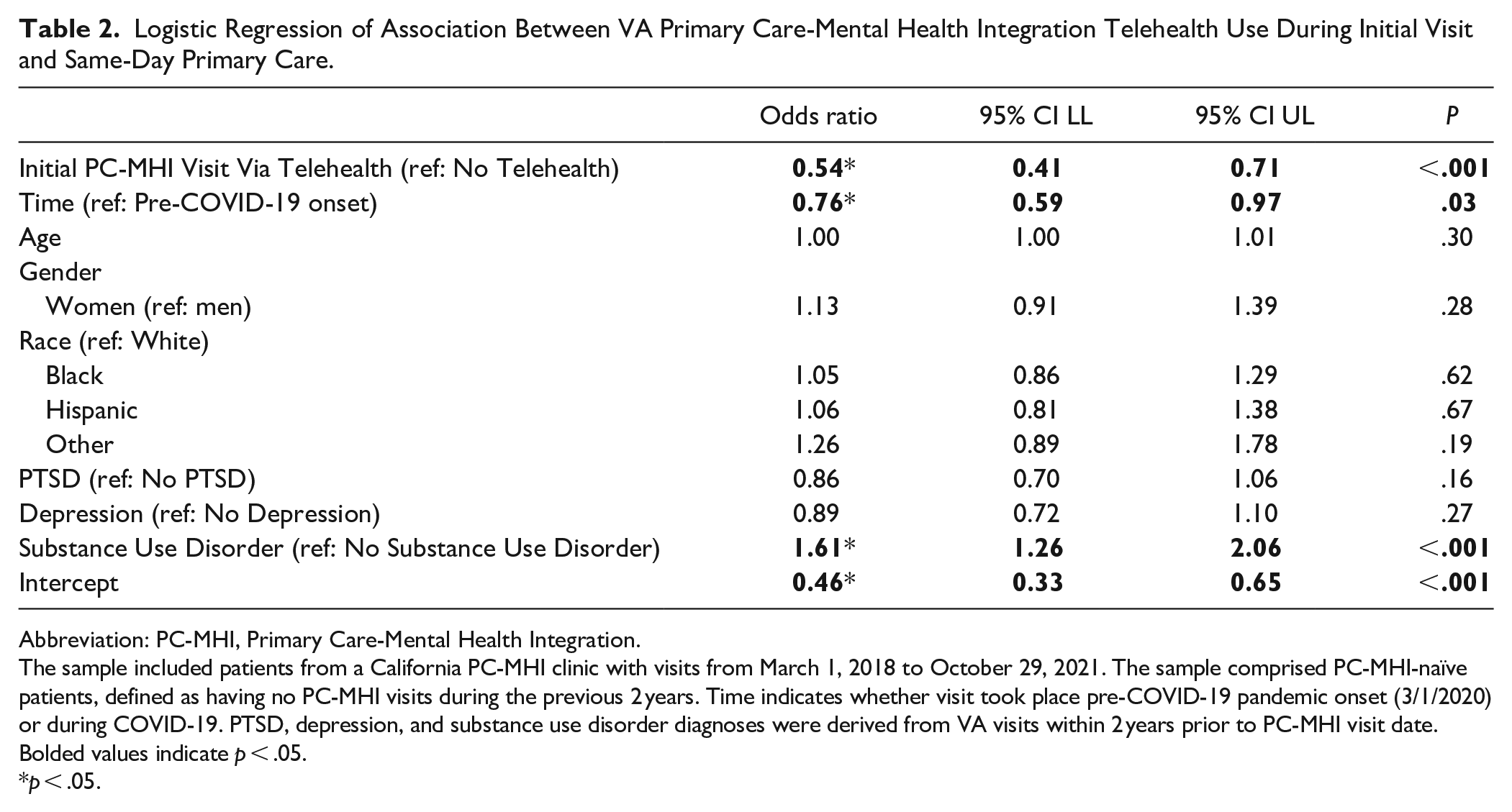
Table 2 shows logistic regressions predicting same-day primary care access among new PC-MHI patients. Same-day primary care visits declined from pre-COVID-19 to during COVID-19 (OR: 0.76; 95% CI: 0.59, 0.97; P = .03). Veterans with substance use disorders were more likely to receive same-day primary care access than veterans without substance use disorders (OR: 1.61; 95% CI: 1.26, 2.06; P < .001). No other demographic or clinical characteristics were associated with same-day primary care access.
Logistic Regression of Association Between VA Primary Care-Mental Health Integration Telehealth Use During Initial Visit and Same-Day Primary Care.
Abbreviation: PC-MHI, Primary Care-Mental Health Integration.
The sample included patients from a California PC-MHI clinic with visits from March 1, 2018 to October 29, 2021. The sample comprised PC-MHI-naïve patients, defined as having no PC-MHI visits during the previous 2 years. Time indicates whether visit took place pre-COVID-19 pandemic onset (3/1/2020) or during COVID-19. PTSD, depression, and substance use disorder diagnoses were derived from VA visits within 2 years prior to PC-MHI visit date. Bolded values indicate p < .05.
p < .05.
Veterans who attended their initial PC-MHI mental health visit via telehealth were significantly less likely to receive same-day primary care access than veterans seen in person (OR: 0.54; 95% CI: 0.41, 0.71; P < .001). See Figure 1 for a graphical depiction of the association between PC-MHI telehealth visits and same-day primary care access.

Initial PC-MHI visit same-day primary care: PC-MHI Telehealth versus PC-MHI In Person.
Discussion
Although PC-MHI telehealth access increased during the COVID-19 pandemic, veterans who attended an initial PC-MHI mental health visit via telehealth were less likely to receive same-day primary care compared to veterans who initiated care in person. There are several possible explanations for this finding. With increased telework capability for mental health providers nationally and social distancing for in-person providers, there may have been fewer opportunities for spontaneous interactions between providers, which can facilitate handoffs in integrated settings. 13 In addition, although several electronic modalities exist to help providers coordinate care, 11 it is unknown whether they are as effective as face-to-face interactions.
Given the important role of integrated behavioral health in enhancing mental health care continuity1,14 and widespread use of telehealth, there is an urgent need to develop strategies to facilitate warm handoffs and greater real-time communication between primary care and mental health providers over telehealth. For example, past research has shown that training providers on the tenets of PC-MHI increases the use of mental health assessment tools among primary care providers. 15 Similarly, trainings focused on electronic strategies for warm handoffs and effective real-time communication between providers could increase same-day referrals in the telehealth context.
PC-MHI telehealth visits increased substantially after the onset of COVID-19. This finding demonstrates the rapid pivot to telehealth that occurred throughout the VA system, particularly for mental health care. 16 Because the present study aimed to examine the impacts of telehealth on same-day primary care in PC-MHI, we did not assess predictors of telehealth uptake. However, descriptive statistics showed that men, White veterans, and Hispanic veterans were more represented among telehealth patients than in-person patients, while women and Black veterans were less represented among telehealth patients than in-person patients. Prior research in a national VA population reported that lower income, higher disability, and higher number of chronic conditions are positively associated with receipt of VA video telehealth, while residence in a rural area, older age, and homelessness are negatively associated with video telehealth. 17 In the current study, the urban location of the clinic, and the sample’s relatively younger average age compared to the general VA population, may have contributed to high overall telehealth uptake (80% of PC-MHI visitors) during COVID-19. More work is needed to understand how barriers and facilitators of telehealth use affect same-day primary care in PC-MHI.
The PC-MHI model is designed to serve as an entry point into mental health services, with the intent to increase patient access to VA mental health care.3,4 However, patients who attended their initial PC-MHI visit via telehealth during COVID-19 appeared to be less likely to experience same-day primary care access than patients whose initial PC-MHI visit occurred in person. To explain these findings, other questions beyond the scope of this project would benefit from further investigation. For instance, it would be helpful to develop a greater understanding of strategies that integrated behavioral health and primary care providers used to collaborate in real-time via telehealth, and to understand which electronic communication modalities were most effective. Identifying potential discrepancies between primary care referrals to PC-MHI and patient follow-through would disentangle the contributions of patient versus provider behavior to same-day primary care access.
Strengths and Limitations
This is the first known work to examine the influence of telehealth on same-day primary care access in an integrated behavioral health setting. We used a PC-MHI-naïve sample, which allowed us to replicate the circumstance of patients who initiated mental health care for the first time. However, although focusing on a single PC-MHI clinic allowed us to capture VA telehealth use in an urban context, our findings may not generalize to other VA clinics with different patient populations.
Conclusions
VA PC-MHI clinics are rapidly increasing telehealth services as a strategy for maximizing access to care. However, in the current study telehealth reduced same-day primary care access, a critical component of integrated behavioral health models. Because effective PC-MHI care coordination enhances mental health care continuity, the development of strategies for maximizing same-day care via telehealth is an urgent priority.
Footnotes
Acknowledgements
The views expressed in this article are those of the authors and do not necessarily represent the position or policy of the U.S. Department of Veterans Affairs or the United States government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.