
Abstract
Introduction
As per the World Health Organization (WHO) definition, “medicines are rationally used if patients receive medications appropriate to their clinical needs, in doses that meet their own individual requirements, for an adequate period of time, and at the lowest cost to them and their community.” 1 However, contrary to the definition, about 67% of the world population lacks access to essential medicines, and more than half of all medicines are not appropriately prescribed and dispensed, and 50% of patients use the dispensed medicines inappropriately. 2
Lack of essential medicines and improper dosage regimen may result in serious health problems, especially among pediatric patients and individuals with chronic diseases like cardiovascular disorders, diabetes mellitus, and epilepsy.3,4 On the other hand, availability of essential medicines increases the health care professionals’ satisfaction and also motivates to use their training and expertise fully, thereby directly improving quality of patient care. 5 Medication errors resulting from inappropriate use of medicines add unnecessary costs to patients, caregivers, and health care facilities. 6 A previous study revealed that each preventable adverse drug reaction costs additional US$8750. The growing antimicrobial resistance, particularly in low-income countries, also attributed to the overuse and misuse of medicines. 7 On top of that, the drug use problems may initiate patients to self-treat and reduce hospital visit due to medicine inaccessibility and loss of confidence in the health services. 8
WHO recommends regularly evaluating drug use in the health facilities from the perspectives of professionals, patients, and health facilities themselves. The use of medicines needs to be monitored in terms of (a) the types of the problem—it helps develop targeted strategies toward specific problems; (b) the magnitude of the problem—hence, the effect of the strategies can be monitored based on the degree of the problems; and (c) the reasons for irrational use—helps choose relevant, feasible, and effective strategies. 4
The most common reasons for misuse of medicines are lack of knowledge, absence of objective information, health workers job burden, negligence, inadequate staff training, inaccurate diagnoses, and poor patient-practitioner relationship. 9 As a result, communities experience different types of drug use problems like polypharmacy, improper duration of treatments, a high or low dose of medicines, and self-medication widely.1,10,11
There are well-established techniques for measuring the irrational use of medicines at health facilities. The use of World Health Organization/International Network for the Rational Use of Drugs (WHO/INRUD) core indicators is among the strategies to identify and quantify the drug use problems at the health facility level. Generally, there are 3 WHO/INRUD core drug use indicators, including prescribing, patient care, and facility indicators. Prescribing indicators address clinicians prescribing practice while patient care indicators helps assess mainly pharmacists dispensing practice and patient awareness of prescribed medicines. The last, facility indicators like availability of treatment guidelines helps to evaluate drug use practice from facility perspectives. 12 However, related studies conducted in Ethiopia employed the prescribing and facility indicators frequently while patient care indicators overlooked. Therefore, in addition to patient exit interviews, we used the following patient care indicators to evaluate the pharmacists dispensing practice and patient knowledge of dispensed medicines 12 : (a) average consultation times (ACT)—helps measure the length of time the pharmacists spend with their patients during consultations; (b) average dispensing times (ADT)—used to measure the length of time the dispensers spend in dispensing drugs to patients; (c) percentage of drugs actually dispensed (PDAD)—helps measure the degree to which the health facilities can offer the prescribed medicines; (d) percentage of drugs adequately labeled—helps measure the degree to which dispensers attach all the necessary information on the drug packages they dispense; and (e) patients’ knowledge of correct dosage (PKCD)—helps measure the effectiveness of the information provided to patients on the dosage regimen of the drugs they received. Despite the size of services that Jimma Medical Center offers, there is a poor culture of monitoring and evaluating medicine use patterns in the hospital. Therefore, the purpose of the current study was to investigate patient knowledge of dosage regimen and the pharmacists dispensing practice.
Methods and Materials
Study Area
The study was conducted at Jimma Medical Center. It is one of the oldest teaching hospitals in Ethiopia and was established in 1937 by Italians for the purpose of serving their troops. The hospital is located in Jimma city 346 km southwest of Addis Ababa, the capital city of the country. Currently, it provides service for the catchment population of 15 million with 1600 staff members, 32 intensive care units, and 800 beds. The hospital has 4 outpatient pharmacy or outpatient department pharmacies (OPD pharmacies) and 5 inpatient pharmacies.
Study Design and Period
A cross-sectional study design was employed from March 1, 2018 to April 29, 2018.
Source and Study Populations
The source populations for this study were all dispensary units and also patients attending Jimma University Medical Center. The study populations were all outpatient pharmacies (the 4 OPD pharmacies) and the patients visiting those pharmacies. However, based on their experience, some of the dispensers were also interviewed to identify reasons for drug use problems.
Sample Size Determination and Sampling Procedures
All OPD pharmacies were included without any precondition. Regarding the participants’ sample size calculation, the study used a single population proportion formula and finite population correction (FPC) factor as follows:

where n = sample size from the formula;
However, before deciding the final sample size, the authors reviewed the most recent records at the outpatient pharmacies of the hospital to determine the approximate number of encounters per month. Accordingly, within the past month (just before the data collection) around 3000 patients have visited the pharmacies. Therefore, the sample size (n = 384) obtained from the general formula was adjusted by a finite population correction factor as the sampling frame (3000) was <10 000.

where n′ = the adjusted required sample size (384), and N = the population size (3000). Finally, by considering 5% nonresponse rates, the final sample size became 357.
Patients who visited the outpatient pharmacies during the data collection period and volunteer to participate in the study were randomly selected using a lottery method.
Data Collection Procedures
Data were collected prospectively using observational technique and patient exit interviews. Observational technique was used to collect data for calculating average dispensing times, percentage of drugs actually dispensed, average consultation times, and also determine some of the reasons for inappropriate use of drugs. Graduating pharmacy students who had a practical attachment at the outpatient pharmacy during the data collection period were employed as data collectors to minimize bias that might result from a change in dispensers’ behavior. Patient exit interviews conducted to collect data on patient knowledge of dispensed drugs, sociodemographic characteristics, the percentage of drugs adequately labeled, and other patient-related factors. Checklists and structured questionnaires were used for the observational data collection and patient exit interviews, respectively.
Measurements of Patient Care Indicators
The indicators used in this study were calculated as follows8,12:
Average consultation time (ACT):
WHO optimal value: ≥10 minutes
Average dispensing time (ADT):
WHO optimal value: ≥90 seconds
Percentage of drugs actually dispensed (PDAD):
WHO optimal value: 100%
Percentage of drugs adequately labeled (PDAL):
WHO optimal value: 100%
Patients’ knowledge of correct dosage (PKCD):
WHO optimal value: 100%
Data processing and Analysis
Statistical Package for the Social Sciences (SPSS) version 20 was used for analysis. After cleaning, coding, and entering into SPSS, a descriptive statistical analysis was conducted, and the outputs presented as frequency, percentages, mean, and standard deviation. Logistic regression analysis was also run to determine the association between patient knowledge of dosage regimen, and sociodemographic characteristics and other patient-related factors. Accordingly, bivariate analysis was conducted and variables with P value less than .25 were further analyzed in multivariate regression analysis. A critical point, P < .05 at a confidence interval of 95% in the multivariate analysis was used to determine the level of significance.
Data Quality Assurance
A pretest conducted on 5% of the sample size at Shenen Gibe hospital located in Jimma city to ensure the clarity and completeness of the data collection tools as well as to estimate the length of time each interview would take. The principal investigators provided training for the data collectors on how to collect the relevant data by describing the objectives and significance of the study. The investigators also daily checked the questionnaires for completeness of data.
Operational Definitions
Patient knowledge of dosage regimen: If patients adequately report the dosage schedule for all drugs. 12
Dosage regimen: includes frequency of administration, the dose per a single administration, the time interval between administrations, duration of treatments, and how a medicine is to be taken.
Drugs: interchangeably used with medicines.
Adequately labeled: As per the world health organization definition, a drug is adequately labeled if it includes at least patient name, name of the drug and when the drug should be taken. 11
Results
Sociodemographic Characteristics of the Participants
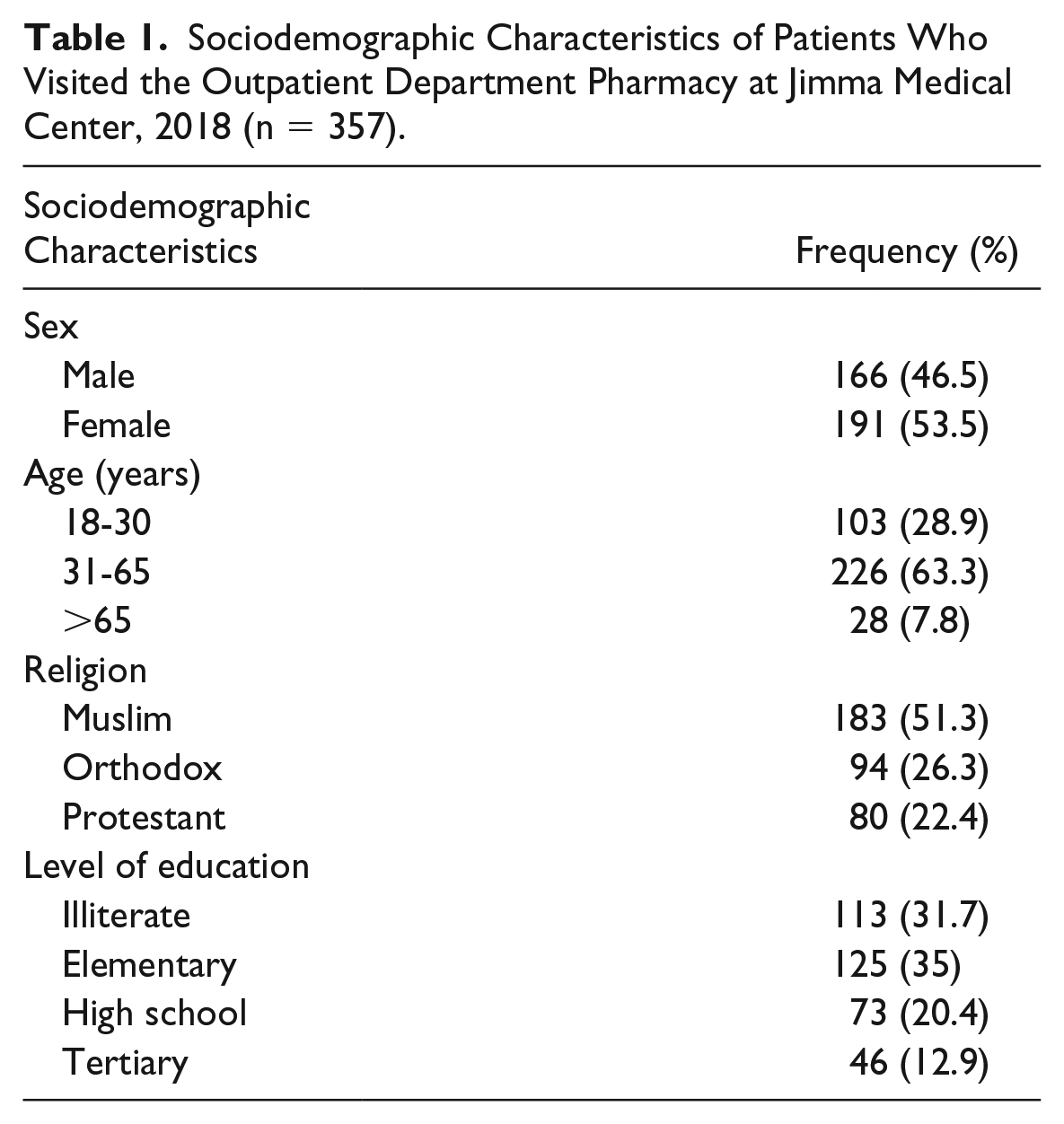
A total of 357 patients took part in the study, making a response rate of 100%. Of the total participants, more than half, 191 (53.5%) were females. Majority of them, 226 (63.3) were within the age range of 31 to 65 years. A total of 183 (51.3%) were Muslims, and the remaining were Orthodox, 94 (26.3%) and Protestant, 80 (22.4%) followers. Regarding educational background, majority the participants completed elementary school, 125 (35%) and 113 (31.7%) were illiterate (Table 1).
Sociodemographic Characteristics of Patients Who Visited the Outpatient Department Pharmacy at Jimma Medical Center, 2018 (n = 357).
The Proportion of Drugs Actually Dispensed and Adequately Labeled
A total of 928 different drugs were prescribed during the data collection period. Of the total prescribed drugs, 689 (74.25%) were actually dispensed and only 239 (34.7%) drugs were adequately labeled (Figure 1).

Graph showing the number of drugs prescribed, actually dispensed and adequately labeled during the study period at the outpatient department pharmacy of Jimma Medical Center, 2018 (n = 357).
The Length of Drug Dispensing and Patient Consultation Times
The average time spent to dispense drugs was 41.45 ± 12.1 seconds with a minimum of 19 and maximum 80 seconds. The length of consultation times on average was 49.13 ± 12 with a minimum of 20 and a maximum of 80 seconds.
The Types of Information Provided to Patients During Counseling
Majority of the patients received information about frequency of administration, 265 (74.2%), course of treatment, 148 (41.5%), amount to be taken each time, 138 (38.7%), and information about drug food interactions, 118 (33.1%). However, only 69 (19.3%) patients were asked to repeat the instructions about their medications to ensure their understanding (Table 2).
Types of Information Provided to Patients During Counseling at Outpatient Department Pharmacy of Jimma Medical Center, 2018 (n = 357).

Patient Knowledge of Dosage Regimen
During the exit interview, 267 (74.8%) patients correctly reported the dosage regimen of all dispensed drugs, that is, frequency of administration, the time interval between administrations; amount to be taken each time, duration of treatments, and how to take all the dispensed medicines (Figure 2).
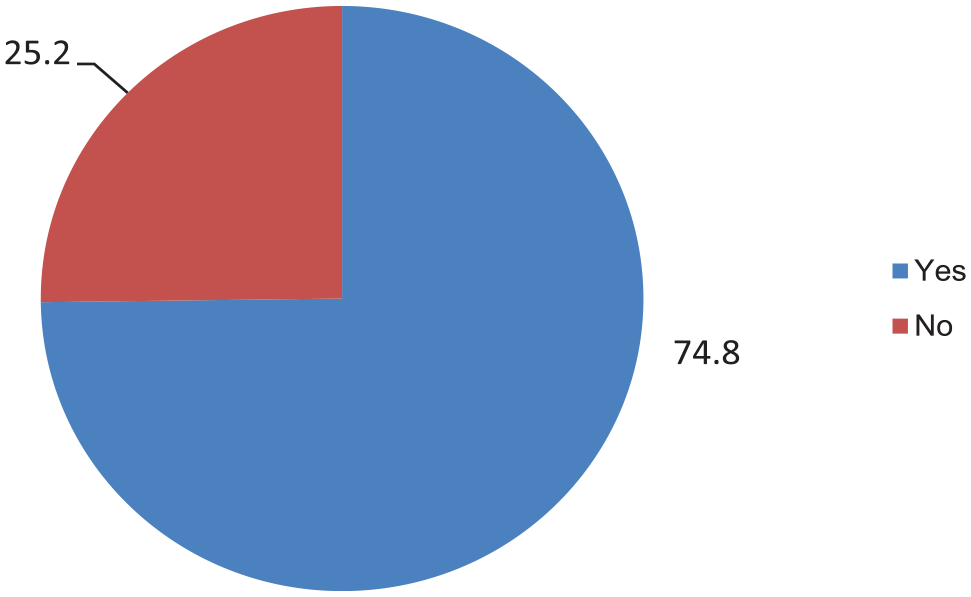
The distribution of patient knowledge of dosage regimen at the outpatient department of Jimma Medical CenterJMC, 2018 (n = 357).
Reasons for Poor Dispensing and Prescribing Practice
From physical observation and interview of some of the dispensers, the major reasons for drug use problems were patient load, absence of monitoring and evaluation, lack of incentives for staffs, language barriers, and the patients’ health condition.
Factors Associated With the Patient Knowledge of Dosage Regimen
Bivariate and multivariate logistics regression analysis conducted to determine factors associated with patient knowledge of dosage regimen. Accordingly, patient age, level of education, language barrier, severity of health condition, and number of drugs received by the patients became candidates for multivariate logistics regression analysis. After running the analysis, variables including language barrier (adjusted odds ratio [AOR] = 32.6, 95% confidence interval [CI] = 12.23-87.15), severity of health condition (AOR = 7.3, 95% CI = 2.70-19.56), and the number of drugs dispensed (AOR = 0.41, 95% CI = 0.18-0.87 [1 drug], AOR = 0.16, 95% CI = 0.61-0.42 [2 drugs]) were identified to have significant association with patient knowledge of dosage regimen (Table 3).
Bivariate and Multivariate Logistics Regression Analysis for Factors Associated With Patient Knowledge of Dosage Regimen at the Outpatient Department Pharmacy of Jimma Medical Center, 2018 (n = 357).
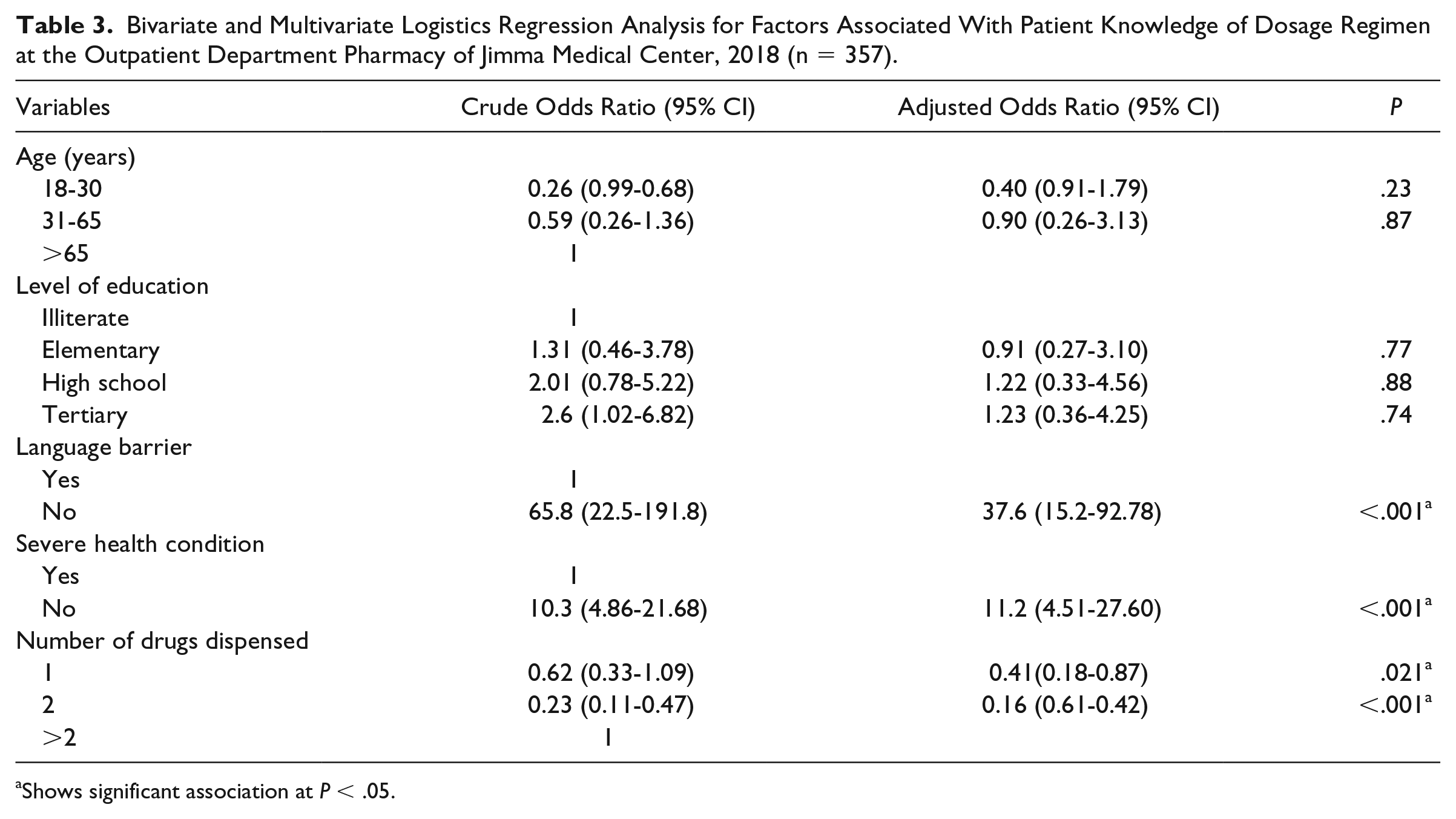
Shows significant association at P < .05.
Discussion
The current study revealed that 74.25% of the prescribed medicines were actually dispensed to patients during the study period. It is almost comparable to the study conducted in public hospitals of Eastern Ethiopia (75.77%) but lower than WHO recommendation (100%).1,13 This is an implication of poor medicine supply in Ethiopia.
Regarding medication labeling, it assists patients to identify the contents of the package and also find clear and concise information on how to use the prescribed medications. 11 In the present study, only 34.7% drugs were adequately labeled wherein at least the patient name, name of the drug, and when to take the medication were recorded. This finding is much lower than previous studies conducted in tertiary hospitals in Punjab, Pakistan and health facilities in Eastern Ethiopia where 100% and 64% of the dispensed drugs were adequately labeled, respectively.8,13 this vast discrepancy suggests a poor dispensing practice in Jimma Medical Center. The possible reasons as mentioned by the dispensers could be lack of commitment from top level management like failure to conduct monitoring and evaluation of pharmacy service regularly.
The current study also evaluated the length of time dispensers spent with their patients during consultation and dispensing medicines. Accordingly, the average dispensing and consultation times were 41.45 ± 12.1 and 49.13 ± 12 seconds, respectively. Compared with previous studies conducted in Niger and India14,15 and also WHO optimal values (dispensing times ≥90 seconds, consultation times ≥10 minutes),1,8,12 the dispensers in the present study did not give adequate time for their patients. The difference might be because of patient load at the dispensary point and staff commitment. However, the length of time health professionals spend with their patients has paramount impact on their treatment outcomes. Patients will have room to ask questions about their health and medications they are taking.
Concerning patient knowledge of dosage regimen, 74.8% of the current study participants had an awareness of correct dosage schedule for all dispensed medicines. The finding is still lower than WHO optimal value (100% expected),1,8 and a related study conducted at the referral hospital of South India wherein 89.3% knew the correct dosage regimen. 16 It infers poor dispensing practice and weak patient-practitioner relationship at Jimma Medical Center. As stated by the dispensers, the possible reasons might be lack of staff motivation and commitments secondary to absence of incentives and a system for monitoring and evaluation. In addition, language barrier, severity of patient health condition, and the number of dispensed drugs had significant association with the patient knowledge. As limitations, we conducted the study using WHO patient care indicators only. The dispensers were also purposively selected for interview to explore the reasons for the inappropriate use of medicines.
Conclusions
The considerable number of participants at the outpatient pharmacy of JMC could not receive the prescribed medicines. On top of that, high percentages of drugs were handed over to patients without adequate labeling. The average dispensing and consultation times were too short for patients to understand the prescribed medications. The intervals of drug administration, dose, duration of therapy, and food-drug interaction were the most frequently delivered drug information to patients during consultations. However, the percentage of participants who knew the correct dosage regimen of the dispensed medicines was low. Generally, high prevalence of irrational use of medicines identified at Jimma Medical Center. The main reasons for misuse of drugs were identified to be high patient load, absence of monitoring and evaluation, lack of incentives, language barriers, and the patients’ health condition.
Footnotes
Acknowledgements
The authors would like to thank Jimma University for creating the opportunity to conduct this study. Our sincere gratitude also goes to the administrative staff of Jimma Medical Center for their kind cooperation.
Authors’ Note
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
TG reviewed articles, took part in data collection process, analyzed data, interpreted data, participated in the sequence alignment, drafted the manuscript and communicated for publication. DM reviewed articles, involved in the designing of the study, data collection process, data analysis, and interpretation. All the authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The authors received ethical approval from the institutional review board of Jimma University and a letter of permission from the School of Pharmacy. We used the ethical clearance and permission letter to communicate the concerned administrative staffs of the hospital.
Informed Consent
The participants were asked to sign consent form before starting the data collection.